Going to 1st clinicals for outside hospital just as 2nd year student without final for self experience but i knew nothing from any subject so help me to learn and main important things we also learn daily keep this and remaind me but main things alll I need to learn
Reading File
Asking for Preferences
Finding Sources
Searching the Web
2nd year MBBS clinical posting survival guide important topics ward skills
Finding Sources
Finding Sources
Reading Web Page
https://gmch.gov.in/sites/default/files/documents/Student_Le…
Finding Sources
Finding Sources
I now have enough from the library structure and curriculum documents to build you a thorough, structured guide. Here it is:
🏥 Your 2nd Year Clinical Survival Guide
"Starting from Zero" - Everything You Need for Your First Hospital Posting
PART 1 - THE MINDSET FIRST
You are NOT expected to know everything. You are there to observe, assist, and learn. Nobody will fail you for not knowing a drug dose on Day 1. What matters is:
- You show up every day
- You watch and ask questions
- You write things down and look them up that night
- You keep this guide updated as you learn new things
PART 2 - THE 5 THINGS YOU NEED ON DAY 1
Before anything clinical, have these ready every single day:
| Item | Why |
|---|---|
| Small pocket notebook | Write every new thing you see or hear |
| Pen torch (penlight) | Pupil reflex, throat, ear |
| Stethoscope | Always around your neck |
| Your white coat | Clean, name badge on |
| This guide open on your phone | Reference everything here |
PART 3 - THE MOST IMPORTANT SKILL - HISTORY TAKING (SOCRATES + SYSTEM)
Every patient encounter starts with history. This is the #1 skill in all departments.
The Universal History Format (use this for EVERY patient)
1. Chief Complaint (CC)
- "What brought you to hospital today?" - in patient's own words
- Write it as: "Fever for 3 days" or "Chest pain since morning"
2. History of Present Illness (HPI) - use SOCRATES for any symptom:
| Letter | Question to ask |
|---|---|
| S - Site | Where exactly is it? |
| O - Onset | When did it start? Sudden or gradual? |
| C - Character | What does it feel like? (sharp, dull, burning, crushing) |
| R - Radiation | Does it go anywhere else? |
| A - Associations | Any other symptoms along with this? |
| T - Timing | Constant or comes and goes? How long each time? |
| E - Exacerbating/Relieving | What makes it worse? What makes it better? |
| S - Severity | Score on 1-10? |
3. Past Medical History (PMH)
- Any previous hospital admissions?
- Hypertension / Diabetes / Asthma / TB / Heart disease?
- Any previous surgeries?
4. Drug History
- Current medications? Dosage?
- Any allergies? (especially drug allergies - ask this EVERY time)
5. Family History
- Parents/siblings with similar illness?
- Diabetes, hypertension, cancer in family?
6. Social History
- Smoking (pack-years = packs/day x years smoked)
- Alcohol (units/week)
- Occupation
- Living conditions (for infectious diseases)
7. Review of Systems (ROS)
- Go through each system briefly: any cough? bowel issues? urinary symptoms? etc.
PART 4 - GENERAL EXAMINATION (What to check on EVERY patient)
The 4 Vitals - Check These First, Every Time
| Vital | Normal Range | How to check |
|---|---|---|
| Temperature | 36.5-37.5°C (oral) | Thermometer |
| Pulse | 60-100 bpm | Radial artery, 15 sec x 4 |
| Blood Pressure | 120/80 mmHg | Sphygmomanometer, right arm seated |
| Respiratory Rate | 12-20/min | Count chest rises for 30 sec x 2 |
| SpO2 | >95% | Pulse oximeter |
General Appearance - Look at the patient from the foot of the bed:
- Conscious? Alert? Confused?
- Comfortable or in distress?
- Pale, jaundiced, cyanosed?
- Well-nourished or malnourished?
Hands (examine first):
- Nails: clubbing, pallor (anemia), koilonychia, leukonychia
- Palms: palmar erythema, Dupuytren's contracture
- Pulse: rate, rhythm, character, volume
Eyes:
- Conjunctival pallor = anemia
- Scleral icterus = jaundice
- Xanthelasma = hyperlipidemia
Mouth:
- Central cyanosis (blue tongue) = hypoxia
- Tongue: smooth tongue = iron/B12 deficiency
Lymph nodes: always check neck, axilla, groin
Edema: press shin for 5 seconds - pitting or non-pitting?
PART 5 - SYSTEM-BY-SYSTEM QUICK GUIDES
🫀 CARDIOVASCULAR (Heart)
Key symptoms to look for: Chest pain, breathlessness (dyspnea), palpitations, ankle swelling, syncope (fainting)
Examination sequence:
- Inspect: Visible pulsations, scars from surgery
- JVP (Jugular Venous Pressure): look at neck veins, raised in heart failure
- Palpate: Apex beat (normally 5th intercostal space, midclavicular line)
- Auscultate with stethoscope - 4 areas:
- Aortic: 2nd right intercostal space
- Pulmonary: 2nd left intercostal space
- Tricuspid: left lower sternal border
- Mitral: apex (5th ICS, MCL)
Normal heart sounds: S1 (lub) = mitral/tricuspid closing, S2 (dub) = aortic/pulmonary closing
Common conditions you'll see:
- Heart Failure: breathlessness, bilateral leg edema, raised JVP, basal crackles
- Hypertension: often found by chance, check BP both arms
- MI (Heart Attack): crushing central chest pain radiating to left arm/jaw, diaphoresis (sweating)
🫁 RESPIRATORY (Lungs)
Key symptoms: Cough, sputum (color matters), breathlessness, chest pain (pleuritic = worse on breathing), hemoptysis (coughing blood), fever
Sputum color guide:
- White/clear = viral, asthma
- Yellow/green = bacterial infection
- Rusty = pneumonia (lobar)
- Pink frothy = pulmonary edema
- Blood-stained = TB, cancer, PE
Examination sequence:
- Inspect: Rate, work of breathing, use of accessory muscles, shape of chest
- Tracheal position (normally midline - pushed away in effusion, pulled toward in collapse)
- Expansion: Hands on chest - equal movement?
- Percussion: Resonant (normal air), Dull (fluid/consolidation), Hyperresonant (pneumothorax)
- Auscultation: Vesicular (normal), Bronchial (consolidation), Added sounds:
- Crackles/crepitations = fluid (pneumonia, CCF)
- Wheeze = airway narrowing (asthma, COPD)
- Pleural rub = pleuritis
Common conditions:
- Pneumonia: fever, cough, purulent sputum, dullness to percussion, bronchial breath sounds
- Asthma: wheeze, breathlessness, chest tightness, worse at night/with triggers
- TB: chronic cough >3 weeks, fever, night sweats, weight loss, hemoptysis
🫃 ABDOMEN (GI)
Key symptoms: Abdominal pain (use SOCRATES), nausea/vomiting, diarrhea/constipation, jaundice, blood in stool
Examination sequence - IAPP (Inspect, Auscultate, Percuss, Palpate - in this order for abdomen!):
- Inspect: Distension, scars, visible veins (caput medusae = portal hypertension), pulsations
- Auscultate FIRST (before palpating, otherwise bowel sounds change): Normal = gurgling every 5-10 sec; Absent = ileus/peritonitis; Tinkling = obstruction
- Percuss: Liver dullness (right side), spleen dullness (left), shifting dullness = ascites
- Palpate: Light then deep, watch patient's face for pain
- Liver: start from right iliac fossa, move up
- Spleen: start from right iliac fossa toward left hypochondrium
- Renal angles: punch tenderness = kidney infection
- Special signs: Murphy's (cholecystitis), McBurney's (appendicitis), Rovsing's (appendicitis)
Jaundice quick classification:
| Type | Cause | Clue |
|---|---|---|
| Pre-hepatic | Hemolysis | Dark urine, pale stools... wait no - NO bilirubin in urine |
| Hepatic | Liver disease | All abnormal |
| Post-hepatic (Obstructive) | Bile duct blockage | Dark urine + pale/clay stools + itch |
🧠 NEUROLOGY
Consciousness: use GCS (Glasgow Coma Scale)
| Component | Score |
|---|---|
| Eye opening: Spontaneous/To voice/To pain/None | 4/3/2/1 |
| Verbal: Oriented/Confused/Words/Sounds/None | 5/4/3/2/1 |
| Motor: Obeys/Localizes/Withdraws/Flexion/Extension/None | 6/5/4/3/2/1 |
| Maximum | 15 (normal) |
| Minimum | 3 |
| Coma | ≤8 |
Mini mental status: Ask patient - What is today's date? What year is it? Where are you? Count backwards from 100 by 7s.
Cranial nerves (quick test):
- CN II: Visual acuity (read a chart)
- CN III/IV/VI: Eye movements ("follow my finger" - H pattern)
- CN V: Facial sensation
- CN VII: "Show your teeth, close your eyes tight, raise your eyebrows"
- CN IX/X: "Say ahh" - uvula midline?
- CN XII: Tongue out - midline?
Motor exam - 5 things:
- Tone: passive movement of limb - normal/hypertonia/hypotonia
- Power: grade 0-5 (0=no movement, 3=against gravity, 5=full normal)
- Reflexes: use tendon hammer - knee jerk (L3/4), ankle jerk (S1), biceps (C5/6)
- Sensation: light touch, pinprick
- Coordination: finger-nose test, heel-shin test
🍼 PEDIATRICS (Children)
Key difference: everything is age-based
Developmental milestones to remember:
| Age | Motor | Social/Language |
|---|---|---|
| 3 months | Holds head up | Social smile |
| 6 months | Sits with support | Babbles |
| 9 months | Stands with support | Says mama/dada |
| 12 months | Walks alone | 1-2 words with meaning |
| 18 months | Runs | 10+ words |
| 2 years | Climbs stairs | 2-word sentences |
Pediatric vitals (vary with age):
| Age | Normal HR | Normal RR |
|---|---|---|
| Newborn | 100-160 | 40-60 |
| 1-5 years | 80-120 | 20-30 |
| 6-12 years | 70-110 | 15-20 |
Immunization - must know:
- BCG: at birth (against TB)
- OPV + IPV: at birth, 6, 10, 14 weeks (polio)
- DTP (Penta): 6, 10, 14 weeks (diphtheria, tetanus, pertussis)
- MMR: 9-12 months (measles, mumps, rubella)
👶 OBSTETRICS & GYNECOLOGY (OBG)
Obstetric History Format (in addition to standard history):
- G_P_A_ : Gravida (total pregnancies), Para (deliveries >28 wks), Abortion (<28 wks)
- LMP (Last Menstrual Period) - to calculate gestational age and EDD
- EDD (Expected Date of Delivery) = LMP + 9 months + 7 days (Naegele's rule)
Antenatal (ANC) Checkup basics:
- Blood pressure every visit (watch for preeclampsia - BP >140/90 after 20 weeks)
- Fundal height = gestational age in weeks (roughly)
- Fetal heart sounds: normal 110-160 bpm
Obstetric emergencies to recognize (shout for senior help immediately):
- Eclampsia: seizures in pregnancy - give MgSO4
- PPH (Postpartum Hemorrhage): >500mL blood loss after delivery
- Cord prolapse: cord visible at vagina - emergency C-section
PART 6 - IMPORTANT INVESTIGATIONS (Lab Values to Know)
CBC (Complete Blood Count)
| Test | Normal Range | Abnormal means |
|---|---|---|
| Hemoglobin (Hb) | Men: 13-17 g/dL, Women: 12-15 g/dL | Low = anemia |
| WBC (White cells) | 4,000-11,000 /μL | High = infection/leukemia |
| Neutrophils | 40-70% | High = bacterial infection |
| Lymphocytes | 20-40% | High = viral infection |
| Platelets | 1,50,000-4,00,000 /μL | Low = dengue, ITP |
LFT (Liver Function Tests)
| Test | Normal |
|---|---|
| Total Bilirubin | 0.3-1.2 mg/dL |
| AST/ALT (transaminases) | <40 U/L |
| ALP | 44-147 U/L |
| Albumin | 3.5-5.0 g/dL |
| PT/INR | 0.9-1.1 |
KFT (Kidney Function Tests)
| Test | Normal |
|---|---|
| Serum Creatinine | 0.6-1.2 mg/dL |
| Blood Urea Nitrogen | 7-20 mg/dL |
| Serum Sodium | 136-145 mEq/L |
| Serum Potassium | 3.5-5.0 mEq/L |
RBS/FBS (Blood Sugar)
| Test | Normal | Diabetes |
|---|---|---|
| Fasting | <100 mg/dL | >126 mg/dL |
| Random (RBS) | <140 mg/dL | >200 mg/dL |
| HbA1c | <5.7% | >6.5% |
PART 7 - COMMON DRUGS YOU'LL SEE ON PRESCRIPTIONS
| Drug | For | Route | Remember |
|---|---|---|---|
| Paracetamol | Fever/pain | Oral/IV | Max 4g/day, safe in pregnancy |
| Ibuprofen (NSAIDs) | Pain/inflammation | Oral | Avoid in renal failure, gastric ulcer |
| Amoxicillin | Bacterial infections | Oral | Check penicillin allergy |
| Metformin | Type 2 Diabetes | Oral | Hold before contrast dye |
| Amlodipine | Hypertension | Oral | Ankle edema is side effect |
| Atorvastatin | High cholesterol | Oral | Give at night |
| Furosemide | Edema/fluid overload | Oral/IV | Loops lose potassium |
| Metronidazole | Anaerobic infections | Oral/IV | No alcohol! |
| Ondansetron | Nausea/vomiting | Oral/IV | QT prolongation concern |
| Omeprazole | Stomach protection/ulcers | Oral | Give before meals |
PART 8 - WARD PRACTICAL SKILLS (Watch First, Then Practice)
These are the skills done in the ward. Watch seniors do each one 3 times before attempting:
Basic skills (you will assist with these):
- IV cannulation - insert IV line into vein
- Blood sample collection (venipuncture)
- ABG (Arterial Blood Gas) - for respiratory patients
- Urine catheter insertion (Foley's)
- NG (Nasogastric) tube insertion
- Measuring blood pressure manually
- Reading ECG (electrocardiogram) - see below
ECG Reading - 5-Step Approach
- Rate: Count big squares between two R waves, divide 300 by that number. Normal 60-100 bpm.
- Rhythm: Regular or irregular? P wave before every QRS?
- Axis: Normal = -30° to +90°
- P waves: Present? Normal shape?
- QRS + ST changes: Look for ST elevation (STEMI), ST depression (ischemia), Q waves (old MI), widened QRS (bundle branch block)
Normal ECG intervals:
- PR interval: 0.12-0.20 sec (one big square)
- QRS: <0.12 sec (3 small squares)
- QT: <0.44 sec (adjusted for rate)
PART 9 - HOW TO PRESENT A CASE (On Ward Rounds)
This is what you say when the doctor asks you to present your patient. Practice this format every day:
"This is [Mr/Mrs X], a [age]-year-old [male/female] who presented with [chief complaint] for [duration]. On history, [relevant positives and negatives]. On examination, vitals are [state vitals]. General examination revealed [findings]. Systemic examination of [relevant system] showed [findings]. Investigations showed [key results]. My impression is [diagnosis/differential]. The patient is currently on [treatment]."
Keep it under 2 minutes. State the most important findings first.
PART 10 - YOUR DAILY LEARNING ROUTINE (Do This Every Day)
Morning (Before Ward Rounds)
- Review the patients you are following from yesterday
- Look up ONE topic from yesterday that you didn't understand
- Know your patients' vitals from the nursing chart before rounds
During Ward Rounds
- Stand where you can see and hear clearly
- Write every unfamiliar term in your notebook
- Note what questions the senior doctor asks the patient
- Ask "What does that finding mean?" when you have a moment
Evening (After Posting)
- Pick ONE new topic you encountered today
- Read about it for 20-30 minutes from your textbook or notes
- Write a 5-line summary of what you learned
- Ask me (Orris) to explain anything you still don't understand
PART 11 - DAILY TOPIC SCHEDULE (2-Week Rotation Starter)
| Day | Topic | Department |
|---|---|---|
| Day 1 | History taking + SOCRATES | Any |
| Day 2 | Vitals + General examination | Any |
| Day 3 | CVS examination + Heart failure | Medicine |
| Day 4 | ECG basics | Medicine/Cardiology |
| Day 5 | Respiratory examination + Pneumonia | Medicine |
| Day 6 | Abdominal examination + Jaundice | Medicine/Surgery |
| Day 7 | Blood investigations (CBC, LFT, KFT, RBS) | Any |
| Day 8 | Surgical ward - wound care, drains, IV fluids | Surgery |
| Day 9 | Pediatric history + Developmental milestones | Pediatrics |
| Day 10 | Immunization + Pediatric emergencies | Pediatrics |
| Day 11 | Obstetric history + ANC | OBG |
| Day 12 | Common drugs + prescription reading | Pharmacology/Any |
| Day 13 | Neurology exam + GCS | Medicine/Neurology |
| Day 14 | Case presentation practice | Any |
PART 12 - EMERGENCY SIGNS - CALL FOR HELP IMMEDIATELY
If you see ANY of these, immediately call your senior resident or attending:
🚨 ABCDE danger signs:
- Airway: patient unable to speak/gurgling sounds
- Breathing: RR >30 or <8, SpO2 <90%, severe labored breathing
- Circulation: BP <90/60, HR >130 or <40, cold clammy skin
- Disability: GCS dropping, new-onset seizure, unequal pupils
- Exposure: high fever >40°C, massive bleeding
HOW TO USE THIS GUIDE GOING FORWARD
Each day, come back to me with:
- What department you're in
- One condition or case you saw
- One question you couldn't answer
I will give you:
- A focused explanation of that condition
- What to look for on examination
- What questions might be asked about it
- A 3-5 line summary to add to your notes
This guide grows with you every day. You are starting from zero today - that is completely okay. By the end of your rotations, you will know enough to handle any ward confidently.
You've got this. See you tomorrow with your Day 1 questions.
