Are kasai procedure and roux en y hepaticojejunostony the same?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a thorough comparison based directly from the surgical textbooks:
Kasai Procedure vs. Roux-en-Y Hepaticojejunostomy
These two procedures are not the same, though they share a common element: both use a Roux-en-Y loop of jejunum for biliary drainage. The critical differences lie in the indication, anatomy of anastomosis, and the structure being connected.
Kasai Procedure (Portoenterostomy)
| Feature | Detail |
|---|---|
| Full name | Kasai portoenterostomy |
| Developed by | Morio Kasai (Japan, late 1950s) |
| Indication | Biliary atresia (absence/obliteration of extrahepatic bile ducts) |
| What is anastomosed | The porta hepatis (cut fibrous biliary remnant at the hilum) -- NOT a bile duct, because there is no patent duct |
| To what | A short Roux-en-Y jejunal limb (15-25 cm, retrocolic) |
| Age group | Neonates/infants (best results if done < 60 days of age) |
| Goal | Drain bile from microscopic bile ductules within the fibrous portal plate into the bowel |
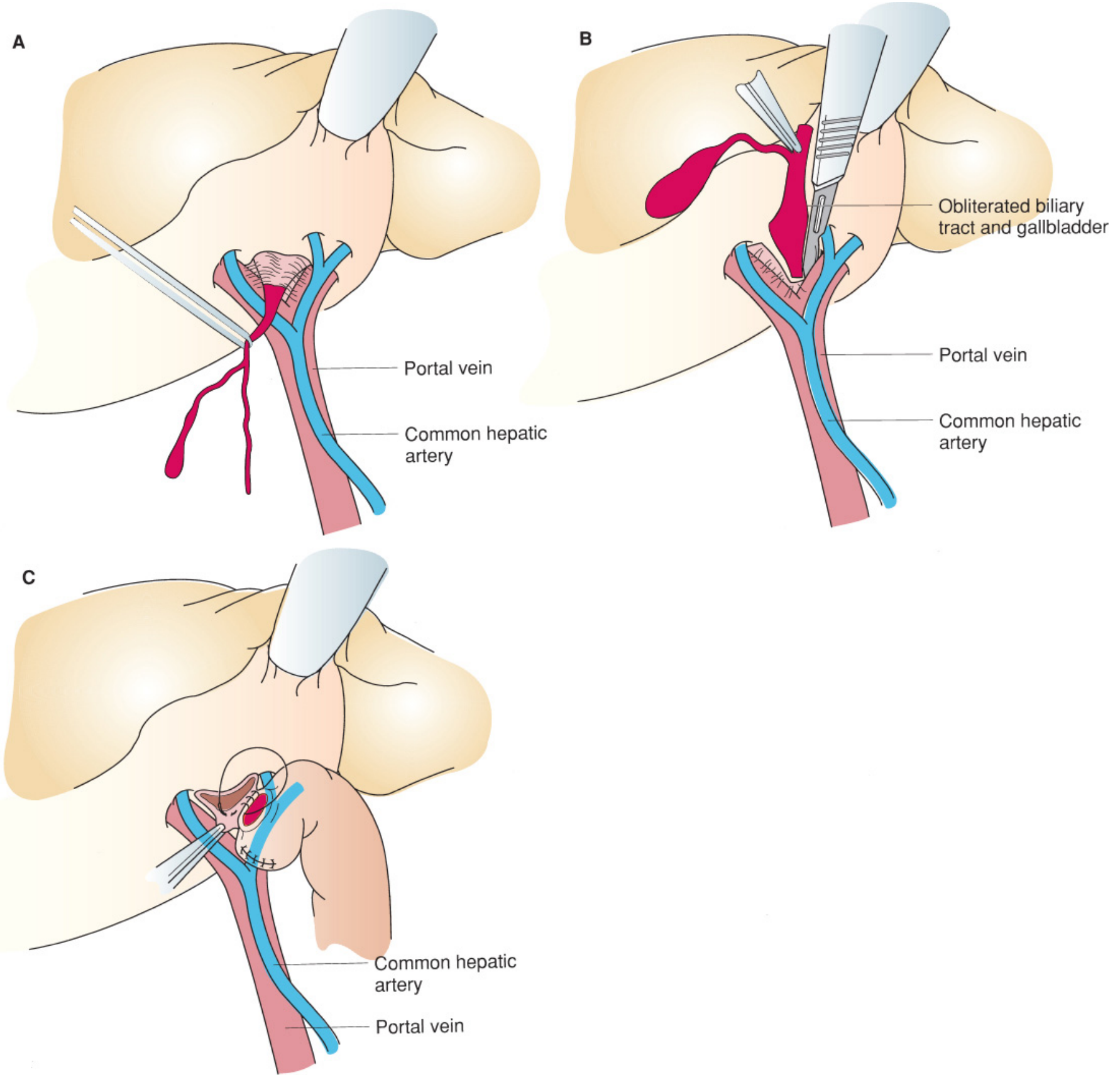
The Kasai procedure involves dissecting out the fibrous biliary remnant up to the porta hepatis, sharply transecting it at the level of the portal vein bifurcation, and then anastomosing the jejunal limb directly to the cut surface of the liver hilum. There is no true bile duct being sewn -- the anastomosis is to liver tissue at the porta.
