Stroke
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"stroke" AND "epidemiology"
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have everything needed for a comprehensive overview. Let me compile the full response.
Stroke — Overview for Medical Students
Definition
A stroke (cerebrovascular accident) is defined as the abrupt onset of a neurologic deficit attributable to a vascular cause. The definition is clinical; brain imaging supports but does not make the diagnosis.
- Transient ischemic attack (TIA): all neurologic signs resolve within 24 h and no infarction on imaging
- Stroke: deficits persist >24 h or brain infarction is demonstrated
— Harrison's Principles of Internal Medicine, 22e
Epidemiology
- Second leading cause of death worldwide — 7.1 million deaths from stroke in 2020
- ~7 million Americans ≥20 years old have had a stroke; prevalence projected to rise by 3.4 million in the next decade (→ 4% of all adults)
- Age-standardized death rate has fallen ~15% over the past decade due to improved prevention and treatment
- Stroke remains the #1 cause of adult disability in the US; number one cause of acquired neurologic disability globally
— Harrison's, 22e
Classification: Two Major Types
1. Ischemic Stroke (~80–85%)
Caused by a reduction or cessation of blood flow to a brain region via:
| Mechanism | Description |
|---|---|
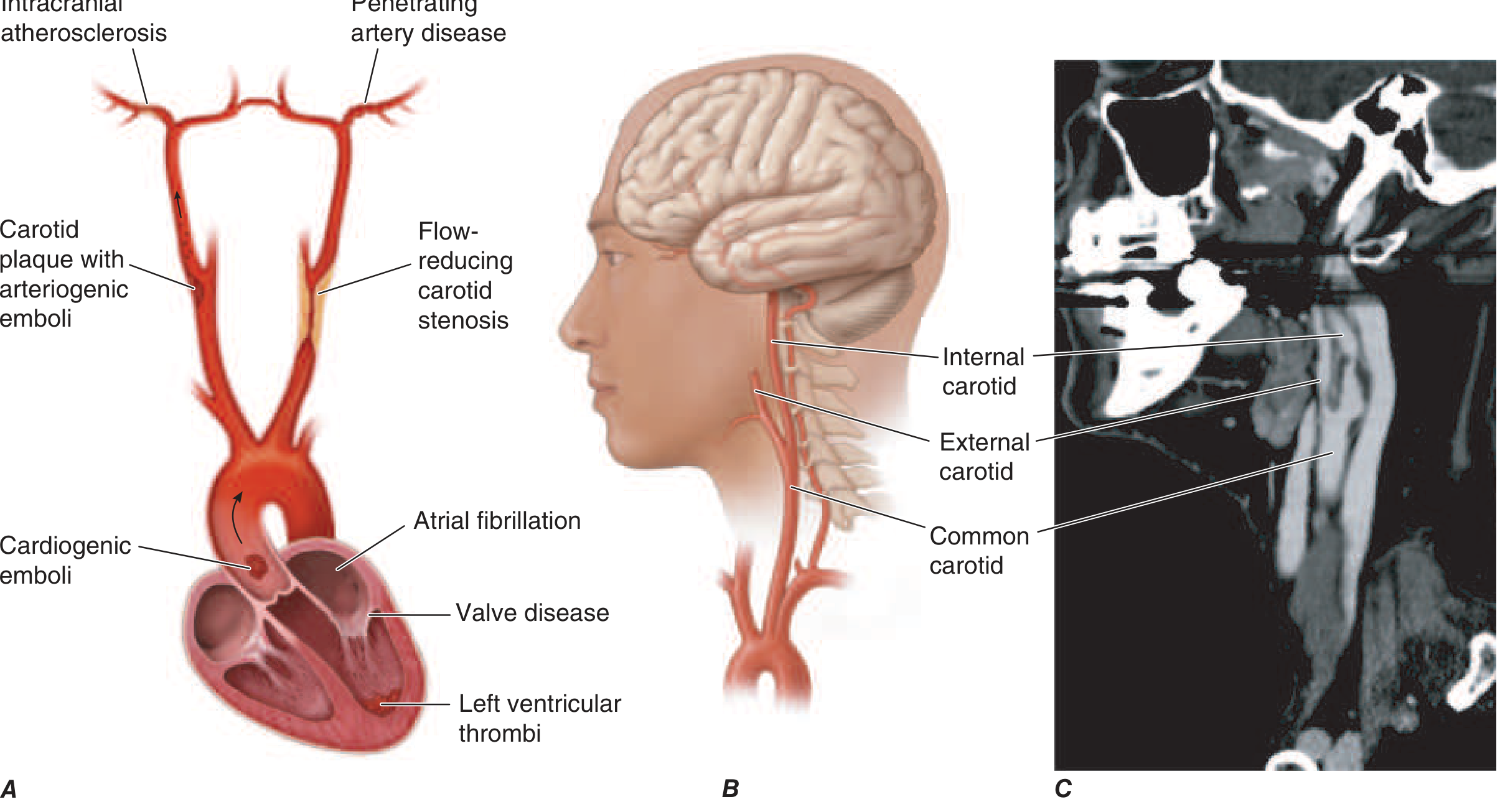
| Embolism | Clot travels from a proximal source (heart, aortic arch, carotid plaque) and occludes an intracranial artery |
| In situ thrombosis | Local thrombus in a cerebral vessel, typically in small penetrating arteries (lacunar) |
| Hypoperfusion | Flow-limiting stenosis causing watershed ischemia |
Etiologic subtypes (TOAST classification):
- Large-vessel atherothrombosis — carotid/vertebral/intracranial atherosclerosis
- Cardioembolic — atrial fibrillation (most common), valvular disease, LV thrombus, dilated cardiomyopathy
- Small-vessel (lacunar) — occlusion of single penetrating arteries, usually from lipohyalinosis due to hypertension/diabetes
- Cryptogenic — no source identified after full workup (~30%)
- Other determined cause — vasculitis, dissection, hypercoagulable states, Moyamoya, drug use
2. Hemorrhagic Stroke (~15–20%)
Divided into:
| Type | Key Features |
|---|---|
| Intracerebral hemorrhage (ICH) | Spontaneous bleeding into brain parenchyma; most commonly hypertensive; also amyloid angiopathy, AVMs, coagulopathy |
| Subarachnoid hemorrhage (SAH) | Bleeding into subarachnoid space; classic "thunderclap headache"; most often ruptured saccular aneurysm |
Pathophysiology of Ischemic Stroke
When cerebral blood flow (CBF) drops:
| CBF Level | Consequence |
|---|---|
| → 0 | Brain tissue death within 4–10 minutes |
| <16–18 mL/100g/min | Infarction within ~1 hour |
| <20 mL/100g/min | Ischemia without infarction (if not prolonged) |
Ischemic Core vs. Penumbra
- Ischemic core: irreversibly infarcted tissue at the center
- Ischemic penumbra: surrounding hypoperfused but potentially salvageable tissue — the target of reperfusion therapy
Cellular Cascade
- ↓ CBF → ↓ O₂/glucose → ↓ ATP → failure of Na⁺/K⁺-ATPase
- Neuronal depolarization → Na⁺/Ca²⁺ influx