Cardiac
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Great - I have solid textbook content from Fuster & Hurst's The Heart and Goldman-Cecil Medicine. Here is your full Cardiac module:
❤️ CARDIAC MODULE - Complete Clinical Guide
For 2nd Year Students on Cardiology/Medicine Posting
SECTION 1 - CARDIAC HISTORY TAKING
When a patient comes with a cardiac complaint, always ask these specific questions on top of the standard SOCRATES:
5 Key Cardiac Symptoms
| Symptom | Ask This |
|---|---|
| Chest pain | Where? Left/central? Radiation to arm/jaw? Crushing or sharp? Worse on exertion? |
| Dyspnea | On exertion or at rest? How many pillows to sleep? (orthopnea) Woken up at night gasping? (PND) |
| Palpitations | Fast or slow? Regular or irregular? How long? Associated dizziness? |
| Syncope | Any warning? During exertion or at rest? Full loss of consciousness? |
| Edema | Ankle swelling? Both legs? How long? Getting worse? |
Special cardiac history questions:
- Rheumatic fever as a child? (causes valvular disease)
- Family history of sudden cardiac death or early heart disease?
- Smoking, diabetes, hypertension, high cholesterol? (risk factors)
- Previous heart attack or stents?
SECTION 2 - CARDIOVASCULAR EXAMINATION (Step-by-Step)
THE SEQUENCE: Inspect → Palpate → Percuss → Auscultate
STEP 1 - HANDS (Start here always)
| Finding | What it means |
|---|---|
| Clubbing | Cyanotic congenital heart disease, infective endocarditis |
| Splinter hemorrhages (nails) | Infective endocarditis |
| Osler's nodes (painful lumps on fingers) | Infective endocarditis |
| Janeway lesions (painless on palms) | Infective endocarditis |
| Peripheral cyanosis (blue fingers) | Low cardiac output |
| Xanthomas (fatty deposits on tendons) | High cholesterol |
Pulse - 6 things to check:
- Rate - count for 15 sec x 4 (normal 60-100 bpm)
- Rhythm - regular or irregular? (irregular = AF - atrial fibrillation)
- Character - normal / bounding (aortic regurgitation) / weak/thready (shock) / collapsing (AR)
- Volume - normal / increased / decreased
- Radio-radial delay - feel both wrists together (delay = aortic dissection, coarctation)
- Radio-femoral delay - feel wrist + groin simultaneously (delay = coarctation of aorta)
STEP 2 - BLOOD PRESSURE
- Measure both arms (difference >15 mmHg = subclavian stenosis or aortic dissection)
- Normal: <120/80 mmHg
- Hypertension: ≥140/90 mmHg
- Pulse pressure = Systolic - Diastolic (normal ~40 mmHg)
- Wide pulse pressure (>60) = aortic regurgitation, thyrotoxicosis
- Narrow pulse pressure (<25) = aortic stenosis, cardiac tamponade
STEP 3 - FACE & EYES
| Finding | Condition |
|---|---|
| Malar flush (red cheeks) | Mitral stenosis |
| Central cyanosis (blue tongue/lips) | Right-to-left shunt, severe heart failure |
| Xanthelasma (yellow deposits around eyes) | Hypercholesterolemia |
| High-arched palate + tall build | Marfan syndrome (aortic root disease) |
STEP 4 - JVP (Jugular Venous Pressure)
Why it matters: JVP reflects the pressure in the right side of the heart. Raised JVP = fluid overload / right heart failure.
How to assess:
- Patient at 45 degrees, head turned slightly left
- Look at the right side of the neck - find the internal jugular vein (not the carotid - JVP has 2 waves, is non-pulsatile, and goes away when you press on it)
- Normal = top of pulsation <4 cm above sternal angle
Raised JVP seen in:
- Right heart failure
- Cardiac tamponade (with pulsus paradoxus)
- Superior vena cava obstruction
- Fluid overload
STEP 5 - PRAECORDIUM (Chest)
Inspect:
- Scars: midline sternotomy scar = bypass surgery; left lateral = mitral valve surgery
- Visible pulsations: apex beat visible? Heaves?
Palpate:
- Apex beat: Normally at 5th intercostal space, midclavicular line
- Displaced outward/downward = cardiomegaly (heart failure, dilated cardiomyopathy)
- Tapping quality = mitral stenosis
- Heaving/thrusting = left ventricular hypertrophy (hypertension, aortic stenosis)
- Parasternal heave: Place palm on left sternal border - heave felt = right ventricular enlargement
- Thrills: Palpable vibration = severe murmur present (like feeling a cat purr)
STEP 6 - AUSCULTATION (The most important step)
4 areas to listen - in this order:
2nd Right ICS = AORTIC area (A)
2nd Left ICS = PULMONARY area (P)
Left sternal border = TRICUSPID area (T)
5th ICS, MCL = MITRAL/Apex area (M)
Normal heart sounds:
- S1 (lub) = mitral + tricuspid valves CLOSING at start of systole
- S2 (dub) = aortic + pulmonary valves CLOSING at end of systole
- Listen: lub-DUB ... lub-DUB (S2 louder at base)
Extra sounds:
- S3 (lub-dub-ta): heard after S2, at apex - sign of heart FAILURE (volume overload)
- S4 (ta-lub-dub): heard before S1, at apex - sign of STIFF ventricle (hypertension, LVH)
Murmurs - GRADE them (Levine scale 1-6):
| Grade | Description |
|---|---|
| 1 | Very faint, only with concentration |
| 2 | Faint but heard immediately |
| 3 | Moderate, no thrill |
| 4 | Loud with thrill |
| 5 | Very loud, heard with stethoscope partly off chest |
| 6 | Heard without stethoscope |
COMMON MURMURS TO KNOW
| Murmur | Type | Area | Radiation | Pitch | Mnemonic |
|---|---|---|---|---|---|
| Aortic Stenosis | Systolic (ejection) | Aortic area | To neck/carotids | Harsh, crescendo-decrescendo | "AS radiates to neck" |
| Aortic Regurgitation | Diastolic | Aortic area | Left sternal border | Soft, blowing, early diastolic | "AR = diastolic at left sternal border" |
| Mitral Stenosis | Diastolic | Apex | None | Rumbling, low-pitched, mid-diastolic | "MS = rumble at apex" |
| Mitral Regurgitation | Systolic (pansystolic) | Apex | To axilla | Blowing, pansystolic | "MR blows to armpit" |
Quick rule: Systolic murmur = between S1 and S2. Diastolic murmur = between S2 and next S1.
STEP 7 - LUNGS (always do this after cardiac exam)
- Basal crackles (crepitations) at both lung bases = pulmonary edema from left heart failure
- Pleural effusion (stony dullness, absent breath sounds) = can be from heart failure
STEP 8 - ABDOMEN & LEGS
- Hepatomegaly (enlarged liver): right heart failure causes liver congestion - tender liver
- Ascites: right heart failure (shifting dullness)
- Pitting edema: press shin/ankle for 5 seconds - indentation = pitting edema from heart failure, hypoalbuminemia
SECTION 3 - MOST COMMON CONDITIONS YOU'LL SEE
1. HEART FAILURE
Simple definition: The heart cannot pump enough blood to meet the body's needs.
Two types:
| HFrEF (Reduced EF) | HFpEF (Preserved EF) | |
|---|---|---|
| EF | <40% | >50% |
| Problem | Weak pump | Stiff pump |
| Common cause | MI, dilated cardiomyopathy | Hypertension, diabetes, obesity |
Symptoms - split by sided failure:
| Left Heart Failure | Right Heart Failure |
|---|---|
| Dyspnea on exertion | Ankle/leg edema |
| Orthopnea (can't lie flat) | Raised JVP |
| PND (woken at night gasping) | Tender hepatomegaly |
| Basal lung crackles | Ascites |
| Frothy pink sputum (severe) |
Investigations:
- ECG: may show LVH, old MI, arrhythmia
- Chest X-Ray (CXR): look for ABCDE:
- A - Alveolar edema (bat-wing shadowing)
- B - Kerley B lines (horizontal lines at bases)
- C - Cardiomegaly (CTR >0.5)
- D - Dilated upper lobe veins
- E - Effusion (pleural)
- BNP/NT-proBNP: elevated in heart failure (best marker)
- Echo (TTE): measures ejection fraction - the GOLD STANDARD test
Here is the full heart failure overview from Fuster & Hurst's The Heart (2024):
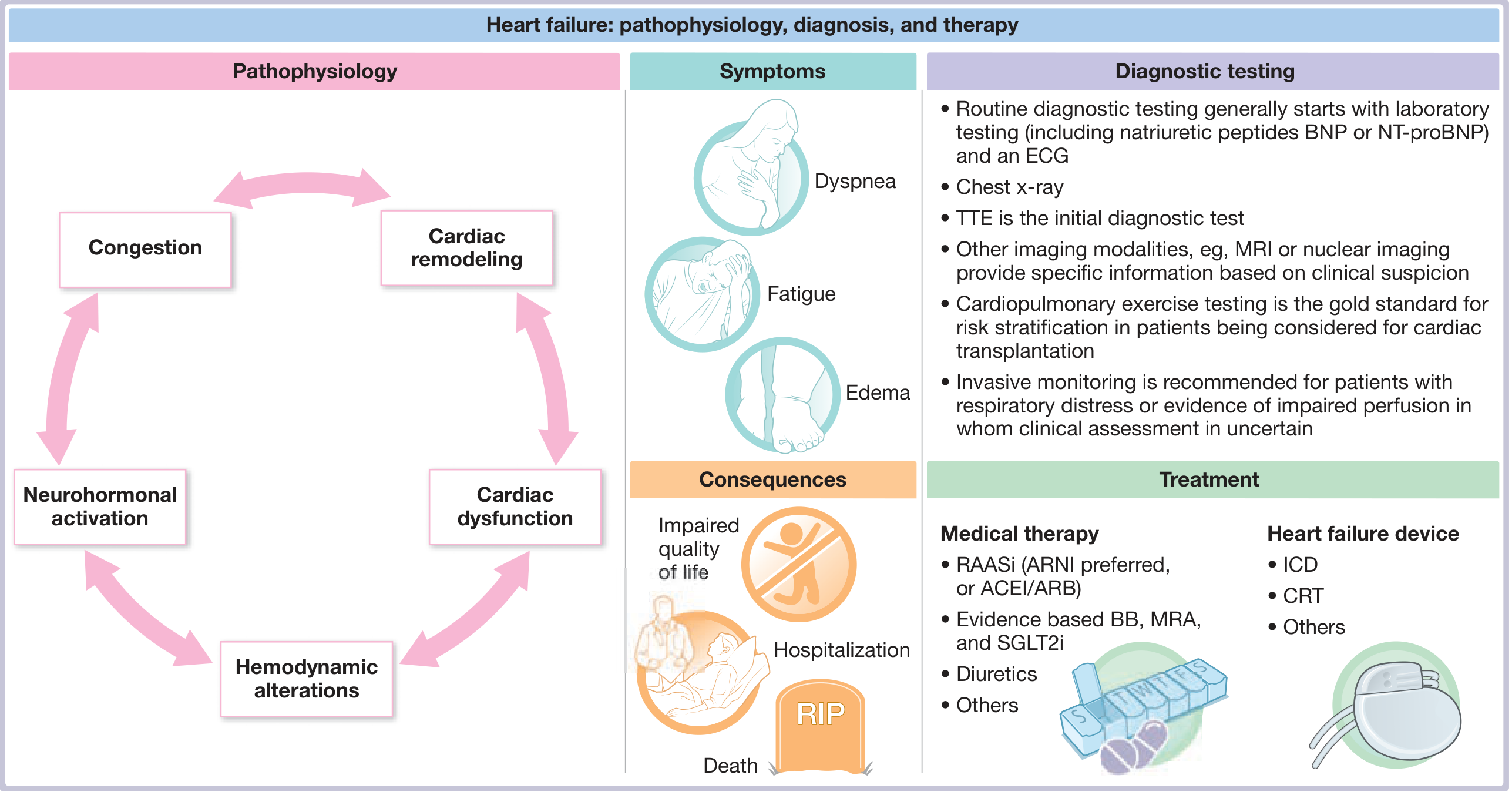
Treatment of Heart Failure (HFrEF) - "BADS" drugs:
| Drug class | Example | Why given |
|---|---|---|
| Beta-blocker | Carvedilol, Metoprolol | Reduces mortality, slows heart |
| ACEi / ARB / ARNI | Ramipril / Sacubitril-Valsartan | Reduces remodeling, mortality |
| Diuretic | Furosemide | Relieves congestion/edema |
| SGLT2 inhibitor | Dapagliflozin, Empagliflozin | New - reduces hospitalization |
| Spironolactone (MRA) | Spironolactone | Reduces mortality |
2. HYPERTENSION
Definition: BP ≥140/90 mmHg on two separate readings
Classification:
| Category | Systolic | Diastolic |
|---|---|---|
| Normal | <120 | <80 |
| Elevated | 120-129 | <80 |
| Stage 1 HTN | 130-139 | 80-89 |
| Stage 2 HTN | ≥140 | ≥90 |
| Hypertensive Crisis | >180 | >120 |
95% of hypertension = Primary/Essential (no identifiable cause - lifestyle related)
5% = Secondary - think of this in young patients or resistant HTN:
- Renal artery stenosis
- Pheochromocytoma (episodic headache, sweating, palpitations)
- Hyperaldosteronism (low potassium + high BP)
- Coarctation of aorta
Complications (target organ damage) - "HEADS":
- Heart: LVH, heart failure, IHD
- Eyes: hypertensive retinopathy (papilledema, AV nipping, flame hemorrhages)
- Aorta: dissection
- Deep kidneys: proteinuria, CKD
- Stroke/brain: hemorrhagic stroke, hypertensive encephalopathy
First-line drugs:
- Young patient: ACE inhibitor (Ramipril 2.5-10mg OD)
- Elderly/African: Calcium channel blocker (Amlodipine 5-10mg OD)
- With fluid overload: Thiazide diuretic (Hydrochlorothiazide 12.5-25mg OD)
3. ISCHEMIC HEART DISEASE (IHD) / ANGINA / MI
Spectrum:
Stable Angina → Unstable Angina → NSTEMI → STEMI
(chronic) (ACS - Acute Coronary Syndrome)
Stable Angina: Chest pain on exertion, relieved by rest or GTN spray in <5 min. Fixed coronary narrowing.
ACS (Acute Coronary Syndrome): Chest pain at REST or with minimal exertion. Plaque rupture + clot.
Classic MI presentation:
- Sudden severe crushing/squeezing central chest pain
- Radiation to left arm, jaw, neck, back
- Sweating (diaphoresis), nausea, vomiting
- Breathlessness
- Sense of doom
- Note: Diabetics and elderly can have SILENT MI (no pain - just breathlessness, fatigue)
ECG changes in MI:
| Stage | ECG Finding |
|---|---|
| Hyperacute (minutes) | Tall peaked T waves |
| Acute (hours) | ST elevation (STEMI) |
| Evolving (hours-days) | T wave inversion |
| Old (days-weeks) | Pathological Q waves (>0.04 sec, >25% of R) |
Territory by lead:
| Leads with changes | Territory | Artery |
|---|---|---|
| II, III, aVF | Inferior | RCA |
| V1-V4 | Anterior | LAD |
| I, aVL, V5-V6 | Lateral | LCx |
STEMI management (time = muscle):
- MONA (old mnemonic, still useful to know):
- Morphine (for pain)
- Oxygen (if SpO2 <94%)
- Nitrates (GTN) - sublingual
- Aspirin 300mg (chewed, not swallowed)
- Dual antiplatelet: Aspirin + Clopidogrel (or Ticagrelor)
- Reperfusion within 90 min: Primary PCI (angioplasty + stent) is GOLD STANDARD. If not available: thrombolysis (streptokinase or tPA)
- Anticoagulation: Heparin
- Long-term: Beta-blocker + ACEi + Statin + Dual antiplatelets
4. ATRIAL FIBRILLATION (AF)
The most common sustained cardiac arrhythmia.
Definition: Chaotic, disorganized atrial activity. No P waves on ECG. Irregularly irregular pulse.
How to recognize on ECG:
- No visible P waves (replaced by fibrillatory baseline - wavy line)
- Irregularly irregular QRS complexes
- Ventricular rate usually fast (100-180 bpm) if uncontrolled
Causes ("PIRATES"):
- Pulmonary (PE, pneumonia)
- Ischaemia (MI)
- Rheumatic heart disease
- Alcohol / thyrotoxicosis
- Thyroid (hyperthyroidism - very common cause)
- Electrolytes (low K/Mg)
- Sepsis / surgery
Risk from AF: Blood pools in atria → clot forms → clot travels to brain = STROKE
Treatment:
- Rate control: Beta-blocker (metoprolol) or Digoxin
- Rhythm control: Cardioversion (electrical or chemical with amiodarone)
- Anticoagulation to prevent stroke: Warfarin or DOACs (apixaban, rivaroxaban) - based on CHA₂DS₂-VASc score
SECTION 4 - ECG INTERPRETATION (Step-by-Step System)
Always follow the same 7 steps - every single ECG:
Step 1 - Check the basics
- Patient name, date, speed (25 mm/sec standard), calibration (1mV = 10mm)
Step 2 - Rate
- Regular rhythm: 300 ÷ number of large squares between R waves
- Irregular: count QRS complexes in 10-second strip × 6
Step 3 - Rhythm
- Is it regular or irregular?
- Is there a P wave before every QRS?
- Regular + P before every QRS = sinus rhythm ✓
Step 4 - Axis
| Leads I & aVF | Axis |
|---|---|
| Both positive | Normal (-30° to +90°) |
| I positive, aVF negative | Left axis deviation (LAD) |
| I negative, aVF positive | Right axis deviation (RAD) |
Step 5 - P wave
- Present? Normal shape? Duration <0.12 sec? Positive in I and II?