From Mulholland and Greenfield's Surgery:
"A nonpatent, fibrous cord rather than a normal common bile duct is found in the hepatoduodenal ligament. This cord is dissected free proximally to the level of the porta hepatis between the portal vein bifurcation. The fibrous remnant is sharply transected at this level to preserve any patent bile ducts. A short, 15- to 25-cm retrocolic, jejunal Roux-Y limb is constructed."
Roux-en-Y Hepaticojejunostomy
| Feature | Detail |
|---|---|
| Full name | Roux-en-Y hepaticojejunostomy |
| Indications | Choledochal cysts (after resection), biliary strictures, bile duct injuries, pancreaticoduodenectomy (Whipple), liver transplantation biliary reconstruction, recurrent CBD stones |
| What is anastomosed | A patent hepatic duct (common hepatic duct or left/right hepatic duct) |
| To what | A Roux-en-Y limb of jejunum (typically 60 cm), side-to-side or end-to-side |
| Age group | Any age; adults most commonly |
| Goal | Bypass or reconstruct an obstructed/resected bile duct using a defunctionalized jejunal limb |
In this operation, a proper, patent bile duct is identified and sutured to the jejunum. The anastomosis is a true ductal anastomosis (single-layer absorbable suture), not to raw liver parenchyma.
Key Comparison Summary
| Kasai Portoenterostomy | Roux-en-Y Hepaticojejunostomy | |
|---|---|---|
| Indication | Biliary atresia | Bile duct obstruction/injury/resection |
| Anastomosis to | Porta hepatis (raw liver hilum) | Hepatic bile duct (patent duct) |
| Bile duct present? | No - obliterated | Yes - patent duct sutured |
| Patient age | Neonates/infants | Any age |
| Roux-en-Y limb used? | Yes | Yes |
| Outcome | ~66-75% achieve bile flow; most eventually need transplant | Generally durable biliary drainage |
The Shared Element
Both procedures use a Roux-en-Y configuration to divert enteric content and prevent bile reflux into the biliary tree. This is where the similarity ends. The Kasai procedure is a specific variant designed for the unique pathology of biliary atresia, where no duct exists to anastomose. A hepaticojejunostomy, by definition, requires a hepatic duct to sew to the jejunum.
In fact, after a failed Kasai procedure, patients who progress to liver transplantation will often have a hepaticojejunostomy constructed as part of the biliary reconstruction in the transplant - illustrating that they are sequential, not synonymous operations.
- Mulholland and Greenfield's Surgery, 7e, p. 5601
- Clinical Gastrointestinal Endoscopy, 3e, p. 190
What is pirta hepatizls
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
You likely meant porta hepatis - here is a full explanation:
Porta Hepatis ("Gateway of the Liver")
The term comes from Latin: porta = gate/door, hepatis = of the liver. It is the hilum of the liver - a transverse fissure on the visceral (inferior) surface where structures enter and leave the liver.
What passes through the porta hepatis?
The porta hepatis contains the portal triad (three key structures) in a consistent arrangement within the hepatoduodenal ligament:
| Structure | Position | Direction |
|---|---|---|
| Portal vein | Posterior | Enters liver (carries nutrient-rich blood from gut) |
| Hepatic artery proper | Left-lateral, anterior | Enters liver (oxygenated blood) |
| Bile ducts (hepatic ducts) | Right-lateral, anterior | Exits liver (carries bile out) |
| Lymphatics & nerve plexus | Also present | Enter/exit |
From Gray's Anatomy for Students:
"The porta hepatis serves as the point of entry into the liver for the hepatic arteries and the portal vein, and the exit point for the hepatic ducts."