- Glutamate release (excitotoxicity) → sustained NMDA receptor activation → ↑ intracellular Ca²⁺
- Reactive oxygen species (ROS) damage DNA, lipid membranes
- Microglial activation + peripheral immune cell infiltration → inflammatory injury
- Fever and hyperglycemia (>200 mg/dL) dramatically worsen injury
— Harrison's, 22e, Chapter 438
Pathophysiology of ICH
- Spontaneous ICH = bleeding directly into brain parenchyma
- Creates a mass effect on neural structures + direct neurotoxicity from blood breakdown products
- Most common cause: chronic hypertension → lipohyalinosis of small penetrating vessels (putamen, thalamus, cerebellum, pons most common sites)
- Second most common: cerebral amyloid angiopathy (lobar hemorrhages in elderly)
- Blood pressure management is key: AHA/ASA guidelines target SBP 130–150 mmHg acutely for spontaneous ICH with initial SBP 150–220 mmHg
Vascular Territories & Stroke Syndromes
Stroke syndromes are divided into anterior and posterior circulations:
Anterior Circulation (Internal Carotid → MCA/ACA)
| Vessel | Classic Syndrome |
|---|---|
| MCA (proximal) | Contralateral hemiplegia, hemisensory loss, hemianopia; dominant hemisphere → aphasia; non-dominant → neglect |
| MCA superior division | Face/arm > leg weakness + Broca's aphasia (if dominant) |
| MCA inferior division | Wernicke's aphasia + superior quadrantanopia (dominant) |
| ACA | Leg > arm weakness, abulia, urinary incontinence |
| ICA | Ipsilateral monocular blindness (amaurosis fugax) + MCA/ACA territory deficits |
Posterior Circulation (Vertebrobasilar)
| Vessel | Classic Syndrome |
|---|---|
| PCA | Contralateral homonymous hemianopia ± alexia without agraphia (left PCA) |
| Basilar artery | "Locked-in syndrome" (bilateral pontine infarct); quadriplegia, intact consciousness |
| PICA (Wallenberg) | Ipsilateral facial sensory loss, Horner's, dysphagia/dysarthria; contralateral limb hemianesthesia; vertigo, nausea |
| AICA | Ipsilateral facial weakness, hearing loss, vertigo, ataxia |
Small-Vessel (Lacunar) Syndromes
- Pure motor hemiplegia (posterior limb of internal capsule or pons)
- Pure sensory stroke (thalamus)
- Ataxic hemiparesis
- Dysarthria–clumsy hand
Risk Factors
| Modifiable | Non-modifiable |
|---|---|
| Hypertension (#1) | Age |
| Atrial fibrillation | Sex (male > female, though women have more lifetime strokes) |
| Diabetes mellitus | Race (Black > White > Asian for ICH) |
| Hyperlipidemia | Family history/genetics |
| Smoking | Prior stroke/TIA |
| Obesity, physical inactivity | |
| Carotid stenosis |
Key Points to Remember
- Time is brain — ~1.9 million neurons die per minute during a large-vessel occlusion
- Always CT first to exclude hemorrhage before any thrombolysis
- The ischemic penumbra is the therapeutic window — this is why door-to-needle time matters
- Atrial fibrillation is the single most important modifiable cardioembolic risk factor
- Lacunar infarcts are caused by small-vessel disease from HTN/DM, not emboli — so workup and treatment differ
- SAH presents with thunderclap headache ("worst headache of my life") — a clinical emergency requiring immediate imaging
Sources: Harrison's Principles of Internal Medicine, 22e (2025), Chapters 437, 438, 439 | Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.