- Absent = AF or junctional rhythm
Step 6 - PR interval
- Normal: 0.12-0.20 sec (3-5 small squares)
- Short (<0.12): WPW syndrome
- Prolonged (>0.20): 1st degree AV block
- Progressive lengthening then dropped beat: 2nd degree (Wenckebach)
- No relationship between P and QRS: 3rd degree (complete) heart block
Step 7 - QRS, ST, T waves
| Finding | Meaning |
|---|---|
| Wide QRS (>0.12 sec) | Bundle branch block or ventricular rhythm |
| LBBB pattern (broad notched R in V5/V6) | Left bundle branch block |
| RBBB pattern (RSR' in V1, broad S in V6) | Right bundle branch block |
| ST elevation | STEMI, pericarditis |
| ST depression | NSTEMI/unstable angina, ischemia, digoxin |
| T wave inversion | Ischemia, PE, LVH |
| Pathological Q wave | Old MI (>0.04 sec or >25% of R wave height) |
SECTION 5 - IMPORTANT CARDIAC INVESTIGATIONS AT A GLANCE
| Test | What it tells you | When to order |
|---|---|---|
| ECG | Rate, rhythm, ischemia, blocks | First test for all cardiac complaints |
| CXR | Cardiomegaly, pulmonary edema, effusion | Dyspnea, suspected heart failure |
| Echo (TTE) | EF, valve function, wall motion | Heart failure, murmur, suspected structural disease |
| BNP/NT-proBNP | Heart failure marker | Dyspnea - is it cardiac or respiratory? |
| Troponin I or T | Myocardial necrosis | Chest pain - rule in/rule out MI (serial: 0, 3, 6 hours) |
| Lipid profile | Cardiovascular risk | All cardiac patients |
| HbA1c | Diabetes control | All cardiac patients (diabetes = major risk factor) |
| TSH | Thyroid function | AF, heart failure |
SECTION 6 - CARDIAC DRUGS SUMMARY (You'll See These Daily)
| Drug | Class | Use | Key Side Effect |
|---|---|---|---|
| Aspirin | Antiplatelet | MI prevention, ACS | GI bleeding |
| Clopidogrel | Antiplatelet | After stent, ACS | Bleeding |
| Atorvastatin | Statin | Cholesterol, CAD prevention | Myopathy, ↑LFTs |
| Ramipril | ACE inhibitor | HTN, heart failure, post-MI | Dry cough, hyperkalemia |
| Metoprolol/Carvedilol | Beta-blocker | HTN, HF, angina, AF | Bradycardia, bronchospasm (avoid in asthma) |
| Amlodipine | Calcium channel blocker | HTN, angina | Ankle edema, flushing |
| Furosemide | Loop diuretic | Heart failure, edema | Hypokalemia, dehydration |
| Spironolactone | MRA | Heart failure, HTN | Hyperkalemia, gynecomastia |
| Digoxin | Cardiac glycoside | AF rate control, HF | Narrow therapeutic window - toxicity: nausea, xanthopsia (yellow vision), bradycardia |
| GTN (Nitroglycerin) | Nitrate | Angina relief | Headache, hypotension |
| Warfarin | Anticoagulant | AF, DVT, valve disease | Bleeding - monitor INR (target 2-3) |
| Heparin | Anticoagulant | ACS, DVT (acute) | Bleeding, HIT |
| Amiodarone | Antiarrhythmic | AF, VT | Thyroid, lung, liver, photosensitivity |
SECTION 7 - QUICK REFERENCE CARD (Memorize These)
NORMAL CARDIAC VALUES:
HR: 60-100 bpm
BP: <120/80 mmHg
Apex beat: 5th ICS, MCL
PR interval: 0.12-0.20 sec
QRS: <0.12 sec
EF (ejection fraction): 55-70% normal; <40% = HFrEF
KEY NUMBERS:
JVP normal: <4 cm above sternal angle (at 45°)
BNP: >100 pg/mL = likely heart failure
NT-proBNP: >125 pg/mL = heart failure
Troponin: ANY elevation = myocardial injury
TODAY'S SUMMARY (5 Lines)
- Cardiac exam follows: Hands → Pulse → BP → Face → JVP → Praecordium (IPPPA) → Lungs → Legs
- S3 = heart failure; S4 = stiff ventricle (HTN/LVH)
- STEMI = ST elevation on ECG → call senior immediately → aspirin + reperfusion
- AF = irregularly irregular pulse, no P waves, risk of stroke → anticoagulate
- Heart failure = dyspnea + edema + raised JVP + basal crackles → treat with BADS drugs
Come back tomorrow or whenever you see a new patient/condition in the cardiac ward. Tell me what you saw and I'll break it down for you!
Source: Fuster & Hurst's The Heart 15th Ed, Goldman-Cecil Medicine, Braunwald's Heart Disease
Tests in cardiac like ecg echo angio and other all how to learn and red it
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Excellent - rich content pulled from Harrison's, Washington Manual, Braunwald's, and the Textbook of Clinical Echocardiography. Here is your complete guide:
🔬 CARDIAC INVESTIGATIONS - How to Learn & Read All of Them
Complete Guide for Clinical Students
THE BIG PICTURE - What Test Gets Ordered When?
Patient comes with cardiac complaint
↓
STEP 1: ECG (first, always, within 10 minutes)
↓
STEP 2: Blood tests (Troponin, BNP, CBC, LFT, KFT, lipids)
↓
STEP 3: Chest X-Ray
↓
STEP 4: Echocardiogram (Echo/TTE) - structure & function
↓
STEP 5: Stress Test / Holter (if needed)
↓
STEP 6: CT Angio / MRI (specialized)
↓
STEP 7: Coronary Angiography (invasive - gold standard for arteries)
TEST 1 - ECG (Electrocardiogram)
What is an ECG?
A recording of the electrical activity of the heart using 10 electrodes placed on the body, producing 12 views (leads) of the heart.
The 12 Leads - What Each One "Looks At"
Limb leads (on arms and legs):
| Lead | Looks at |
|---|---|
| I | Lateral wall of heart |
| II | Inferior + conduction (used for rhythm strip) |
| III | Inferior wall |
| aVR | Right side (looks "into" the cavity - normally negative) |
| aVL | High lateral wall |
| aVF | Inferior wall |
Chest/Precordial leads (V1-V6):
| Lead | Looks at |
|---|---|
| V1-V2 | Septal wall |
| V3-V4 | Anterior wall |
| V5-V6 | Lateral wall |
Tip: V1 is at the RIGHT side of the sternum (4th ICS). V6 is at the axilla. They go in order across the chest.
The ECG Waveform - What Each Part Means
R
/ \
/ \
P T/ \
\ / \ S
\/ \ /
Q \_/
P wave → QRS complex → T wave
| Wave/Interval | What it represents | Normal Duration |
|---|---|---|
| P wave | Atrial depolarization (atria contract) | <0.12 sec (3 small squares) |
| PR interval | Time from atrial to ventricular activation (AV node delay) | 0.12-0.20 sec (3-5 small squares) |
| QRS complex | Ventricular depolarization (ventricles contract) | <0.12 sec (<3 small squares) |
| ST segment | Ventricles fully depolarized (should be at baseline) | Flat = normal |
| T wave | Ventricular repolarization (ventricles recover) | Same direction as QRS |
| QT interval | Total ventricular activity | <0.44 sec (corrected for rate) |
The ECG paper:
- Small square = 0.04 sec (40 ms) horizontally
- Large square = 0.20 sec (200 ms) = 5 small squares
- Vertically: 1 small square = 0.1 mV
How to READ an ECG - The 7-Step System (Never Skip Steps)
Step 1 - Check Calibration & Speed
- Standard speed: 25 mm/sec
- Standard calibration: 10 mm = 1 mV (look for calibration box at start)
Step 2 - Heart Rate
Regular rhythm:
Rate = 300 ÷ (number of large squares between two R peaks)
| Large squares between R-R | Heart rate |
|---|---|
| 1 | 300 bpm |
| 2 | 150 bpm |
| 3 | 100 bpm |
| 4 | 75 bpm |
| 5 | 60 bpm |
| 6 | 50 bpm |
Mnemonic: "300, 150, 100, 75, 60, 50"
Irregular rhythm: Count all QRS in a 10-second rhythm strip × 6
Step 3 - Rhythm
Ask yourself:
- Is it regular? (Are R-R intervals equal?)
- Is there a P wave before every QRS? (= sinus rhythm)
- Is the QRS narrow (<3 small squares) or wide?
| Pattern | Rhythm |
|---|---|
| Regular, P before every QRS, narrow QRS | Normal sinus rhythm ✓ |
| Regular, no P waves, narrow QRS | Junctional rhythm |
| Irregularly irregular, no P waves | Atrial Fibrillation |
| Regular saw-tooth waves, 2:1 or 4:1 QRS | Atrial Flutter |
| No organized activity, chaotic | Ventricular Fibrillation (emergency!) |
Step 4 - Axis
Look at leads I and aVF (the two "thumbs"):
| Lead I | aVF | Axis |
|---|---|---|
| Positive (upright) | Positive (upright) | Normal ✓ |
| Positive | Negative | Left axis deviation (LAD) |
| Negative | Positive | Right axis deviation (RAD) |
| Both negative | Extreme axis |
Causes:
- LAD: LBBB, left anterior fascicular block, inferior MI
- RAD: RBBB, right ventricular hypertrophy, lateral MI, PE
Step 5 - P Waves
- Present and upright in leads I and II = sinus rhythm
- Absent = AF, junctional rhythm, or complete heart block
- Peaked P in II (>2.5mm) = right atrial enlargement (P pulmonale)
- Broad notched P in II = left atrial enlargement (P mitrale)
Step 6 - PR Interval (0.12-0.20 sec)
| PR interval | Condition |
|---|---|
| Short (<0.12 sec) | WPW syndrome (delta wave), junctional |
| Normal (0.12-0.20) | Normal ✓ |
| Long >0.20 (1 big square) | 1st degree AV block |
| Progressive lengthening then dropped beat | 2nd degree Mobitz I (Wenckebach) |
| Fixed PR, some beats dropped | 2nd degree Mobitz II |
| P and QRS completely unrelated | 3rd degree (Complete) heart block - emergency! |
Step 7 - QRS, ST segment, T waves
QRS:
| Finding | Meaning |
|---|---|
| Wide QRS (>3 small squares / 0.12 sec) | BBB or ventricular origin |
| RBBB pattern (RSR' in V1, wide S in V6) | Right bundle branch block |
| LBBB pattern (broad M-shaped in V5/V6, W in V1) | Left bundle branch block |
| Pathological Q wave (>1 small square wide OR >25% of R height) | Old MI |
ST segment (the most important part for emergencies):
| ST change | Meaning |
|---|---|
| Elevation ≥1mm in ≥2 contiguous limb leads | STEMI (call senior now!) |
| Elevation ≥2mm in ≥2 contiguous chest leads | STEMI |
| Saddle-shaped elevation in all leads | Pericarditis |
| Depression ≥1mm | Ischemia, NSTEMI, digoxin effect |
| Horizontal/downsloping depression | More specific for ischemia |
T waves:
- Inverted T in V1-V4 = anterior ischemia, PE, right heart strain
- Tall peaked T = hyperkalemia (early), hyperacute STEMI
- Flattened T = hypokalemia, ischemia
ECG Patterns to Recognize Immediately
STEMI (Emergency - shout for help):
- ST elevation in at least 2 leads in the same territory
- New LBBB can also = STEMI equivalent
AF (Atrial Fibrillation):
- No P waves
- Irregularly irregular QRS
- Wavy/fibrillatory baseline
Complete Heart Block (3rd degree):
- P waves march at their own rate (~30-60 bpm)
- QRS complex marches at its own slower rate
- They have NO relationship to each other
- Wide QRS (escape rhythm from ventricles)
Ventricular Tachycardia (VT):
- Wide QRS tachycardia (rate >100, QRS >0.12)
- Monomorphic (all QRS same shape) = regular VT
- If pulseless = VF → Defibrillate immediately
WPW (Wolff-Parkinson-White):
- Short PR (<0.12 sec)
- Delta wave (slurred upstroke of QRS)
- Wide QRS
- Accessory pathway bypasses AV node
TEST 2 - ECHOCARDIOGRAM (Echo / TTE)
What is it?
Ultrasound of the heart. Completely non-invasive. Uses sound waves to create real-time images of the heart's structure and function.
Types of Echo
| Type | How | What it shows |
|---|---|---|
| TTE (Transthoracic Echo) | Probe on chest wall | Standard views - structure, EF, valves |
| TOE/TEE (Transoesophageal) | Probe swallowed - sits behind heart | Better images - used for valves, thrombus, endocarditis |
| Stress Echo | Echo during exercise or dobutamine | Wall motion abnormalities during ischemia |
| 3D Echo | Volumetric imaging | Detailed valve anatomy, EF |
The Most Important Echo Numbers to Know
| Measurement | Normal Value | Abnormal means |
|---|---|---|
| Ejection Fraction (EF) | 55-70% | <40% = HFrEF (systolic failure) |
| LV end-diastolic diameter | <5.5 cm | >5.5 = dilated LV |
| LV wall thickness | 0.6-1.1 cm | >1.1 = LVH (hypertrophy) |
| Aortic root | <3.7 cm | >4.0 = aortic root dilation (Marfan risk) |
| IVC diameter | <2.1 cm, collapses >50% | Non-collapsing IVC = raised RA pressure |
What the Echo Report Will Tell You
When you see an echo report on the ward, look for these 5 things:
1. LV size and function:
- EF% - the most important single number
- Wall motion abnormality (WMA) = area of heart not moving = previous MI
2. RV function:
- TAPSE >17mm = normal RV function
- <17mm = RV dysfunction (cor pulmonale, PE, right heart failure)
3. Valves:
- Each valve graded as: Normal / Mild / Moderate / Severe regurgitation or stenosis
- Aortic valve area (AVA): Normal >2 cm², Severe AS <1 cm²
4. Pericardium:
- Pericardial effusion = fluid around heart
- Large effusion + hemodynamic compromise = cardiac tamponade (emergency)
5. Doppler findings:
- E/A ratio for diastolic function
- Pressure gradients across valves (e.g., mean gradient >40 mmHg = severe AS)
How to understand Echo views (what the probe shows):
| View | How to get it | What you see |
|---|---|---|
| Parasternal long axis (PLAX) | Probe left of sternum, 3-4th ICS | LV, aortic valve, mitral valve side-on |
| Parasternal short axis (PSAX) | Same position rotated 90° | Cross-section of LV - like looking down a barrel |
| Apical 4-chamber | Probe at apex (where you felt apex beat) | All 4 chambers at once - great for EF |
| Subcostal | Probe below xiphisternum | IVC, pericardial effusion |
As a student: watch the echo tech/doctor do it, ask them what view they're taking and what they're looking for.
TEST 3 - CORONARY ANGIOGRAPHY (Cardiac Cath / Angio)
What is it?
An invasive procedure where a thin catheter is inserted through the radial artery (wrist) or femoral artery (groin), advanced to the heart, and contrast dye is injected into the coronary arteries under X-ray. This shows blockages directly.
(Source: Harrison's Principles of Internal Medicine 22nd Ed, Ch. 249)
When is it done? (Indications)
| Situation | Why angio |
|---|---|
| STEMI | Immediate PCI (open the blocked artery) |
| ACS (NSTEMI/unstable angina) | Risk stratification + possible stenting |
| Stable angina not controlled by drugs | Check severity of blockages |
| Positive stress test | Confirm ischemia, plan treatment |
| Before valve surgery | Rule out coexisting coronary disease |
| New-onset heart failure | Check if ischemic cause |
| Cardiogenic shock | Urgent revascularization |
What you see on angiogram:
- Normal artery: Smooth, well-defined lumen with good dye flow
- Stenosis: Narrowing of the artery - described as % blockage (e.g., 70% stenosis)
- Occlusion: Complete block, no dye flow beyond the point
- TIMI flow grade:
- Grade 0 = no flow (complete occlusion)
- Grade 1 = trickle
- Grade 2 = partial flow
- Grade 3 = normal flow ✓
What happens after angio?
| Finding | Action |
|---|---|
| <50% stenosis | Medical management only |
| 50-70% stenosis | Depends on symptoms and FFR measurement |
| >70% stenosis | PCI (stenting) or CABG (bypass surgery) |
| Left main disease or triple vessel disease | CABG preferred |
PCI (Angioplasty + Stent):
- Balloon inflated to open stenosis
- Stent (metal mesh tube) placed to keep artery open
- Drug-eluting stent (DES) = coated with drug to prevent re-narrowing
- Post-stent: dual antiplatelet for at least 12 months (Aspirin + Clopidogrel)
TEST 4 - BLOOD TESTS IN CARDIAC PATIENTS
Cardiac Enzymes / Biomarkers
Troponin (the most important)
- Released when heart muscle cells die
- Types: Troponin I (TnI) and Troponin T (TnT) - high sensitivity versions used now
- Any elevation = myocardial injury (must interpret with clinical context)
| Time from MI | Troponin level |
|---|---|
| 0-2 hours | Starting to rise |
| 3-6 hours | Detectably elevated |
| 12-24 hours | Peak |
| 7-10 days | Returns to normal |
Serial troponins: Always order at 0h, 3h, 6h - a RISE is more meaningful than a single value
Causes of elevated troponin other than MI:
- PE (pulmonary embolism)
- Myocarditis
- Sepsis
- Renal failure
- Tachyarrhythmia
- Stroke/subarachnoid hemorrhage
BNP / NT-proBNP (Heart Failure Marker)
- Released by ventricles when they are stretched (volume/pressure overload)
- Best test for: "Is this dyspnea cardiac or respiratory?"
| BNP Level | Interpretation |
|---|---|
| <100 pg/mL | Heart failure unlikely |
| 100-400 | Indeterminate - assess clinically |
| >400 pg/mL | Heart failure very likely |
| NT-proBNP | Interpretation |
|---|---|
| <125 pg/mL (age <75) | Heart failure unlikely |
| >900 pg/mL (age <75) | Heart failure likely |
Raised BNP also in: Renal failure, PE, severe infection, AF, RV overload
CK-MB (Creatine Kinase - MB fraction)
- Older marker, less specific than troponin
- Still used in some centers to detect re-infarction (rises faster than troponin after repeat MI)
Other Blood Tests Ordered in Cardiac Patients
| Test | Why ordered | What to look for |
|---|---|---|
| CBC | Anemia worsens cardiac disease | Low Hb = anemia |
| Lipid profile | Cardiovascular risk | LDL >100 mg/dL = treat if CAD |
| HbA1c | Diabetes control | >6.5% = diabetic |
| KFT (creatinine) | Renal function before ACEi, contrast dye | Check before angio |
| Potassium | Before diuretics, ACEi | <3.5 = hypokalemia (arrhythmia risk) |
| TSH | Thyroid disease causes AF, HF | High TSH = hypothyroidism, low = hyperthyroidism |
| Serum ferritin + iron | Iron deficiency worsens heart failure | Low ferritin = give IV iron |
| Coagulation (PT/INR) | Warfarin monitoring | Target INR 2-3 for AF |
| D-dimer | Suspected PE or DVT | <500 = PE unlikely if low pre-test probability |
TEST 5 - CHEST X-RAY (CXR) IN CARDIAC DISEASE
How to Read a CXR Systematically (ABCDE)
Always check in this order:
Before reading: Is it PA (posterior-anterior) or AP? AP films (portable) make the heart look bigger - don't diagnose cardiomegaly on AP.
