Fate of thrombosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive answer. Here is the full breakdown:
Fate of Thrombosis
When a patient survives an initial thrombotic event, the thrombus evolves over the following days to weeks through one or more of four possible outcomes (Robbins & Kumar Basic Pathology, p. 91-92):
1. Propagation
The thrombus enlarges through continued accretion of additional platelets and fibrin. This increases the probability of:
- Complete vascular occlusion
- Embolization to distant sites
This is the most dangerous short-term outcome, particularly in deep venous thrombosis (DVT) where the thrombus may extend proximally toward the heart.
2. Embolization
Part or all of the thrombus detaches and is carried through the bloodstream to lodge elsewhere. Key points:
- Venous thrombi most commonly embolize to the pulmonary vasculature (pulmonary embolism), which can be fatal
- Arterial thrombi may embolize to the brain (stroke), gut, kidneys, or limbs
- DVTs in large leg veins at or above the knee (popliteal, femoral, iliac) are most prone to embolization
3. Dissolution (Fibrinolysis / Lysis)
If the thrombus is newly formed, activation of fibrinolytic factors (plasmin) may cause rapid shrinkage and complete dissolution. Important caveats:
- With older thrombi, extensive fibrin polymerization makes the clot substantially more resistant to plasmin-induced proteolysis - lysis becomes ineffective
- This is why thrombolytic agents (e.g., t-PA in acute coronary thrombosis) are only effective if given within a few hours of thrombus formation
- This window of susceptibility to lysis has major clinical significance for acute MI and stroke management
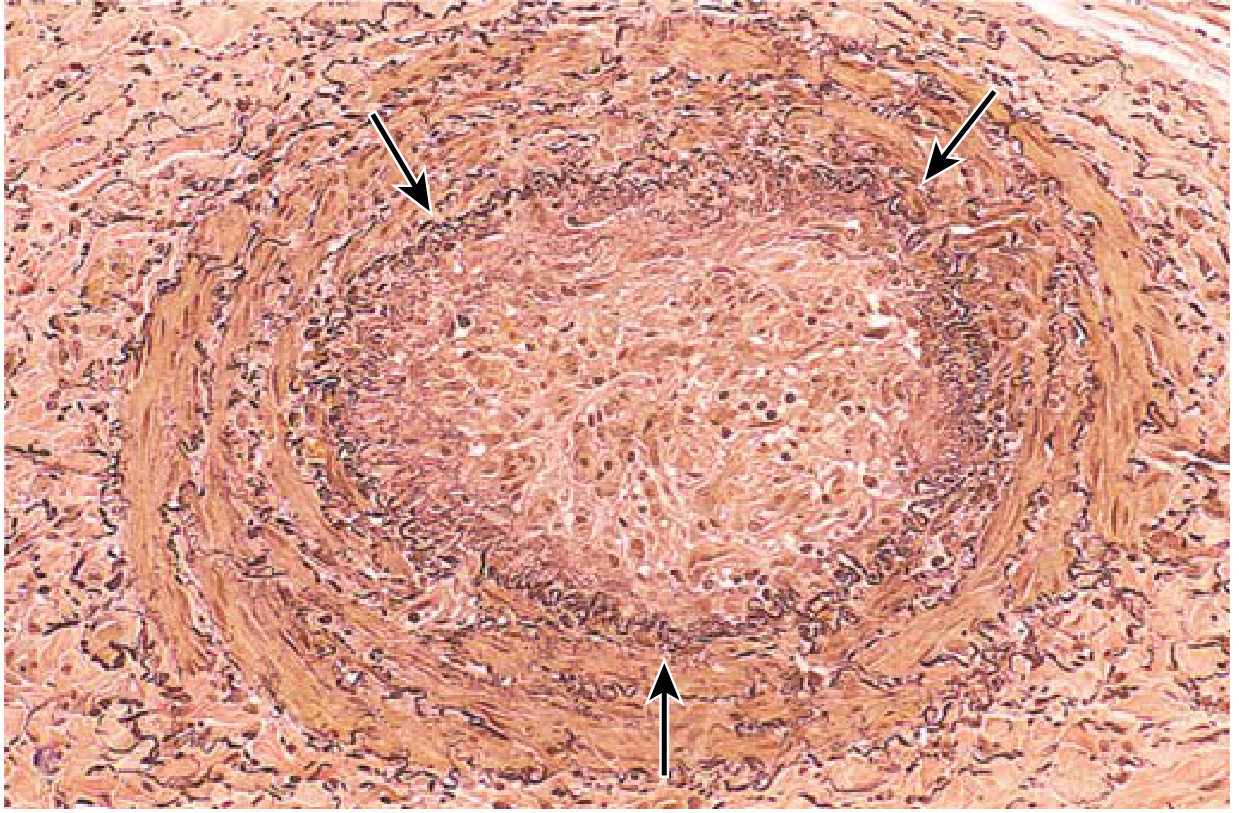
4. Organization and Recanalization
This is the outcome of older thrombi that are not dissolved or embolized:
- Organization: Ingrowth of endothelial cells, smooth muscle cells, and fibroblasts into the thrombus
- Recanalization: Capillary channels form along the length of the organized thrombus, partially restoring blood flow through the original lumen
- Over time, this can convert the thrombus into a vascularized mass of connective tissue that is incorporated into the vessel wall (see histology image below)
- Occasionally, instead of organizing, the center of a thrombus undergoes enzymatic digestion (liquefaction) due to lysosomal enzymes released from entrapped leukocytes
Summary Table
| Fate | Mechanism | Outcome |
|---|---|---|
| Propagation | Platelet/fibrin accretion | Worsening obstruction, embolism risk |
| Embolization | Detachment and downstream lodging | PE, stroke, infarction |
| Dissolution | Plasmin-mediated fibrinolysis | Complete resolution (only early thrombi) |
| Organization & Recanalization | Ingrowth of cells, capillary formation | Partial lumen restoration; wall incorporation |
| Enzymatic digestion | Leukocyte lysosomal enzymes | Central liquefaction of thrombus |
Clinical Relevance
- Venous thrombi (e.g., DVT): Main danger is embolization to the lungs. ~50% of DVTs are clinically silent until they embolize
- Arterial thrombi: Typically rich in platelets; main danger is local infarction (MI, stroke) rather than embolization
- Superficial venous thrombi: Rarely embolize; cause local pain, congestion, and varicose ulcers
- Vegetations: Thrombi on heart valves; can arise from infective endocarditis, nonbacterial thrombotic endocarditis, or Libman-Sacks endocarditis (SLE)
- Robbins & Kumar Basic Pathology, pp. 88-93
This is a shared conversation. Sign in to Orris to start your own chat.