A - Airway
- Trachea midline? (pushed = tension pneumothorax, mediastinal mass)
B - Bones & Borders
- Look at ribs, clavicles for rib notching (coarctation of aorta)
- Heart borders sharp? (blurred = consolidation next to heart)
C - Cardiac size
- CTR (Cardiothoracic Ratio): Widest heart diameter ÷ widest chest diameter
- Normal < 0.5 (heart occupies less than half the chest)
-
0.5 on PA film = cardiomegaly
D - Diaphragm
- Right higher than left (liver below)
- Loss of costophrenic angle = pleural effusion
- Air under diaphragm = perforated viscus (surgery emergency)
E - Everything Else (pulmonary vasculature)
Look for signs of heart failure:
| X-ray Sign | Meaning |
|---|---|
| Upper lobe venous diversion | Early left heart failure (veins in upper zones become more prominent) |
| Kerley B lines (horizontal lines at bases) | Interstitial edema |
| Bat-wing / Butterfly shadowing | Alveolar pulmonary edema - severe |
| Bilateral pleural effusions | Heart failure, hypoalbuminemia |
| Large globular heart shadow | Pericardial effusion ("flask-shaped heart") |
TEST 6 - STRESS TEST (Exercise ECG / TMT)
What is it?
Patient walks on a treadmill while an ECG is continuously recorded. Speed and incline increase every 3 minutes (Bruce protocol). Heart rate and blood pressure monitored throughout.
Why done?
- Diagnose angina / ischemia
- Risk-stratify after MI
- Assess exercise-induced arrhythmias
Positive stress test (= ischemia) - stop the test if any of these:
- ST depression >1mm (horizontal or downsloping) during exercise
- ST elevation during exercise
- Chest pain reproduced
- BP drops during exercise (hypotension = severe disease)
- Serious arrhythmia (VT, VF)
Contraindications (don't do stress test in these patients):
- STEMI within 2 days
- Unstable angina (ongoing chest pain)
- Uncontrolled heart failure
- Severe aortic stenosis
- Uncontrolled arrhythmia
When stress test is positive → proceed to coronary angiography
TEST 7 - HOLTER MONITOR & AMBULATORY ECG
What is it?
A small device the patient wears for 24-48 hours (or up to 2 weeks with event recorder) that continuously records the ECG while the patient goes about their daily life.
(Source: Washington Manual of Medical Therapeutics)
Why used?
- Patient reports palpitations, dizziness, blackouts - but ECG in clinic is normal
- Monitor for paroxysmal AF (comes and goes)
- Assess heart rate response to antiarrhythmic drugs
Types:
| Device | Duration | Used for |
|---|---|---|
| Holter monitor | 24-48 hours | Frequent palpitations |
| Event recorder (loop) | Weeks to months | Infrequent symptoms |
| Implantable loop recorder (ILR) | Up to 3 years | Very rare syncope, cryptogenic stroke |
| Telemetry (inpatient) | Continuous | Hospitalized cardiac patients |
What to look for in a Holter report:
- Maximum and minimum heart rate over 24 hours
- Any pauses (>3 seconds = significant)
- PACs (premature atrial contractions) or PVCs (ventricular)
- Paroxysmal AF episodes
- Does the patient's diary symptoms match any arrhythmia on the recording?
TEST 8 - CT CORONARY ANGIOGRAPHY (CTCA) & CARDIAC MRI
CTCA (CT Coronary Angiogram)
- Non-invasive way to look at coronary arteries using a CT scanner + contrast dye
- Used for: Intermediate-risk chest pain, ruling out significant CAD
- Gives calcium score (higher = more plaque = higher CV risk)
- Cannot treat (unlike invasive angiography) - only diagnoses
Cardiac MRI (CMR)
- Best test for: Myocarditis, cardiomyopathy, cardiac masses, pericardial disease, viability assessment
- No radiation
- Late gadolinium enhancement (LGE): Shows areas of scar tissue (fibrosis) - crucial for cardiomyopathy diagnosis
- Not available everywhere - done in specialized centers
SUMMARY TABLE - Which Test Answers Which Question?
| Clinical Question | Best Test |
|---|---|
| Is there an arrhythmia right now? | ECG |
| Did this patient have an MI? | Serial Troponin (0, 3, 6h) |
| Does the patient have heart failure? | BNP + Echo |
| How strong is the heart pumping? | Echo (EF%) |
| Are the heart valves working? | Echo (Doppler) |
| Is there significant coronary blockage? | Coronary Angiography (gold standard) |
| Screening for CAD non-invasively? | CTCA |
| Intermittent palpitations at home? | Holter monitor |
| Is there cardiac scar/myocarditis? | Cardiac MRI |
| Is there pulmonary edema? | Chest X-Ray |
| Exercise-induced chest pain? | Stress test (TMT) |
| Before giving contrast/ACEi? | Serum creatinine |
| Before giving diuretics? | Serum potassium |
DAILY CARD - Stick This on Your Notebook
ECG READING ORDER (Never skip):
1. Rate 2. Rhythm 3. Axis 4. P waves
5. PR interval 6. QRS 7. ST & T waves
NORMAL VALUES:
HR: 60-100 | PR: 3-5 small squares
QRS: <3 squares | QT: <11 squares
ST: flat/isoelectric | T: same direction as QRS
STEMI = ST elevation in 2+ contiguous leads → EMERGENCY
AF = No P waves + irregular QRS
3rd degree block = P and QRS unrelated → EMERGENCY
ECHO: EF <40% = systolic failure (HFrEF)
TROPONIN: Any rise = myocardial injury
BNP >400 = heart failure likely
Practice method: Every day in the ward, ask your resident/intern - "Can I look at today's ECG with you?" Do it for 10 patients and you will recognize patterns faster than any book can teach you. Ask: "What are you looking for? What does this mean for this patient?"
Sources: Harrison's Principles of Internal Medicine 22nd Ed (2025), Washington Manual of Medical Therapeutics, Braunwald's Heart Disease, Textbook of Clinical Echocardiography
In patient ward possible of any departments what need to learn all explain fast
Finding Sources
Finding Sources
Searching the Web
medical student inpatient ward skills checklist all departments general medicine surgery OBG pediatrics
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Good - I have enough content. Here is the complete, fast, all-department inpatient ward guide:
🏥 INPATIENT WARD - Everything You Need to Know
All Departments | Fast & Practical
THE GOLDEN RULE IN ANY WARD
Every patient in every department needs the same 3 things from you:
- A proper history
- A proper examination
- A plan (investigations + treatment)
The rest is just department-specific details layered on top.
PART 1 - WHAT HAPPENS IN THE WARD (Daily Routine)
Understanding the ward routine is the first thing to learn. Everything runs on a schedule.
The Typical Ward Day
| Time | Activity | What you do |
|---|---|---|
| 7:00-8:00 AM | Pre-round | Check vitals chart, review overnight events, read new results |
| 8:00-10:00 AM | Ward rounds | Walk with team, present your patients, take notes |
| 10:00 AM-1:00 PM | Post-round work | Collect samples, write notes, assist procedures |
| 2:00-4:00 PM | Afternoon rounds/procedures | Follow up results, IV fluids, dressings |
| 4:00-5:00 PM | Handover | Pass information to night team |
The Hierarchy - Know Who is Who
Consultant (Attending) → Head of team
↓
Senior Resident (PG 2-3) → Runs the ward
↓
Junior Resident (PG 1) → Day-to-day orders
↓
Intern → Direct ward work
↓
YOU (Student) → Learn, observe, assist
Your rule: Never do anything to a patient without a senior knowing. Always ask. Never assume.
PART 2 - UNIVERSAL WARD SKILLS (Every Department)
These apply in medicine, surgery, OBG, pediatrics, orthopedics, ENT - everywhere.
SKILL 1 - Reading the Bedside Chart
Every inpatient bed has a chart hanging at the end. Learn to read it.
TEMPERATURE CHART (TPR chart):
- Temperature: plotted as dots - look for fever spikes (>38°C) or hypothermia (<36°C)
- Pulse: plotted as line
- Respiration rate: noted
- Blood pressure: recorded each shift
- SpO2: oxygen saturation
- Input/Output chart: IV fluids in + oral in / urine out + drain out
What to check every morning before rounds:
- Max temp in last 24 hours - fever? improving?
- Pulse rate trend
- Blood pressure - high/low?
- Urine output - minimum acceptable = 0.5 mL/kg/hour (e.g., 70kg person = 35 mL/hour minimum)
- Any overnight events written in nursing notes?
SKILL 2 - IV Lines & IV Fluids
You will see IV lines in almost every patient. Know the basics.
Types of IV Access:
| Type | Where | Used for |
|---|---|---|
| Peripheral IV (cannula) | Vein on hand/forearm | Fluids, drugs (most patients) |
| Central line (CVP) | Neck/chest/groin | ICU patients, caustic drugs, CVP monitoring |
| Arterial line | Radial artery | Continuous BP monitoring, ABG |
IV Fluid Types - Know These 5:
| Fluid | Contents | When used | Watch out for |
|---|---|---|---|
| Normal Saline (NS) 0.9% | NaCl 154 mEq/L | Hypovolemia, hyponatremia | Hyperchloremic acidosis if large volumes |
| Dextrose 5% (D5W) | 50g glucose/L | Hypoglycemia, maintenance, drug diluent | NOT for hyponatremia |
| Ringer's Lactate (RL) | Na, K, Ca, lactate | Surgical patients, trauma, burns | Most physiological |
| DNS (Dextrose Normal Saline) | D5 + half NS | Maintenance fluids, pediatrics | Common in wards |
| Dextrose 10% (D10W) | 100g glucose/L | Severe hypoglycemia, neonates | Hyperglycemia |
How to read an IV order:
"1 pint NS over 6 hours" = 500 mL normal saline → drip rate = 500/6 = ~83 mL/hour
Drop rate formula (macro-drip set, 20 drops/mL):
Drops/min = (Volume in mL × 20) ÷ (Time in minutes)
Signs that IV site needs to be changed:
- Redness, swelling, pain at cannula site = phlebitis → change site immediately
- Fluid not draining = blocked → flush gently or re-site
- Cannula sites should be changed every 72 hours routinely
SKILL 3 - Oxygen Therapy
You will see oxygen being given to patients in every department.
Oxygen Delivery Devices:
| Device | Flow Rate | FiO2 delivered | Used when |
|---|---|---|---|
| Nasal cannula (prongs) | 1-6 L/min | 24-44% | Mild hypoxia, comfortable for patient |
| Simple face mask | 5-10 L/min | 35-55% | Moderate hypoxia |
| Non-rebreather mask (NRM) | 10-15 L/min | 60-90% | Severe hypoxia, emergency |
| Venturi mask | Fixed rates | Precise % (24%, 28%, 35%, 40%, 60%) | COPD patients (controlled O2) |
Target SpO2:
- Most patients: 94-98%
- COPD patients: 88-92% (too much O2 can suppress their drive to breathe)
Key rule: If SpO2 <90% or patient is distressed - increase O2, call senior, prepare for escalation.
SKILL 4 - Reading Drug Charts & Prescriptions
Every patient has a drug chart (prescription sheet). You must be able to read it.
Parts of a Drug Chart:
Regular medications: given every day at set times
PRN (as needed): given only when patient asks or when certain condition met
One-time (STAT) dose: given immediately once
IV medications: separate section, with rate
Common Abbreviations on Drug Charts:
| Abbreviation | Meaning |
|---|---|
| OD / QD | Once daily |
| BD / BID | Twice daily |
| TDS / TID | Three times daily |
| QID | Four times daily |
| HS / ON | At night (hora somni) |
| AC | Before meals |
| PC | After meals |
| PRN / SOS | As needed |
| STAT | Immediately |
| SC | Subcutaneous |
| IM | Intramuscular |
| IV | Intravenous |
| PO | By mouth (oral) |
| SL | Sublingual (under tongue) |
| NGT | Through nasogastric tube |
SKILL 5 - Writing a Progress Note (SOAP Format)
Every day, for every patient, a progress note is written. The standard format is SOAP:
Date: 24/06/2026 Time: 08:30 Day 3 of admission
S - Subjective (what the patient says):
"Patient reports reduced chest pain today. Still some breathlessness on exertion.
Slept well. Appetite improving."
O - Objective (what you find):
Vitals: T 37.2°C, P 88 bpm regular, BP 128/82, RR 18, SpO2 97% on room air
General: Alert, comfortable at rest
CVS: S1 S2 heard, no murmurs. JVP not raised.
RS: Clear air entry bilaterally, no crackles.
Abdomen: Soft, non-tender
Investigations: Today's Troponin 0.04 (down from 1.2 on admission). ECG: sinus rhythm, no new changes.
A - Assessment (your impression):
NSTEMI - clinically improving. Troponin trending down. Haemodynamically stable.
P - Plan:
Continue aspirin 75mg + clopidogrel 75mg + atorvastatin 40mg + ramipril 2.5mg
Urology review not needed
Echo ordered - pending
Plan for stress test before discharge
Discussed with Dr. [Senior name]
Minimum you need to write every day: Vitals + overnight events + current status + plan changes
SKILL 6 - Recognizing a Sick Patient (ABCDE Emergency Approach)
In any department, if a patient suddenly deteriorates, use ABCDE:
| Step | Check | Action if abnormal |
|---|---|---|
| A - Airway | Can they speak? Gurgling/stridor? | Head tilt, jaw thrust, suction, call senior |
| B - Breathing | RR, SpO2, chest movement | High-flow O2, examine chest |
| C - Circulation | Pulse, BP, cap refill, cold limbs | IV access, fluid bolus, ECG |
| D - Disability | GCS, pupils, blood glucose | Check BGL (hypoglycemia is common!) |
| E - Exposure | Fever, rash, bleeding, drain output | Full exposure, check drug chart |
Call for help IMMEDIATELY if:
- SpO2 <90% despite O2
- BP <90/60 or falling
- HR <40 or >150
- GCS drop of >2 points
- Unresponsive patient
- New seizure
PART 3 - DEPARTMENT-SPECIFIC WARD KNOWLEDGE
🏥 GENERAL MEDICINE WARD
What you see here:
Diabetes, hypertension, heart failure, stroke, infections (pneumonia, UTI, cellulitis), COPD exacerbations, renal failure, liver disease, anemia.
Most Common Admissions & What to Know:
1. Diabetic Patient in Ward
Monitoring: Blood glucose levels (BGL) - 4 times a day (fasting, pre-lunch, pre-dinner, bedtime)
Common problems to watch for:
| Problem | BGL | Symptoms | Treatment |
|---|---|---|---|
| Hypoglycemia | <70 mg/dL | Sweating, trembling, confusion, palpitations | 15g sugar (juice/glucose) + recheck in 15 min |
| Hyperglycemia | >250 mg/dL | Polyuria, thirst, weakness | Insulin sliding scale or correction dose |
| DKA | Usually >300, with ketones | Fruity breath, deep breathing (Kussmaul), vomiting | IV fluids + insulin infusion (emergency!) |
| HHS | >600, NO ketones | Extreme dehydration, confusion, elderly | IV fluids slowly |
Insulin types you'll see on drug charts:
| Insulin | Onset | Duration | Given when |
|---|---|---|---|
| Regular/Actrapid (short-acting) | 30 min | 6-8 hours | Before meals or sliding scale |
| NPH (intermediate) | 1-2 hr | 12-18 hours | BD dosing |
| Glargine/Lantus (long-acting) | 1-2 hr | 24 hours | Once daily, basal |
2. Hypertensive Patient
- Target BP in ward: <140/90 (general), <130/80 (diabetic/CKD)
- Hypertensive emergency: BP >180/120 + end organ damage (headache, visual changes, confusion, chest pain) → IV labetalol or nitroprusside - call senior immediately
- Hypertensive urgency: BP >180/120, NO end organ damage → oral antihypertensives, reduce slowly over 24-48 hours
3. Fever in a Ward Patient
Common causes: Pneumonia, UTI, cellulitis, line infection (IV site), DVT, drug fever, abscess
Fever workup:
- Blood culture (2 sets from different sites, before antibiotics)
- Urine culture and sensitivity (C&S) + urine routine
- CXR
- CBC with differential (neutrophils up = bacterial, lymphocytes up = viral)
- Examine: IV sites, wound sites, chest, abdomen, legs (for DVT)
Temperature fever grades:
- Low grade: 37.5-38°C
- Moderate: 38-39°C
- High grade: >39°C
- Hyperpyrexia: >41°C (emergency - brain damage risk)
4. Stroke Patient in Medicine Ward
FAST: Face drooping, Arm weakness, Speech difficulty, Time to call emergency
Types:
| Ischemic Stroke | Hemorrhagic Stroke | |
|---|---|---|
| Cause | Clot blocking artery | Blood vessel bursting |
| CT scan | Normal initially / later infarct | Bright white (blood) immediately |
| Treatment | tPA (thrombolysis) within 4.5 hours OR thrombectomy | BP control, neurosurgery review |
| Anticoagulation | YES (prevent recurrence) | NO (makes bleeding worse) |
What to monitor on ward:
- Neuro obs every 4-8 hours: GCS, pupils, limb power
- BP (target varies - don't over-lower in first 24 hours)
- Blood glucose (hyperglycemia worsens stroke)
- Swallow assessment before giving oral food/drugs (aspiration risk)
- DVT prophylaxis (compression stockings, heparin)
🔪 SURGERY WARD
What you see here:
Pre-op and post-op patients, wounds, drains, appendicitis, cholecystitis, hernias, bowel obstruction, trauma.
Pre-Operative Patient (Before Surgery):
Pre-op checklist - know this cold:
- Patient fasted? (6 hours for food, 2 hours for clear fluids)
- Consent signed?
- Blood group and cross-match done?
- Investigations: CBC, KFT, LFT, coagulation, ECG, CXR
- Allergies documented?
- Regular medications reviewed (hold metformin, warfarin, aspirin as instructed)
- IV access secured?
- Anaesthesia review done?
- Mark the site of surgery?
Post-Operative Patient (After Surgery):
The 5 Ws of post-op fever (most common reason juniors called at night):
| Time post-op | Cause | W |
|---|---|---|
| Day 1-2 | Wind - atelectasis (collapsed alveoli), pneumonia | Pulmonary |
| Day 3-5 | Water - UTI | Urinary |
| Day 5-7 | Wound infection | Wound |
| Day 5+ | Walking - DVT/PE | Venous |
| Anytime | Wonder drugs - drug fever | Drug/IV line |
Post-op monitoring - check these every round:
- Vitals trend
- Pain score (0-10) - is analgesia adequate?
- Wound: dry and intact? Any ooze, redness, dehiscence?
- Drains: type, color, amount of output
- Urine output (catheter bag)
- Bowel sounds returned? Passing gas? (before allowing oral feeds)
- IV site clean?
- DVT prophylaxis ordered?
Surgical Drains - What You'll See:
| Drain type | Looks like | Used for | What to check |
|---|---|---|---|
| Corrugated (passive) | Flat rubber sheet | Wound dead space | Amount, color of fluid |
| Redivac/suction | Plastic bulb with vacuum | Enclosed spaces (breast, neck) | Collapse of bulb = working |
| Intercostal drain (ICD) | Tube in chest → water seal | Pneumothorax, hemothorax, effusion | Bubbling, swinging, amount |
| T-tube | T-shaped in bile duct | After cholecystectomy | Bile output |
| Ryle's tube (NG tube) | Tube through nose to stomach | Decompression, aspiration | Aspirate color, amount |
Drain output colors:
- Serous (clear/straw yellow) = normal wound fluid
- Serosanguinous (pink) = normal after surgery
- Sanguinous (frank blood) = active bleeding - call senior
- Purulent (cloudy/thick) = infection
- Bilious (green) = bile leak
- Chylous (milky white) = lymphatic leak
Wound Dressings - How to Assist:
Basic sequence:
- Wash hands, gloves on (sterile for clean wounds)
- Remove old dressing - note: wet? soiled? adherent?
- Clean wound with saline or antiseptic (per surgeon's instruction)
- Inspect wound: is it healing? Any dehiscence (opening), infection, necrosis?
- Apply new dressing
- Document wound appearance in notes
Wound healing classification:
- Primary intention: edges closed (sutured) - clean surgical wounds
- Secondary intention: left open to heal from base - infected/large wounds
- Tertiary (delayed primary): cleaned first, then closed later
👶 PEDIATRICS WARD
The key difference: everything depends on AGE and WEIGHT
Calculating Drug Doses in Children:
Most drugs are given per kg body weight
Weight estimation if scale not available:
- Age 1-10 years: Weight (kg) = (Age + 4) × 2
- e.g., 6-year-old: (6+4) × 2 = 20 kg
Common Pediatric Ward Problems:
Fever in a Child
Febrile seizure: Most common cause of seizure in children (6 months - 5 years)
- Simple: <15 min, one episode, no focal features → benign, good prognosis
- Complex: >15 min, focal, repeated → investigate for meningitis
- Immediate management: ABC, position (lateral), diazepam if >5 min (0.5 mg/kg PR or IV 0.2-0.3 mg/kg)
Fever in neonate (<28 days): ALWAYS serious - sepsis must be excluded. Full septic screen + antibiotics.
Dehydration in Children
Assessment:
| Degree | % body weight lost | Signs |
|---|---|---|
| Mild | <5% | Slightly dry mouth, normal eyes, normal skin turgor |
| Moderate | 5-10% | Sunken eyes, reduced skin turgor, tachycardia |
| Severe | >10% | Sunken fontanelle, very dry, no tears, weak/absent pulse |
Oral Rehydration Salts (ORS): First line for mild-moderate dehydration
IV Fluids: For severe dehydration or unable to take orally
Rehydration calculation:
- Deficit = % dehydration × weight × 10 mL/kg
- Plus maintenance fluids per day (Holliday-Segar rule):
- 0-10 kg: 100 mL/kg/day
- 10-20 kg: 1000 mL + 50 mL/kg for each kg above 10
-
20 kg: 1500 mL + 20 mL/kg for each kg above 20
Jaundice in Newborn (Neonatal Jaundice)
- Physiological: Appears day 2-3, gone by day 14 in term, day 21 in preterm - normal
- Pathological: Appears <24 hours OR persists >14 days OR bilirubin very high → treat
- Treatment: Phototherapy (blue light breaks down bilirubin through skin)
- Severe: Exchange transfusion (double-volume blood exchange)
Common Pediatric Presentations Table:
| Condition | Age | Key signs | First thing to do |
|---|---|---|---|
| Bronchiolitis | <2 years | Wheeze, tachypnea, feeding difficulty | O2, hydration, supportive care |
| Croup | 6 months-3 years | Barking cough, stridor (inspiratory) | Dexamethasone 0.6 mg/kg oral/IM |
| Epiglottitis | 2-7 years | Drooling, tripod position, high fever, muffled voice | DON'T examine throat - secure airway first |
| Intussusception | 3 months-6 years | Colicky pain, current jelly stool, sausage-shaped mass | USS abdomen - air enema reduction |
| Meningitis | Any | Neck stiffness, photophobia, petechial rash, bulging fontanelle | LP + antibiotics ASAP |
🤰 OBG WARD (Obstetrics & Gynecology)
Obstetrics Section:
Key monitoring in ANC ward:
| Measurement | How often | Normal | Alarm |
|---|---|---|---|
| BP | Every visit | <140/90 | >140/90 after 20 weeks = preeclampsia |
| Urine dipstick | Every visit | No protein, no glucose | Proteinuria = preeclampsia risk |
| Fundal height | Every visit | = weeks of pregnancy (cm) | Too small = IUGR, too big = twins/polyhydramnios |
| Fetal heart rate (FHR) | Every visit | 110-160 bpm | <110 or >160 = fetal distress |
| Edema | Every visit | Mild ankle ok | Facial/generalized = preeclampsia |
G_P_ notation explained:
- G = Gravida (total pregnancies including current)
- P = Para (deliveries >28 weeks)
- A/L = Abortions/Live births
- Example: G3P2A1 = 3 pregnancies, 2 deliveries, 1 abortion
Trimesters:
- 1st: 0-13 weeks (organogenesis - MOST drug-sensitive)
- 2nd: 14-26 weeks (growth phase)
- 3rd: 27-40 weeks (preparation for birth)
SAFE drugs in pregnancy: Paracetamol, penicillins, cephalosporins, methyldopa, labetalol, heparin
DANGEROUS in pregnancy (avoid): NSAIDs (3rd trimester), tetracyclines, warfarin, ACE inhibitors, methotrexate, statins
Obstetric emergencies (shout for help + call senior):
| Emergency | Signs | Immediate action |
|---|---|---|
| Eclampsia | Seizure in pregnant/postpartum woman | MgSO4 4g IV loading dose, airway, O2 |
| PPH | >500mL blood loss after vaginal delivery | Fundal massage, oxytocin 10 IU IM, IV access |
| Cord prolapse | Cord visible/felt at cervix | Head down position, push presenting part up, emergency C-section |
| Placenta previa | Painless bright red bleeding | No vaginal exam! IV access, crossmatch, emergency C-section |
| Placental abruption | Painful dark bleeding, rigid uterus | IV access, fetal monitoring, possible C-section |
Gynecology Section:
Common admissions:
- Ectopic pregnancy (always check pregnancy test in female of reproductive age with pelvic pain)
- PID (pelvic inflammatory disease)
- Ovarian cyst - torsion or rupture
- Uterine fibroid with bleeding
- Post-operative hysterectomy/myomectomy
🦴 ORTHOPEDICS WARD
Common admissions: Fractures (hip, wrist, spine), joint replacements, infections (osteomyelitis, septic arthritis), post-op spinal surgery
Key things to check post-ortho surgery:
Neurovascular check (every 4 hours for first 24 hours):
- 5 P's: Pain (out of proportion = compartment syndrome!) | Pallor | Paresthesia | Paralysis | Pulselessness
- Any of these = emergency - compartment syndrome or vascular injury
Compartment syndrome: Pressure builds up inside fascial compartment → muscle death → emergency fasciotomy
- Classic: Pain out of proportion to injury, pain on passive stretch, tense swollen limb
Traction care:
- Check weights are hanging freely
- Limb in correct position
- Skin under traction device - pressure sores?
DVT prophylaxis is critical in ortho:
- All hip/knee replacement patients → low molecular weight heparin (enoxaparin) + compression stockings
- Early mobilization encouraged
👁️ ENT WARD
Common admissions: Tonsillectomy, adenoidectomy, septoplasty, tracheostomy, head & neck cancers, epistaxis (nosebleed)
Post-tonsillectomy watch for:
- Bleeding (primary = within 24 hours, secondary = days 5-10) → emergency return to OR
- Pain score, able to swallow
- No hot drinks/spicy food for 2 weeks
Tracheostomy care:
- Tie/flange secure (2-finger gap)
- Inner tube cleaned every 4-8 hours
- Suction PRN
- Always have same-size spare tube at bedside
- Emergency: tube blocked → remove inner tube → if still blocked → deflate cuff → if still blocked → remove tube → ventilate via stoma
Epistaxis (nosebleed) management:
- Sit forward, breathe through mouth
- Pinch soft part of nose for 10 minutes continuous
- If not stopped: anterior nasal packing (Merocel/BIPP)
- Posterior bleed: posterior packing, ENT review
🧠 NEUROLOGY / NEUROSURGERY WARD
Common admissions: Stroke, seizures, meningitis, Guillain-Barré, raised ICP, post-craniotomy
Neuro Obs (Neurological Observations):
Done every 1-4 hours depending on severity:
- GCS (E+V+M, max 15)
- Pupils: Size (mm), equality, reaction to light (PEARL = Pupils Equal And Reactive to Light)
- Limb power: Grade 0-5 each limb
- Temperature, BP, pulse
Raised ICP (Intracranial Pressure) signs - Cushing's Triad:
- Hypertension (high BP)
- Bradycardia (slow heart rate)
- Irregular breathing (Cheyne-Stokes) → This is a pre-terminal sign - call senior immediately
Lumbar Puncture (LP) - what you need to know as a student:
- Patient in lateral decubitus (fetal position) or seated leaning forward
- Level: L3-L4 or L4-L5 (below spinal cord ending at L1-L2)
- Normal CSF: Clear, opening pressure 6-20 cmH2O
| CSF finding | Bacterial meningitis | Viral meningitis | TB meningitis |
|---|---|---|---|
| Appearance | Turbid/cloudy | Clear | Slightly turbid |
| Cells | PMNs (thousands) | Lymphocytes (hundreds) | Lymphocytes |
| Protein | Very high (>1g/L) | Mildly elevated | High |
| Glucose | Very low (<1/2 blood) | Normal | Low |
| Gram stain | Positive | Negative | AFB (sometimes) |
PART 4 - PRACTICAL PROCEDURES (Watch Then Assist)
These are the most common procedures done on wards. You will observe first, then assist:
| Procedure | What it is | What to prepare |
|---|---|---|
| IV cannulation | Insert IV line | Gloves, tourniquet, IV cannula (18-20G usually), flush, dressing |
| Venipuncture | Blood sample | Gloves, tourniquet, needle, correct colored tubes |
| NG tube insertion | Tube through nose to stomach | NGT (10-16 Fr), lubricant, stethoscope, 20mL syringe |
| Urinary catheterization | Foley catheter into bladder | Sterile kit, appropriate size catheter (14-16 Fr for adults) |
| Pleural tap (thoracocentesis) | Drain fluid from chest | Large syringe, wide-bore needle, USS guidance ideally |
| Ascitic tap | Drain fluid from abdomen | Like pleural tap but abdomen, USS guidance |
| Blood transfusion | Give packed red cells | Crossmatch done, blood group checked, consent, pre-transfusion vitals |
Blood Transfusion - Safety Steps (MUST follow every time):
Before hanging blood:
- Two nurses check at bedside: patient name, hospital number, blood group, expiry date
- Check for patient identity band - matches blood product label
- Take pre-transfusion baseline vitals
- Each unit runs over 4 hours (unless emergency)
- Check vitals 15 min after starting (most reactions happen early)
Transfusion reactions:
| Reaction | When | Signs | Action |
|---|---|---|---|
| Febrile non-hemolytic | During/after | Fever, chills | Stop transfusion briefly, paracetamol, restart slowly |
| Allergic/urticarial | During | Rash, itch | Stop, chlorphenamine (antihistamine) |
| Anaphylaxis | Immediately | Hypotension, wheeze, rash | Stop immediately, adrenaline 0.5mg IM, call senior |
| ABO incompatibility (hemolytic) | First 15 min | Fever, loin pain, hemoglobinuria (red urine), shock | Stop immediately - life-threatening |
PART 5 - DISCHARGE PLANNING (Happens in All Wards)
Before a patient is discharged, these need to be done:
| Task | Who does it | You can help with |
|---|---|---|
| Discharge summary written | Doctor | Draft on paper for review |
| Medications prescribed for home | Doctor | Check drug names and doses |
| Follow-up appointment booked | Ward clerk / you | Know which OPD to refer to |
| Patient educated | Nurse + Doctor | Explain what to expect at home |
| Red flags explained | Doctor | When to come back to ER |
| Referrals made | Doctor | Physio, OT, social worker if needed |
THE MASTER CHECKLIST - For Every Patient, Every Day
BEFORE ROUNDS:
□ Check vitals chart (last 24 hours)
□ Check urine output
□ Check input/output balance
□ Read nursing notes for overnight events
□ Know today's investigation results
ON ROUNDS:
□ Present patient in SOAP format
□ Know what's being planned for today
□ Write down any new orders or changes
AFTER ROUNDS:
□ Note down 1 new thing you learned
□ Ask "what does this finding/result mean?"
□ Look up any term you didn't understand
END OF DAY:
□ Update your progress note
□ Check evening vitals
□ Confirm handover done
QUICK EMERGENCY REFERENCE - Stick This on Your Pocket Card
PATIENT SUDDENLY DETERIORATES:
→ ABCDE approach
→ Call senior immediately
→ High-flow O2 via non-rebreather mask
→ IV access × 2, blood tests
→ ECG, CXR, ABG
HYPOGLYCEMIA (<70 mg/dL):
→ 15g glucose (3 glucose tablets / 150mL juice)
→ Recheck in 15 min
→ If unconscious: 25mL of 50% dextrose IV
ANAPHYLAXIS:
→ Stop trigger, call help
→ Adrenaline 0.5mg IM (lateral thigh)
→ O2 high flow, IV access, fluids
SEIZURE:
→ Position safely, lateral
→ Time it
→ Diazepam if >5 minutes
→ Check glucose
CARDIAC ARREST:
→ Shout for help + call crash team
→ Start CPR: 30 compressions : 2 breaths
→ Get defibrillator
→ Do not stop until team arrives
That covers every major inpatient department. As you rotate through each one, come back and ask me about specific conditions or patients you saw - I'll break it down for that exact situation.
Sources: Schwartz's Principles of Surgery 11th Ed, Harrison's Internal Medicine 22nd Ed, Washington Manual of Medical Therapeutics, Goldman-Cecil Medicine, Bailey & Love's Surgery 28th Ed
General medicine
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
That is your full General Medicine module. Here is a quick summary of what's covered:
11 Core Conditions:
- Diabetes - Types, diagnosis, DKA, HHS, hypoglycemia, complications
- Hypertension - Classification, target organ damage, drug choices, emergencies
- Pneumonia - CURB-65, organisms, antibiotics
- Tuberculosis - Symptoms, diagnosis, HRZE treatment, DOTS
- Dengue - Phases, warning signs, NS1/IgM, fluid management
- Anemia - Micro/Normo/Macrocytic classification, blood film
- Acute Kidney Injury - Pre/intra/post-renal, hyperkalemia treatment
- Liver disease - Jaundice types, cirrhosis complications (ascites, SBP, encephalopathy)
- Asthma & COPD - Exacerbation management, O2 targets
- Sepsis - qSOFA, Sepsis Six
- Electrolytes - Hyponatremia, hypo/hyperkalemia
Practical tools included: Morning pre-round checklist, lab values reference, top ward drugs, emergency pocket card.
Tell me which condition you are seeing today on the ward and I will go deeper on it.
Continue the above one
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Excellent - I have strong content from Goldman-Cecil Medicine, Lippincott Pharmacology, and Harrison's. Here is the continuation:
🏥 GENERAL MEDICINE - CONTINUED
Part 2 | Conditions 12 to 20
CONDITION 12 - THYROID DISEASE
(Source: Lippincott Illustrated Reviews - Pharmacology)
Quick Anatomy of Thyroid Hormone Axis:
Hypothalamus → TRH
↓
Pituitary → TSH
↓
Thyroid gland → T3 + T4
Key lab test: TSH
- TSH HIGH → Thyroid not making enough → Hypothyroidism
- TSH LOW → Thyroid making too much → Hyperthyroidism
- TSH is always the FIRST test to order
HYPOTHYROIDISM
Causes:
| Cause | Notes |
|---|---|
| Hashimoto's thyroiditis | Most common in developed countries; autoimmune, anti-TPO antibodies |
| Iodine deficiency | Most common worldwide (endemic goiter) |
| Post-radioactive iodine treatment | Iatrogenic |
| Post-thyroidectomy | Surgical removal |
| Drugs | Amiodarone, lithium, interferon |
Symptoms - "SLOW":
- S - Slow metabolism: weight gain, constipation, bradycardia, slow reflexes
- L - Low temperature tolerance: cold intolerance, feeling always cold
- O - Other: dry skin, hair loss, puffy face/eyes (myxedema), hoarse voice
- W - Weakness: fatigue, lethargy, muscle cramps, depression, poor memory
Signs on examination:
- Bradycardia
- Dry, coarse skin
- Non-pitting periorbital edema (myxedema)
- Slow-relaxing (hung-up) tendon reflexes
- Goiter (enlarged thyroid) if due to iodine deficiency or Hashimoto's
- Macroglossia (large tongue)
Investigations:
- TSH: HIGH (most sensitive test)
- Free T4: LOW
- Anti-TPO antibodies: positive in Hashimoto's
- CBC: may show macrocytic anemia
- Lipids: often elevated (hypothyroidism raises LDL)
- ECG: bradycardia, low voltage, flattened T waves
Treatment:
- Levothyroxine (T4) - synthetic thyroid hormone
- Starting dose: 25-50 mcg OD (start low especially in elderly/cardiac patients - can precipitate angina)
- Take on empty stomach, 30-60 minutes before food
- Increase by 25 mcg every 6-8 weeks
- Monitor TSH 6-8 weeks after any dose change
- Target TSH: 0.5-2.5 mIU/L
Myxedema Coma (Extreme Hypothyroidism - Emergency):
- Severely ill, unconscious, hypothermic, bradycardic
- Precipitated by: cold exposure, infection, sedative drugs
- Treatment: IV T4 + IV hydrocortisone + warming + ICU
HYPERTHYROIDISM
Causes:
| Cause | Notes |
|---|---|
| Graves' disease | Most common; autoimmune, TSH receptor antibodies (TRAb); exophthalmos |
| Toxic multinodular goiter | Older patients, nodular thyroid |
| Toxic adenoma | Single hot nodule |
| Subacute thyroiditis | Painful thyroid, transient hyperthyroidism then hypothyroidism |
| Excess iodine (Jod-Basedow) | After contrast dye, amiodarone |
Symptoms - "FAST":
- F - Fast heart: palpitations, tachycardia, AF
- A - Anxious, agitated, tremor of hands, heat intolerance, sweating
- S - Slim down: weight loss despite good appetite, diarrhea
- T - Tired yet hyperactive: insomnia, weakness, menstrual irregularity
Graves' Disease Specific Signs:
- Exophthalmos (proptosis - bulging eyes) - pathognomonic
- Pretibial myxedema (thickened skin over shins)
- Diffuse smooth goiter with bruit
- Thyroid acropachy (clubbing - rare)
Investigations:
- TSH: LOW (suppressed, often undetectable)
- Free T3/T4: HIGH
- TRAb: positive in Graves'
- Thyroid scan (Tc-99m): Graves' = diffuse uptake; toxic adenoma = focal hot nodule
Treatment:
| Option | Drug/Procedure | Notes |
|---|---|---|
| Antithyroid drugs | Methimazole (carbimazole) or PTU | Euthyroid in 3-8 weeks; agranulocytosis is rare but serious side effect |
| Beta-blocker | Propranolol / atenolol | Controls symptoms FAST (tremor, palpitations) while waiting for antithyroid effect |
| Radioactive iodine (RAI) | I-131 | Destroys thyroid tissue; often leads to hypothyroidism eventually |
| Surgery | Thyroidectomy | For large goiter, compressive symptoms, failed drugs |
Thyroid Storm (Thyrotoxic Crisis) - Emergency:
- Extreme hyperthyroidism: very high temp, extreme tachycardia/AF, confusion, vomiting, heart failure
- Precipitated by: surgery, infection, trauma, contrast dye
- Treatment: High-dose methimazole + Lugol's iodine (blocks hormone release) + propranolol + steroids + treat precipitant + ICU
CONDITION 13 - PEPTIC ULCER DISEASE (PUD) & UPPER GI BLEED
Peptic Ulcer Disease
Definition: Break in mucosal lining of stomach or duodenum
| Gastric Ulcer | Duodenal Ulcer | |
|---|---|---|
| More common in | Older age, NSAIDs use | Younger patients, H. pylori |
| Pain timing | Worse 30-60 min AFTER food | Worse 2-3 hrs after food, relieved by eating ("hunger pain") |
| Weight | May lose weight (pain on eating) | Normal |
| H. pylori | 70% | 90% |
Causes:
- H. pylori (Helicobacter pylori) - most common cause worldwide
- NSAIDs (aspirin, ibuprofen, diclofenac) - inhibit prostaglandins that protect stomach
- Stress ulcers - critically ill patients in ICU
- Zollinger-Ellison syndrome - rare; gastrinoma causing massive acid production
Symptoms:
- Epigastric pain (burning/gnawing)
- Nausea, bloating
- Heartburn
- Complications: bleeding (hematemesis, melena), perforation (sudden severe pain), obstruction (persistent vomiting)
H. pylori Testing:
| Test | Notes |
|---|---|
| Urea breath test (UBT) | Best non-invasive; patient drinks labeled urea, bacteria break it down |
| Stool antigen test | Good non-invasive option |
| Biopsy (via endoscopy) | Gold standard; also gives histology |
| Serology (IgG) | Positive = past or present infection, not useful for test-of-cure |
H. pylori Eradication (Triple Therapy × 14 days):
- PPI (omeprazole 20mg BD) + Amoxicillin 1g BD + Clarithromycin 500mg BD
- If penicillin allergy: Replace amoxicillin with metronidazole
- Confirm eradication 4 weeks after completing antibiotics with UBT or stool antigen
Acid Suppression Drugs:
| Drug class | Example | How it works |
|---|---|---|
| PPI (proton pump inhibitor) | Omeprazole, pantoprazole, esomeprazole | Irreversibly blocks H+/K+ ATPase pump - most effective |
| H2 blocker | Ranitidine, famotidine | Blocks H2 receptor on parietal cell |
| Antacids | Magnesium hydroxide, aluminum hydroxide | Neutralizes acid (fast but short acting) |
| Sucralfate | Sucralfate | Coats ulcer base |
| Misoprostol | Misoprostol | Prostaglandin analog - protects mucosa (used with NSAIDs) |
Upper GI Bleed (UGIB)
Definition: Bleeding proximal to the ligament of Treitz (stomach + duodenum + lower esophagus)
Presentation:
- Hematemesis = vomiting blood (bright red = active; coffee-ground = older blood)
- Melena = black, tarry, offensive-smelling stools (blood digested in upper GI)
- Hematochezia (bright red rectal bleeding) only if very massive UGIB
Causes:
| Cause | Clue |
|---|---|
| Peptic ulcer (most common - 50%) | History of NSAIDs, H. pylori, epigastric pain |
| Esophageal varices | Cirrhotic patient, portal hypertension, large UGIB |
| Mallory-Weiss tear | Retching/vomiting before blood |
| Gastritis/erosions | NSAID use, alcohol, stress |
| Esophagitis | GERD, dysphagia |
Glasgow-Blatchford Score (Pre-endoscopy risk score):
Calculated from: BUN, Hb, systolic BP, pulse, presence of melena/syncope/liver disease/heart failure
- Score 0 = low risk → outpatient management possible
- Score ≥7 → needs urgent endoscopy and likely intervention
Immediate Management of UGIB:
ABCDE FIRST - assess stability
↓
IV access × 2 (large bore, 16G+)
↓
Blood tests: CBC, LFT, KFT, coagulation, GROUP & CROSSMATCH
↓
IV fluids - Ringer's Lactate / Normal saline
↓
Blood transfusion if Hb <8 g/dL (or <10 if cardiac patient)
↓
IV PPI: Pantoprazole 80mg bolus, then 8mg/hr infusion
↓
Urgent endoscopy (within 24h, within 12h if high risk)
↓
If varices: IV terlipressin + antibiotics (ceftriaxone - SBP prophylaxis)
Rockall Score (post-endoscopy risk):
Scores age, shock, comorbidity, diagnosis, endoscopic findings
- Score >5 = high rebleed/mortality risk
CONDITION 14 - URINARY TRACT INFECTION (UTI)
Types:
| Type | Site | Symptoms | Severity |
|---|---|---|---|
| Cystitis | Bladder | Dysuria, frequency, urgency, suprapubic pain | Lower UTI - mild |
| Pyelonephritis | Kidney + pelvis | Above + fever, loin/flank pain, rigors, nausea | Upper UTI - serious |
| Prostatitis | Prostate (men) | Perineal pain, difficulty urinating, tender prostate | Can be severe |
| Asymptomatic bacteriuria | Any | No symptoms, bacteria in urine | Treat only in pregnancy |
Risk Factors:
- Female sex (short urethra)
- Sexual activity ("honeymoon cystitis")
- Pregnancy (always treat even if asymptomatic)
- Urinary catheter (most common hospital infection)
- Obstruction (BPH, stones)
- Diabetes
- Immunocompromised
Diagnosis:
- Urine dipstick: Nitrites (bacteria convert nitrates) + Leucocyte esterase (WBCs) = likely UTI
- Urine microscopy: WBCs >5/HPF (pyuria), bacteria, RBCs
- Urine culture & sensitivity (C&S): Gold standard - identifies organism + antibiotic sensitivity (results take 24-48 hours)
- Send urine before starting antibiotics
Common Organisms:
- E. coli - 80% of uncomplicated UTI
- Klebsiella, Proteus, Pseudomonas (especially in hospital/catheter-associated)
- Staphylococcus saprophyticus - young sexually active women
- Enterococcus - in complicated/hospital UTI
Treatment:
| Type | Drug | Duration |
|---|---|---|
| Uncomplicated cystitis (women) | Nitrofurantoin 100mg BD or Trimethoprim 200mg BD | 3-5 days |
| Pyelonephritis (oral) | Ciprofloxacin 500mg BD or Co-amoxiclav 625mg TDS | 7-14 days |
| Pyelonephritis (IV - admitted) | Ceftriaxone 1-2g OD IV or Gentamicin | Until afebrile 24-48h, then switch oral |
| Catheter-associated UTI | Treat only if symptomatic; change catheter first | 5-7 days |
| Pregnancy (any bacteriuria) | Cephalexin or Nitrofurantoin (avoid in 3rd trimester) | 7 days |
Note: Nitrofurantoin - avoid in pyelonephritis (poor tissue penetration) and CKD (GFR <45)
CONDITION 15 - MALARIA
Very common cause of fever in tropical countries. Always think of it.
Plasmodium Species:
| Species | Clinical severity | Special features |
|---|---|---|
| P. falciparum | Most dangerous - can be fatal | Cerebral malaria, severe anemia, respiratory distress |
| P. vivax | Relapses (liver dormant form - hypnozoite) | Treat with primaquine to prevent relapse |
| P. ovale | Like vivax, relapses | Primaquine needed |
| P. malariae | Mild, can persist for years | Quartan fever (48h cycle) |
Classic Presentation:
- Periodicity of fever: P. falciparum = irregular; P. vivax/ovale = every 48h (tertian); P. malariae = every 72h (quartan)
- Rigors (shaking chills) → high fever → profuse sweating → resolution (cold-hot-sweat cycle)
- Headache, myalgia, nausea
- Splenomegaly (chronic malaria)
- Jaundice, anemia (destruction of RBCs)
Complications of Severe Falciparum Malaria:
- Cerebral malaria: Seizures, altered consciousness, coma
- Blackwater fever: Massive hemolysis → hemoglobinuria (dark/black urine)
- Severe anemia (Hb <7)
- Hypoglycemia (especially in children, pregnant women)
- Acute lung injury / Pulmonary edema
- AKI
Diagnosis:
- Peripheral blood smear (thick + thin smear): Gold standard; identifies species and parasite density
- Thick film: better for detecting parasites (screening)
- Thin film: identifies species (diagnosis)
- Rapid diagnostic test (RDT/ICT): Quick, good for P. falciparum (HRP2 antigen)
- Quantitative buffy coat (QBC)
Treatment:
| Type | Treatment |
|---|---|
| Uncomplicated P. falciparum | Artemisinin-based combination therapy (ACT): Artemether-lumefantrine (Coartem) or AS+AQ |
| Severe/complicated falciparum | IV Artesunate (preferred) or IV quinine + doxycycline |
| P. vivax/ovale (blood stage) | Chloroquine (where sensitive) or ACT |
| P. vivax/ovale (liver - prevent relapse) | Primaquine 15mg OD × 14 days (check G6PD first - primaquine causes hemolysis in G6PD deficiency) |
CONDITION 16 - DEEP VEIN THROMBOSIS (DVT) & PULMONARY EMBOLISM (PE)
DVT - Blood Clot in Deep Vein (usually leg)
Risk Factors - Virchow's Triad:
| Component | Risk factors |
|---|---|
| Stasis | Bed rest, long flight, immobilization, heart failure |
| Hypercoagulability | Malignancy, pregnancy, OCP, thrombophilia, post-surgery |
| Vessel injury | Trauma, surgery, IV catheter |
Symptoms of DVT:
- Unilateral leg swelling (one leg much bigger than other)
- Warmth, redness, tenderness along vein
- Homan's sign (calf pain on dorsiflexion) - not reliable
- Calf circumference >3 cm difference between legs = significant
Wells DVT Score:
Give points: active cancer (+1), paralysis/immobility (+1), bedridden >3 days/surgery in 4 weeks (+1), tenderness along vein (+1), entire leg swollen (+1), calf swelling >3cm (+1), pitting edema (+1), previous DVT (+1), alternative diagnosis likely (-2)
- Score ≥2 = DVT likely → do USS
- Score <2 = DVT unlikely → D-dimer first
Diagnosis:
- Compression USS (duplex): First line - non-compressibility of vein = DVT
- D-dimer: Sensitive but not specific - negative D-dimer rules out DVT if low pre-test probability
PE - Pulmonary Embolism (Clot in Lung Artery)
Clot travels from leg/pelvis vein → right heart → pulmonary artery → blocks lung circulation
Symptoms:
- Sudden breathlessness (most common)
- Pleuritic chest pain (sharp, worse on breathing)
- Hemoptysis (blood-stained sputum)
- Tachycardia
- Tachypnea
- Syncope (massive PE)
Wells PE Score (simplified):
- Clinical signs of DVT (+3)
- PE is #1 diagnosis (+3)
- HR >100 (+1.5)
- Immobilization >3 days / surgery in past 4 weeks (+1.5)
- Previous DVT/PE (+1.5)
- Hemoptysis (+1)
- Malignancy (+1)
Score >4 = PE likely; Score ≤4 = PE unlikely (do D-dimer)
ECG in PE:
- Sinus tachycardia (most common finding)
- S1Q3T3 pattern (S wave in lead I, Q wave + inverted T in lead III) - classic but not common
- Right heart strain: right axis deviation, RBBB, T-wave inversion V1-V4
CTPA (CT Pulmonary Angiogram): Gold standard for PE diagnosis
Treatment:
| Severity | Treatment |
|---|---|
| Low-moderate PE, stable | LMWH (enoxaparin) → transition to DOAC (rivaroxaban or apixaban) |
| High-risk/massive PE + hemodynamic instability | IV thrombolysis (alteplase 100mg over 2h) - systemic; surgical/catheter embolectomy |
| All PE patients | Anticoagulation for minimum 3 months (6+ months if unprovoked or cancer-related) |
DVT prophylaxis in all admitted patients:
- Enoxaparin 40mg SC once daily
-
- Ted stockings / intermittent pneumatic compression
- Early mobilization
CONDITION 17 - CELLULITIS & SKIN INFECTIONS
Definition: Bacterial infection of skin (dermis + subcutaneous tissue)
Presentation:
- Spreading redness, warmth, swelling, tenderness
- Fever, raised WBC
- Typically lower limbs
- Entry point: minor wound, tinea pedis (athlete's foot), insect bite
Organisms:
- Streptococcus pyogenes (Group A Strep): Most common
- Staphylococcus aureus: Especially MRSA (methicillin-resistant)
- Diabetic foot: often polymicrobial
Grading Severity:
| Grade | Features | Treatment |
|---|---|---|
| 1 (mild) | No systemic illness, no comorbidities | Oral flucloxacillin or cefalexin |
| 2 (moderate) | Systemic signs (fever, raised WBC) | IV antibiotics, consider admission |
| 3 (severe) | Severe systemic illness, spreading rapidly | IV antibiotics, surgical review |
| 4 (life-threatening) | Sepsis + necrotizing fasciitis | Emergency surgical debridement + broad spectrum IV ABx |
Mark the Borders:
- Use a skin marker to draw the edge of redness when patient admitted
- Reassess in 6-12 hours: redness spreading beyond line = treatment not working
- Redness staying within line / reducing = improving
Necrotizing Fasciitis (Flesh-eating infection - Emergency):
- Rapidly spreading infection along fascial planes
- Disproportionate pain (pain much worse than appearance)
- Crepitus (gas under skin - feel crackling)
- Skin discoloration → black necrosis
- Treatment: Emergency surgical debridement + broad-spectrum IV ABx (meropenem + clindamycin + vancomycin) + ICU
CONDITION 18 - EPILEPSY & SEIZURES
Types of Seizures (ILAE Classification):
Focal (Partial) Seizures - Start in one area of brain:
- Simple focal: Conscious throughout - twitching of one limb, abnormal smell/taste
- Complex focal: Impaired consciousness - blank staring, automatisms (lip smacking, picking)
- Focal to bilateral tonic-clonic: Starts focal, spreads to whole brain
Generalized Seizures - Involve whole brain from start:
| Type | Features |
|---|---|
| Tonic-clonic ("grand mal") | Rigid (tonic) → jerking (clonic) → post-ictal phase (confused, sleepy) |
| Absence ("petit mal") | Brief blank stare, no post-ictal; children, responsive to ethosuximide |
| Myoclonic | Brief muscle jerks, often in morning |
| Tonic | Sudden rigidity, falls |
| Atonic (drop attacks) | Sudden loss of muscle tone → falls |
Status Epilepticus - Medical Emergency:
Definition: Seizure lasting >5 minutes OR 2+ seizures without recovery between them
Treatment (timed):
| Time | Action |
|---|---|
| 0-5 min | ABCDE, O2, position lateral (recovery), IV access, check BGL |
| 5 min | First-line: Lorazepam 0.1 mg/kg IV (or diazepam 10mg IV/PR) |
| 10 min | If no response: repeat benzodiazepine |
| 20-30 min | Second-line: Levetiracetam 60 mg/kg IV OR phenytoin 20 mg/kg IV OR valproate 40 mg/kg IV |
| 40+ min | Third-line: Anaesthesia (midazolam/propofol infusion) - ICU, ventilation |
Investigations after first seizure:
- BGL (hypoglycemia causes seizures)
- Na, Ca, Mg (electrolyte seizures)
- Toxicology (drug/alcohol related)
- CT brain (rule out structural cause)
- MRI brain (better for hippocampal sclerosis, cortical dysplasia)
- EEG (electroencephalogram) - identifies epileptiform activity
Common Antiepileptic Drugs (AEDs):
| Drug | Best for | Side effects to know |
|---|---|---|
| Sodium valproate | All seizure types, first line generalized | Weight gain, hair loss, tremor, teratogenic (spina bifida) - AVOID in women of childbearing age |
| Carbamazepine | Focal seizures | Diplopia, ataxia, hyponatremia, induces liver enzymes |
| Lamotrigine | Focal + generalized | Rash (Stevens-Johnson syndrome if started too fast) |
| Levetiracetam | All types (widely used now) | Mood changes, depression - safe in pregnancy |
| Phenytoin | Status epilepticus, focal | Zero-order kinetics (small dose changes → big level changes), gum hyperplasia, hirsutism, nystagmus |
| Ethosuximide | Absence seizures only | GI upset |
CONDITION 19 - NEPHROTIC & NEPHRITIC SYNDROME
(Source: Harrison's Internal Medicine + Comprehensive Clinical Nephrology)
Two Key Glomerular Syndromes - Know the Difference:
| Feature | NEPHROTIC | NEPHRITIC |
|---|---|---|
| Proteinuria | Massive (>3.5g/day) | Mild to moderate |
| Haematuria | No (or minimal) | YES - characteristic |
| Oedema | Massive (face, legs, ascites) | Mild-moderate |
| Blood pressure | Normal or low | HIGH (hypertension) |
| Albumin | LOW (lost in urine) | Normal |
| Cholesterol | HIGH (compensatory) | Normal/mildly raised |
Nephrotic Syndrome:
Triad: Massive proteinuria + hypoalbuminemia + oedema
+ Hyperlipidemia + lipiduria (fatty casts in urine)
Causes:
| Primary (kidney disease) | Secondary (systemic disease) |
|---|---|
| Minimal change disease (children) | Diabetes (most common secondary cause) |
| Membranous nephropathy (adults) | Lupus (SLE) |
| FSGS (focal segmental glomerulosclerosis) | Amyloidosis |
Complications:
- Thrombosis (loss of antithrombin III in urine) → DVT, renal vein thrombosis
- Infections (loss of immunoglobulins) → pneumococcal, gram-negative
- Hyperlipidemia → cardiovascular risk
Treatment:
- Steroids (prednisolone 1mg/kg/day) - especially minimal change disease (remits well)
- ACEi/ARB (reduces proteinuria)
- Diuretics for edema
- Statins for hyperlipidemia
- Treat underlying cause
Nephritic Syndrome:
Classic presentation: Haematuria + proteinuria + hypertension + oliguria + oedema
Causes to know:
| Cause | Clue |
|---|---|
| Post-streptococcal GN | Child, 1-3 weeks after throat/skin Strep infection, low C3 |
| IgA nephropathy (Berger's) | Haematuria during/after URTI (synpharyngitic) |
| Lupus nephritis | Young woman + rash + joints + renal involvement |
| Goodpasture's (anti-GBM) | Haemoptysis + haematuria (lung-kidney syndrome) |
| ANCA vasculitis (GPA, MPA) | Multi-system, ANCA positive |
CONDITION 20 - CHRONIC KIDNEY DISEASE (CKD)
Definition: Kidney damage OR GFR <60 mL/min/1.73m² for >3 months
GFR Staging:
| Stage | GFR | Kidney function |
|---|---|---|
| G1 | >90 | Normal/high - but kidney damage present |
| G2 | 60-89 | Mildly reduced |
| G3a | 45-59 | Mildly-moderately reduced |
| G3b | 30-44 | Moderately-severely reduced |
| G4 | 15-29 | Severely reduced |
| G5 | <15 | Kidney failure (need dialysis/transplant) |
Causes:
- Diabetic nephropathy (most common worldwide)
- Hypertensive nephropathy
- Glomerulonephritis
- Obstructive uropathy (stones, BPH)
- Polycystic kidney disease (PKD)
- Recurrent infections
CKD Complications - Know All:
| Complication | Mechanism | Treatment |
|---|---|---|
| Anemia | Low erythropoietin (EPO) | EPO injections (darbepoetin), IV iron |
| Hypertension | Fluid retention + RAAS activation | ACEi/ARB (also slows progression), diuretics |
| Hyperkalemia | Reduced K+ excretion | Low K diet, stop ACEi if K>6, resonium, dialysis |
| Metabolic acidosis | Can't excrete H+ | Sodium bicarbonate tablets |
| Hyperphosphatemia | Reduced phosphate excretion | Phosphate binders (calcium carbonate/sevelamer) |
| Secondary hyperparathyroidism | Low Ca + high PO4 → PTH rises → bone disease | Active vitamin D (calcitriol), cinacalcet |
| Fluid overload | Can't excrete water | Fluid restriction, diuretics, dialysis |
| Uremia (end-stage symptoms) | Toxin accumulation | Dialysis |
Uremia Symptoms (End-Stage CKD):
- Nausea, anorexia, vomiting
- Pruritus (itch all over - urea deposits in skin)
- Encephalopathy (confusion, asterixis)
- Pericarditis (uremic pericarditis)
- Platelet dysfunction → bleeding tendency
- Metallic taste in mouth
Dialysis - Types:
| Hemodialysis (HD) | Peritoneal Dialysis (PD) | |
|---|---|---|
| How | Blood filtered through machine | Fluid put into abdomen, uses peritoneum as membrane |
| Frequency | 3× per week, 4h sessions | Daily (CAPD) or nightly (APD) |
| Access | AV fistula (surgically created) | PD catheter in abdomen |
| Where | Hospital or satellite unit | At home |
GENERAL MEDICINE MASTER DRUG CHART (Complete)
| Drug | Class | Use | Important Points |
|---|---|---|---|
| Levothyroxine | Thyroid hormone | Hypothyroidism | Empty stomach, check TSH 6-8 wks |
| Methimazole / Carbimazole | Antithyroid | Hyperthyroidism | Check WBC (agranulocytosis) |
| Propranolol | Beta-blocker | Symptom control in hyperthyroidism | Also used in portal HTN (varices) |
| Omeprazole / Pantoprazole | PPI | Ulcers, GERD, upper GI bleed | Before meals for best effect |
| Amoxicillin+Clarithromycin+PPI | Triple therapy | H. pylori eradication | 14 days |
| Terlipressin | Vasoconstrictor | Variceal bleed, hepatorenal syndrome | Monitor for ischaemia |
| Artemether-lumefantrine | ACT | Malaria (P. falciparum) | With food for better absorption |
| Primaquine | Antimalarial | P. vivax relapse prevention | Check G6PD first |
| Enoxaparin (LMWH) | Anticoagulant | DVT/PE treatment and prophylaxis | Reduce dose in CKD |
| Rivaroxaban/Apixaban | DOAC | DVT/PE, AF | No monitoring needed (unlike warfarin) |
| Alteplase (tPA) | Thrombolytic | Massive PE, STEMI | Risk of major bleeding |
| Flucloxacillin / Cefalexin | Antibiotic | Cellulitis (Strep/Staph) | Standard first-line |
| Vancomycin | Antibiotic | MRSA infections | Monitor levels, nephrotoxic |
| Lorazepam / Diazepam | Benzodiazepine | Seizures / status epilepticus | Respiratory depression |
| Sodium valproate | AED | Epilepsy (all types) | Teratogenic - avoid in young women |
| Levetiracetam | AED | Epilepsy | Good safety profile, IV available |
| Prednisolone | Steroid | Nephrotic syndrome, asthma, autoimmune | Hyperglycemia, infection, osteoporosis |
| Erythropoietin (EPO) | Growth factor | CKD anaemia | Monitor Hb, risk of hypertension |
| Calcium carbonate | Phosphate binder | CKD hyperphosphatemia | Give WITH meals |
| Calcitriol | Active Vit D | CKD bone disease | Monitor Ca levels |
| Sodium bicarbonate | Alkali | CKD metabolic acidosis | Oral tablets daily |
| Nitrofurantoin | Antibiotic | Uncomplicated UTI | Avoid in CKD, pyelonephritis |
| Ciprofloxacin | Antibiotic | Pyelonephritis, complicated UTI | Avoid in children, tendon rupture |
DAILY CHECKLIST FOR GENERAL MEDICINE - FULL VERSION
Questions to ask yourself about EVERY PATIENT, every day:
SYSTEM-BY-SYSTEM REVIEW:
METABOLIC:
□ If diabetic: BGL checked? Insulin given? Any hypo episodes overnight?
□ Thyroid patient: On levothyroxine? TSH pending?
CARDIOVASCULAR:
□ BP controlled? Which antihypertensive? Any chest pain?
□ If heart failure: weight? Fluid balance? Diuretic response?
RESPIRATORY:
□ SpO2? On O2? How many liters? Can we wean?
□ Fever + cough + consolidation on CXR? Start antibiotics?
RENAL:
□ Urine output >0.5 mL/kg/hr?
□ Creatinine trend? Rising or falling?
□ Any nephrotoxic drugs to stop?
INFECTIONS:
□ Are cultures back? Sensitivities match current antibiotic?
□ IV to oral switch possible? (afebrile 24-48h + tolerating oral)
□ Line sites clean? IV changed in last 72h?
HAEMATOLOGICAL:
□ Anaemia: Hb? Transfusion needed?
□ Thrombocytopenia: Dengue? DIC? TTP?
□ DVT prophylaxis ordered?
GI/LIVER:
□ Bowels moving? If liver disease: any encephalopathy signs (asterixis)?
□ On lactulose? How many stools/day?
MEDICATIONS:
□ Any drug interactions? Any to stop?
□ Renal dosing adjustments needed?
□ Anticoagulation (dose, monitoring)?
SOCIAL/DISCHARGE:
□ Improving enough for discharge?
□ Follow-up appointment needed?
□ Patient knows their diagnosis and medications?
THINGS SENIORS WILL ASK YOU ON ROUNDS (Be Ready)
| Question | Answer they expect |
|---|---|
| "What are the causes of jaundice?" | Pre-hepatic / Hepatic / Post-hepatic |
| "What is this patient's CURB-65 score?" | Calculate from RR, BP, BUN, confusion, age |
| "Why is this patient hyponatremic?" | Assess volume status → SIADH vs dehydration vs fluid overload |
| "What does this ECG show?" | Rate, rhythm, axis, P waves, PR, QRS, ST/T |
| "What is your differential for this fever?" | Think by system: chest? urine? line? wound? drugs? DVT? |
| "What next investigation would you order?" | Based on history - always explain WHY you're ordering it |
| "What is the treatment for DKA?" | Fluids + Insulin + Potassium + Treat cause |
| "How would you manage this GI bleed?" | ABCDE + IV access × 2 + Crossmatch + IV PPI + Endoscopy |
That completes the full General Medicine module (20 conditions).
Conditions covered across both parts:
- Diabetes (DKA, HHS, Hypoglycemia) | 2. Hypertension | 3. Pneumonia | 4. TB | 5. Dengue | 6. Anemia | 7. AKI | 8. Liver / Jaundice | 9. Asthma & COPD | 10. Sepsis | 11. Electrolytes | 12. Thyroid disease | 13. PUD & GI Bleed | 14. UTI | 15. Malaria | 16. DVT & PE | 17. Cellulitis | 18. Epilepsy | 19. Nephrotic & Nephritic | 20. CKD
Tell me which condition you encounter in the ward today - I'll go deeper on exactly that one.
Sources: Goldman-Cecil Medicine, Harrison's Internal Medicine 22nd Ed, Lippincott Pharmacology, Comprehensive Clinical Nephrology, Rosen's Emergency Medicine
Condition 11 not completed the info give that
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have all the detailed textbook content needed. Here is the complete Condition 11:
CONDITION 11 - ELECTROLYTE DISTURBANCES (COMPLETE)
Full Guide | All 7 Electrolytes
OVERVIEW - WHY ELECTROLYTES MATTER
Electrolytes run every cell in the body - heart rhythm, nerve conduction, muscle contraction, fluid balance. A single abnormal electrolyte can cause:
- Cardiac arrest (K+, Ca2+, Mg2+)
- Seizures (Na+, Ca2+, Mg2+)
- Muscle paralysis (K+, Mg2+)
- Coma (Na+)
Always check electrolytes: On admission, after starting IV fluids, after diuretics, in AKI, DKA, liver disease, and any critically ill patient.
ELECTROLYTE 1 - SODIUM (Na+) | Normal: 136-145 mEq/L
HYPONATREMIA (Na+ <135 mEq/L)
Most common electrolyte disorder in hospitalized patients
Symptoms (depend on speed of fall, not just level):
| Na+ Level | Symptoms |
|---|---|
| 130-135 | Usually asymptomatic |
| 125-130 | Nausea, headache, malaise |
| 120-125 | Confusion, disorientation |
| <120 | Seizures, coma, death |
Acute hyponatremia (<48 hours): Dangerous even at moderate levels - brain swells rapidly
Chronic hyponatremia (>48 hours): Brain adapts - symptoms less severe
Step 1: Assess the patient's VOLUME STATUS (the most important step)
Look at the patient:
- Dry mouth, low BP, tachycardia, reduced skin turgor → HYPOVOLEMIC
- Normal examination → EUVOLEMIC
- Oedema, ascites, raised JVP → HYPERVOLEMIC
Causes by Volume Status:
| Volume Status | Condition | Key Clue |
|---|---|---|
| Hypovolemic (dry, losing fluid) | Vomiting/diarrhea, diuretics (especially thiazides), Addison's disease | Urine Na >20 if kidneys losing it (diuretics, Addison); Urine Na <20 if extra-renal loss (diarrhea) |
| Euvolemic (normal volume) | SIADH (most common euvolemic cause), hypothyroidism, psychogenic polydipsia | High urine sodium (>40), high urine osmolality (>100 mOsm/kg) |
| Hypervolemic (oedematous) | Heart failure, cirrhosis, nephrotic syndrome | Dilutional hyponatremia - too much water, Na diluted out |
SIADH (Syndrome of Inappropriate ADH Secretion):
ADH = antidiuretic hormone = causes kidneys to retain water
In SIADH, ADH is released inappropriately → kidneys keep water → Na gets diluted
Causes of SIADH ("CCMDI"):
- CNS: meningitis, stroke, subarachnoid hemorrhage, head injury
- Chest: pneumonia, TB, lung cancer (small cell - most common malignancy cause)
- Malignancy: small cell lung cancer (secretes ADH ectopically)
- Drugs: carbamazepine, SSRIs (fluoxetine), morphine, cyclophosphamide, vincristine
- Idiopathic / Post-surgery
SIADH Diagnosis Criteria (all must be met):
- Serum Na <135 mEq/L (low serum osmolality <280)
- Urine osmolality >100 mOsm/kg (inappropriately concentrated)
- Urine Na >40 mEq/L (kidneys still losing Na)
- Normal thyroid and adrenal function (exclude hypothyroidism, Addison's)
- No diuretics, no volume depletion, no oedema
Treatment of Hyponatremia:
THE GOLDEN RULE: Never correct Na faster than 8-10 mEq/L in 24 hours
Correcting too fast → Osmotic Demyelination Syndrome (ODS) / Central Pontine Myelinolysis
- Myelin sheath around brainstem neurons is destroyed
- Results in: dysarthria (slurred speech), dysphagia, flaccid paralysis, coma
- Irreversible, devastating - especially in malnourished, alcoholics, elderly
(Source: Rosen's Emergency Medicine)
| Severity | Na level & Symptoms | Treatment |
|---|---|---|
| Mild/Chronic asymptomatic | Na 125-134, no symptoms | Treat underlying cause + fluid restriction 1000 mL/day (for SIADH) |
| Moderate | Na 115-124, nausea, confusion | Fluid restriction + cautious sodium correction |
| Severe/Symptomatic | Na <120 OR seizures/coma | 3% Hypertonic saline 100 mL IV over 10 min (can repeat × 2); raise Na by 4-6 mEq in first 6 hours |
3% hypertonic saline - only use when:
- Patient seizing OR
- GCS dropping OR
- Na <115 mEq/L
Special correction rules:
- In chronic hyponatremia (>48h): max correction 8 mEq/L in 24 hours
- In acute hyponatremia (<48h): can correct up to 1-2 mEq/L per hour
- Recheck Na every 2-4 hours when giving hypertonic saline
By cause:
| Cause | Specific treatment |
|---|---|
| Hypovolemic hyponatremia | Normal saline (replace volume) |
| SIADH | Fluid restriction 800-1000 mL/day; treat cause |
| Heart failure | Diuretics + treat heart failure |
| Cirrhosis | Albumin, treat underlying liver disease |
| Hypothyroidism | Levothyroxine (Na corrects as thyroid corrects) |
| Addison's disease | Hydrocortisone (emergency if in crisis) |
HYPERNATREMIA (Na+ >145 mEq/L)
Always means the patient has too little water relative to sodium
Causes:
- Water loss: Fever, sweating, burns, diabetes insipidus (DI), osmotic diuresis (DKA), diarrhea
- Inadequate water intake: Elderly, unconscious, infants who can't ask for water
- Salt excess (rare): IV hypertonic saline, excess sodium bicarbonate, sea water ingestion
Most common in wards: Elderly confused patient not drinking, or patient on NG tube without enough free water
Symptoms:
- Thirst (if conscious)
- Confusion, lethargy, irritability
- Weakness, tremors
- Seizures, coma (severe Na >155-160)
Treatment of Hypernatremia:
Also correct slowly - brain adapts to high Na. Too fast correction → cerebral edema
Free Water Deficit Formula:
(Source: Roberts and Hedges' Clinical Procedures)
Free water deficit = [(Na actual - 140) ÷ 140] × Total Body Water (TBW) TBW = 0.6 × body weight in kg
Example: 70kg man with Na 165 mEq/L
- TBW = 0.6 × 70 = 42 L
- Free water deficit = [(165-140) ÷ 140] × 42 = 7.5 L
Correct over 48-72 hours, max drop 10-12 mEq/L per 24 hours
Fluid of choice:
- Mild: Encourage oral water/feeds
- If IV needed: 5% Dextrose (D5W) or 0.45% NaCl (half-normal saline)
- Never give pure water IV - causes hemolysis
ELECTROLYTE 2 - POTASSIUM (K+) | Normal: 3.5-5.0 mEq/L
HYPERKALEMIA (K+ >5.5 mEq/L)
K+ >6.5 with ECG changes = CARDIAC EMERGENCY
Causes ("DREAD"):
- Drugs: ACEi, ARBs, spironolactone, NSAIDs, heparin, beta-blockers, digoxin toxicity
- Renal failure (AKI/CKD) - can't excrete K+
- Endocrine: Addison's disease (no aldosterone → K+ retained)
- Acidosis: H+ goes into cells, K+ comes out
- Destruction: rhabdomyolysis, tumor lysis syndrome, massive hemolysis, burns
ECG Changes (in order as K rises):
| K+ level | ECG Change |
|---|---|
| 5.5-6.0 | Tall, peaked, narrow, tented T waves |
| 6.0-6.5 | PR interval prolongation, P waves flatten |
| 6.5-7.0 | Wide QRS (>0.12 sec) |
| >7.0 | P waves disappear, sine-wave pattern |
| >8.0-9.0 | VF or asystole → cardiac arrest |
Treatment - Three Goals (from Fischer's Mastery of Surgery):
The treatment diagram from the textbook:
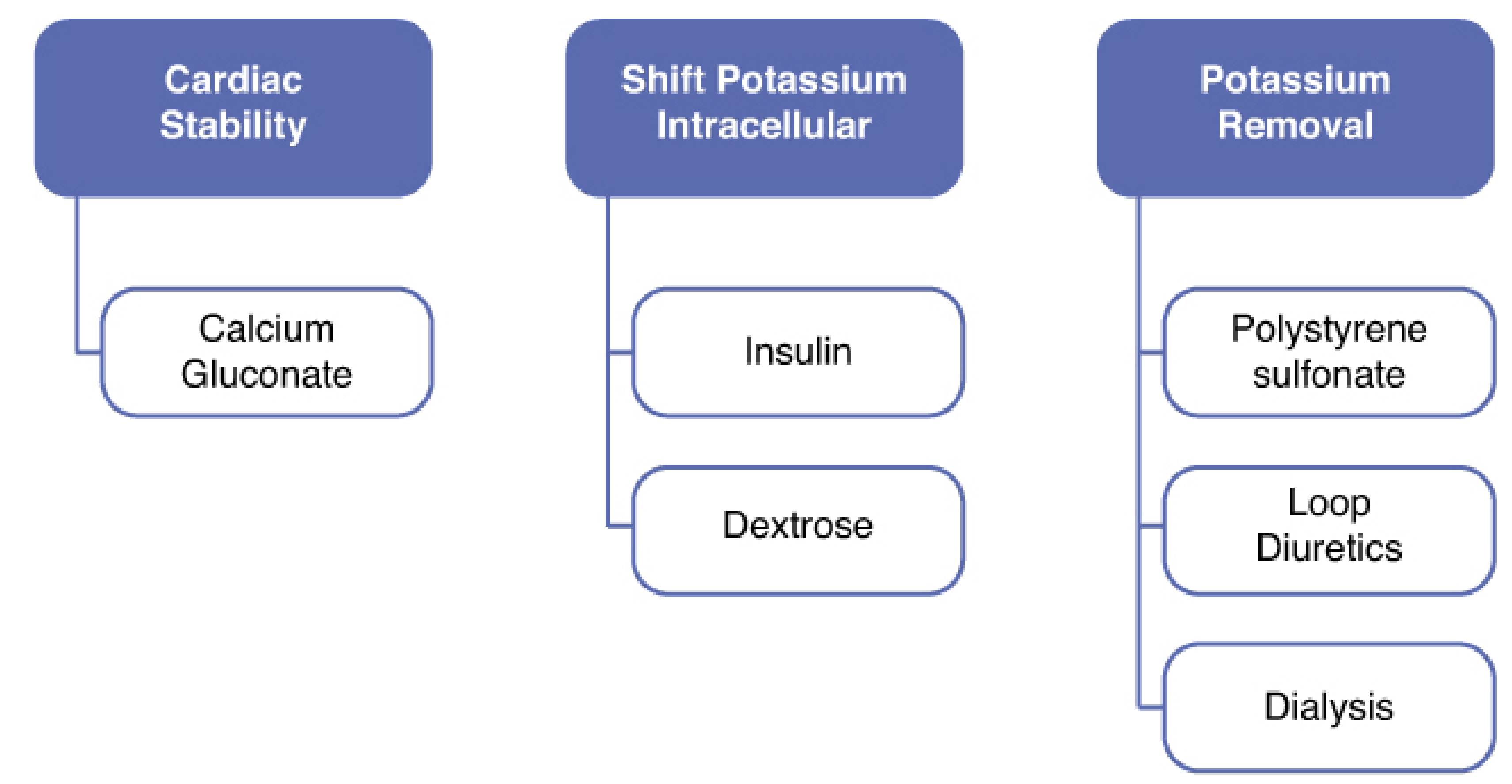
Step-by-step treatment:
| Goal | Drug | Dose | Onset | Duration | Mechanism |
|---|---|---|---|---|---|
| 1. Cardiac protection | Calcium gluconate 10% | 10 mL IV over 2-3 min | 2-3 min | 30-60 min | Stabilizes cardiac membrane - does NOT lower K+ |
| Repeat if no ECG improvement in 5-10 min | |||||
| 2. Shift K+ into cells | Insulin 10-20 units + Dextrose 50% 25-50g IV | Together over 15-30 min | 15-30 min | 4-6 hours | Insulin drives K+ into cells |
| Salbutamol (albuterol) nebulised 10-20mg | Over 30-60 min | 30 min | 2-4 hours | Beta-2 agonist shifts K+ intracellular | |
| Sodium bicarbonate IV | If metabolic acidosis present | 30-60 min | Hours | Corrects acidosis → K+ shifts in | |
| 3. Remove K+ from body | Calcium resonium (polystyrene sulfonate) | 15-30g oral or PR in water | Hours | Hours | Binds K+ in gut, excretes in stool |
| Furosemide 40-80mg IV | If urine output adequate | 30 min | Hours | Promotes renal K+ loss | |
| Dialysis | If renal failure / refractory | Immediate | Definitive | Physically removes K+ |
Important: Calcium gluconate does NOT lower potassium level - it only protects the heart while you wait for other drugs to work. Always give it FIRST if ECG changes present.
Chronic management:
- Low potassium diet (avoid: bananas, oranges, potatoes, tomatoes, dried fruits, nuts)
- Stop ACEi/ARBs if K+ consistently >6
- Newer agents: Patiromer (8.4g daily with food) or Sodium zirconium cyclosilicate
HYPOKALEMIA (K+ <3.5 mEq/L)
Causes:
| Mechanism | Causes |
|---|---|
| GI losses | Vomiting (loses K+ + H+ → alkalosis), diarrhea, laxative abuse, ileostomy |
| Renal losses | Diuretics (furosemide = most common, thiazides), hyperaldosteronism, Cushing's, RTA, amphotericin |
| Transcellular shift | Insulin therapy (DKA treatment), alkalosis, beta-2 agonists (salbutamol), hypothermia |
| Poor intake | Malnutrition, starvation, alcoholism |
Symptoms:
- Mild (3.0-3.5): Often asymptomatic
- Moderate (2.5-3.0): Fatigue, weakness, muscle cramps, constipation, palpitations
- Severe (<2.5): Flaccid paralysis (including respiratory muscles), rhabdomyolysis, ileus
ECG Changes in Hypokalemia:
- Flattening of T waves
- U waves (positive deflection after T wave - classic sign)
- ST depression
- Prolonged QU interval
- Severe: ventricular tachyarrhythmias (torsades de pointes)
Tip: U wave looks like an extra bump after the T wave, best seen in leads V4-V6
Treatment:
| Severity | Route | Dose | Notes |
|---|---|---|---|
| Mild (K 3.0-3.5), asymptomatic | Oral | KCl (Slow-K) 600-1200mg TDS or potassium-rich foods | Banana, orange juice, coconut water |
| Moderate (K 2.5-3.0) | Oral + consider IV | KCl supplements + IV if not tolerating oral | |
| Severe (<2.5) or symptomatic | IV | Add KCl 20-40 mEq to 1L NS/RL, max 10-20 mEq/hour via peripheral IV | NEVER bolus IV KCl - causes cardiac arrest |
ICU rate: Up to 40 mEq/hour via central line with continuous cardiac monitoring only
Always check Mg2+ in refractory hypokalemia - if Mg2+ is also low, K+ cannot be corrected until Mg2+ is replaced first (Mg2+ is needed for K+ reabsorption in kidney)
ELECTROLYTE 3 - CALCIUM (Ca2+) | Normal: 8.5-10.3 mg/dL
Important: Always correct for albumin level:
Corrected Ca2+ = Measured Ca2+ + [0.8 × (4.0 - albumin)]
Example: Ca = 7.5, albumin = 2.0 → Corrected Ca = 7.5 + [0.8 × (4.0-2.0)] = 7.5 + 1.6 = 9.1 (actually normal!)
HYPERCALCEMIA (Ca2+ >10.3 mg/dL)
(Source: Washington Manual of Medical Therapeutics)
Causes - 90% are from just 2 causes:
- Primary hyperparathyroidism - most common in outpatients; elevated PTH, usually asymptomatic, found on routine bloods
- Malignancy - most common in inpatients; PTH suppressed but PTHrP elevated; advanced cancer
Other causes (10%): Vitamin D excess, sarcoidosis and other granulomatous diseases, milk-alkali syndrome, thiazide diuretics, prolonged immobilization, Paget's disease
Symptoms - "Bones, Stones, Groans, Psychic Moans":
| Mnemonic | System | Symptoms |
|---|---|---|
| Bones | Skeletal | Bone pain, fractures, osteitis fibrosa cystica (in hyperparathyroidism) |
| Stones | Renal | Polyuria, polydipsia, kidney stones (Ca oxalate), nephrocalcinosis |
| Groans | GI | Nausea, vomiting, constipation, anorexia, peptic ulcer |
| Psychic Moans | Neurological | Fatigue, depression, confusion, stupor, coma (at >14 mg/dL) |
ECG in Hypercalcemia: Shortened QT interval (opposite of hypo)
Treatment:
| Severity | Treatment |
|---|---|
| Mild (Ca <12 mg/dL), asymptomatic | Stop offending drugs, increase oral fluids, treat underlying cause |
| Moderate (Ca 12-14 mg/dL) | IV fluids (normal saline 200-300 mL/hour) - hydration promotes Ca excretion |
| Severe (Ca >14 mg/dL) or symptomatic | IV NS aggressively + Furosemide (after rehydrated) + Bisphosphonate (zoledronic acid IV - gold standard for malignant hypercalcemia) |
| Malignancy-related | Zoledronic acid 4mg IV over 15 min - works in 24-48 hours |
| Granulomatous/Vitamin D excess | Steroids (hydrocortisone/prednisolone) - inhibit vitamin D activation |
HYPOCALCEMIA (Ca2+ <8.5 mg/dL, corrected)
Causes:
- Hypoparathyroidism - most commonly after thyroid/parathyroid surgery (check for Chvostek + Trousseau after any neck surgery)
- Vitamin D deficiency (very common - especially in sun-deprived populations, malnutrition)
- Hypomagnesemia - low Mg suppresses PTH
- Pancreatitis (fat saponification consumes Ca)
- CKD (impaired vitamin D activation, high phosphate)
- Massive blood transfusion (citrate chelates Ca)
Symptoms - "Neuromuscular excitability":
- Perioral tingling (numbness around lips)
- Tingling in hands and feet
- Muscle cramps → tetany (carpopedal spasm - hands/feet clench)
- Chvostek's sign: Tap facial nerve just in front of ear → facial muscle twitching
- Trousseau's sign: Inflate BP cuff on arm >SBP for 3 min → hand goes into carpal spasm (thumb adducts, fingers extend = "main d'accoucheur")
- Prolonged QT interval on ECG → torsades de pointes
- Seizures (severe hypocalcemia)
- Laryngospasm (emergency - airway obstruction)
Treatment:
| Severity | Treatment |
|---|---|
| Mild, asymptomatic | Oral calcium supplements (calcium carbonate 500mg-1g BD) + oral vitamin D |
| Moderate | Oral calcium + calcitriol (active Vit D) especially if hypoparathyroid |
| Symptomatic (tetany, seizures, laryngospasm) | 10 mL 10% calcium gluconate IV over 10 minutes (slow IV - cardiac monitoring) - can repeat; then maintenance infusion |
After neck surgery: Routinely check Ca 12-24 hourly for 48 hours. Give oral calcium prophylactically.
ELECTROLYTE 4 - MAGNESIUM (Mg2+) | Normal: 1.7-2.2 mg/dL (0.7-0.9 mmol/L)
(Source: Fischer's Mastery of Surgery)
Often overlooked but very important. Low Mg makes it impossible to correct K+ and Ca2+.
HYPOMAGNESEMIA (Mg2+ <1.7 mg/dL)
Causes:
- Diuretics (furosemide, thiazides) - most common hospital cause
- Chronic diarrhea, malabsorption
- Alcohol abuse (renal Mg wasting)
- Diabetes mellitus (renal loss)
- Drugs: aminoglycosides (gentamicin), proton pump inhibitors (long-term), digoxin, cisplatin
- Poor intake + refeeding
Symptoms:
- Mild: Causes other electrolyte disturbances (hypokalemia, hypocalcemia) - often only finding
- Severe:
- Neuromuscular: tremor, muscle cramps, positive Chvostek/Trousseau
- Neurological: confusion, seizures, heightened reflexes
- Cardiac: Torsades de Pointes (the arrhythmia most associated with low Mg - polymorphic VT with QT prolongation)
Key Point: Refractory Hypokalemia
If you keep replacing potassium but it won't go up → always check and replace Mg2+ first
Treatment:
- Mild/moderate: Oral magnesium oxide tablets or magnesium glycinate
- Severe / symptomatic: MgSO4 (Magnesium sulphate) 2g IV over 10-15 min (slowly, watch for bradycardia and hypotension) then maintenance infusion
- Torsades de Pointes: MgSO4 2g IV stat is first-line treatment
- Eclampsia: MgSO4 4g IV loading dose (different context - prevent seizures)
Note: Serum Mg can be normal even when total body stores are depleted - clinical suspicion is key.
HYPERMAGNESEMIA (Mg2+ >2.2 mg/dL)
(Source: Fischer's Mastery of Surgery)
Causes:
- Renal failure (can't excrete Mg)
- Massive Mg supplementation (especially in eclampsia treatment)
- Excessive antacids (Mg-containing: gaviscon, milk of magnesia)
- Adrenal insufficiency
Symptoms by Level:
| Mg level | Effect |
|---|---|
| 4-5 mEq/L | Loss of deep tendon reflexes (first sign to check!) |
| 5-7 mEq/L | Hypotension, bradycardia, nausea |
| 7-10 mEq/L | Respiratory paralysis |
| >10 mEq/L | Cardiac arrest (complete heart block) |
Monitoring MgSO4 in eclampsia patients: Check patellar reflex before every dose - if absent, STOP
Treatment:
- Stop Mg supplementation
- IV calcium gluconate (10 mL 10% over 3 min) - temporarily antagonizes Mg at membrane
- IV fluids + furosemide (promote renal Mg excretion)
- Severe/renal failure: Dialysis
ELECTROLYTE 5 - PHOSPHATE (PO4) | Normal: 2.5-4.5 mg/dL
HYPOPHOSPHATEMIA (PO4 <2.5 mg/dL)
Causes:
- Refeeding syndrome (MOST important ward cause)
- Malnutrition, malabsorption
- Antacid use (aluminum/Mg antacids bind phosphate in gut)
- DKA treatment (insulin drives PO4 into cells)
- Hyperparathyroidism
Refeeding Syndrome:
- Occurs when severely malnourished patient starts eating/receiving nutrition (oral, enteral, or parenteral)
- Carbohydrates in food → insulin release → K+, Mg2+, PO4 all rush into cells → all 3 drop suddenly
- Prevention: Feed slowly, start at 50% of target calories, supplement K/Mg/PO4 before and during feeding
Symptoms of Hypophosphatemia:
- Muscle weakness (including respiratory muscles → ventilator dependence)
- Confusion, seizures
- Hemolytic anemia
- Platelet dysfunction
Treatment:
- Mild: Oral phosphate supplements
- Severe: IV sodium/potassium phosphate infusion
HYPERPHOSPHATEMIA (PO4 >4.5 mg/dL)
Most common in CKD (kidneys can't excrete phosphate)
Treatment: Phosphate binders taken WITH meals to prevent GI absorption:
- Calcium carbonate (cheapest, also supplements Ca)
- Sevelamer (non-calcium binder - better in dialysis patients)
- Lanthanum carbonate
ELECTROLYTE QUICK REFERENCE TABLE
| Electrolyte | Normal | Low (Hypo) | High (Hyper) |
|---|---|---|---|
| Na+ | 136-145 mEq/L | <135: SIADH, heart failure, cirrhosis | >145: Dehydration, DI, fever |
| K+ | 3.5-5.0 mEq/L | <3.5: Diuretics, vomiting, diarrhea | >5.5: AKI, ACEi, acidosis |
| Ca2+ | 8.5-10.3 mg/dL | <8.5: Hypoparathyroid, Vit D deficiency | >10.3: Hyperparathyroid, malignancy |
| Mg2+ | 1.7-2.2 mg/dL | <1.7: Diuretics, alcohol, diarrhea | >2.2: Renal failure, excess Mg |
| PO4 | 2.5-4.5 mg/dL | <2.5: Refeeding, DKA treatment | >4.5: CKD, hypoparathyroid |
ECG SUMMARY - ELECTROLYTES AT A GLANCE
| Finding on ECG | Electrolyte | |
|---|---|---|
| Peaked T waves | High K+ | ↑K+ |
| Flattened T waves + U waves | Low K+ | ↓K+ |
| Short QT interval | High Ca2+ | ↑Ca2+ |
| Long QT interval | Low Ca2+, Low Mg2+ | ↓Ca2+ / ↓Mg2+ |
| Torsades de Pointes (polymorphic VT) | Low Mg2+, Low K+, Low Ca2+ | Emergency! |
| Wide QRS + sine wave | Severe high K+ | ↑↑K+ (cardiac emergency) |
ELECTROLYTE CORRECTION - THE CARDINAL RULES
RULE 1: SODIUM
→ Never correct Na+ faster than 8-10 mEq/L per 24 hours
→ Too fast = osmotic demyelination → permanent brain damage
RULE 2: POTASSIUM
→ NEVER push KCl IV (causes cardiac arrest)
→ Max peripheral IV rate: 10-20 mEq/hour
→ Always give Calcium gluconate FIRST if ECG changes present
→ Check Mg2+ if K+ won't correct
RULE 3: CALCIUM
→ Always correct for albumin before deciding it's abnormal
→ IV calcium gluconate (not calcium chloride) via peripheral - safer
→ Monitor for QT changes on ECG
RULE 4: MAGNESIUM
→ Check Mg2+ in any patient with unexplained hypokalemia or hypocalcemia
→ Torsades de Pointes = give MgSO4 2g IV immediately
→ Check patellar reflex before each dose in eclampsia treatment
RULE 5: PHOSPHATE
→ Refeeding syndrome - think of it in any malnourished patient getting nutrition
→ Replace K+, Mg2+, PO4 BEFORE starting feeds in malnourished patients
Condition 11 is now complete. All 5 electrolytes (Na, K, Ca, Mg, PO4) are fully covered with causes, symptoms, ECG changes, and treatment.
Sources: Washington Manual of Medical Therapeutics, Rosen's Emergency Medicine, Fischer's Mastery of Surgery 8th Ed, Roberts and Hedges' Clinical Procedures
This is a shared conversation. Sign in to Orris to start your own chat.