From Fischer's Mastery of Surgery:
"The hepatoduodenal ligament encloses the portal triad, consisting of the bile duct, hepatic artery, and portal vein... The portal vein lies posteriorly, while the proper hepatic artery lies left lateral and the bile duct lies in the right lateral aspect of the hepatoduodenal ligament anterior to the portal vein."
Clinical Relevance
-
Pringle Manoeuvre: The hepatoduodenal ligament (containing the porta hepatis structures) can be clamped between the thumb and forefinger to temporarily stop blood flow into the liver during surgery - used to control haemorrhage during hepatic resection.
-
Kasai procedure: In biliary atresia, the fibrous biliary remnant is dissected all the way up to the porta hepatis and transected there to expose any residual microscopic bile ductules.
-
Hilar cholangiocarcinoma (Klatskin tumour): A tumour arising at the confluence of the right and left hepatic ducts, right at the porta hepatis - notoriously difficult to resect due to the proximity of portal vein and hepatic artery.
-
Liver transplantation: The portal triad structures at the porta hepatis (portal vein, hepatic artery, bile duct) are all anastomosed individually during implantation of the donor liver.
-
Trauma: Injuries to the porta hepatis carry a mortality rate of ~51% overall, rising to 80% with multiple structure injuries, due to the concentration of major vascular and biliary structures in a small space. - Current Surgical Therapy 14e
In the context of our earlier discussion, when we said the Kasai procedure anastomoses the jejunum to the porta hepatis, it means the jejunum is sewn directly onto the cut surface of the liver hilum at this anatomical gateway, to drain bile from whatever microscopic ductules remain there.
- Gray's Anatomy for Students, p. 392
- Fischer's Mastery of Surgery 8e, p. 4778-4779
- Current Surgical Therapy 14e, p. 491
Ercp
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Here is a comprehensive overview of ERCP:
ERCP - Endoscopic Retrograde Cholangiopancreatography
What is it?
ERCP is a combined endoscopic + fluoroscopic procedure used to visualize and intervene on the biliary and pancreatic ducts. It uses a side-viewing (duodenoscope) - unlike standard endoscopes that look forward - because the ampulla of Vater sits on the medial wall of the second part of the duodenum and is best seen from the side.
Today, ERCP is predominantly therapeutic, not diagnostic. For pure diagnostic imaging of the biliary tree, MRCP is preferred due to the risk of ERCP complications.
Equipment
- Side-viewing duodenoscope (with an elevator/bridge to direct accessories)
- Fluoroscopy (X-ray) machine
- Contrast dye
- Accessories: sphincterotome, guidewires, extraction balloons, baskets, stents
Technique (Step by Step)
- Patient placed prone (or supine if needed, e.g. during laparoscopic cholecystectomy); IV sedation or general anaesthesia
- Side-viewing scope passed blindly into oesophagus → stomach → duodenum
- Scope manoeuvred into "short-scope" position in the second part of the duodenum, where the ampulla of Vater (major papilla) is visible on the medial wall
- Glucagon may be given to reduce duodenal peristalsis
- Papilla is cannulated using a pull-wire sphincterotome or cannula over a guidewire
- Bile duct: enters at 11 o'clock, below the "lip" of the papilla
- Pancreatic duct: enters perpendicularly at 1 o'clock
- Contrast injected under fluoroscopy to visualise ducts
- Therapeutic intervention performed as needed
Indications
From Maingot's Abdominal Operations:
| # | Indication |
|---|---|
| 1 | Suspected choledocholithiasis (CBD stones) |
| 2 | Malignant or benign biliary/pancreatic strictures |
| 3 | Abnormal biliary imaging |
| 4 | Persistent jaundice / cholangitis |
| 5 | Sphincter of Oddi dysfunction (SOD) |
| 6 | Bile duct injury / leak / trauma |
| 7 | Ampullary adenoma treatment |
| 8 | Recurrent or idiopathic pancreatitis |
| 9 | Chronic pancreatitis (stones, strictures) |
| 10 | Pancreatic fluid collections / necrosis |
| 11 | Cytology of suspected pancreatic cancer |
Therapeutic Interventions Possible at ERCP
| Intervention | Use |
|---|---|
| Biliary sphincterotomy | Cut the sphincter to allow stone passage; most common intervention |
| Stone extraction (balloon/basket) | Remove CBD stones; go distal-to-proximal |
| Large balloon sphincteroplasty | For stones > 15 mm |
| Mechanical / laser lithotripsy | Fragment very large stones |
| Stent placement (plastic or metal) | Bypass strictures (malignant or benign) |
| Biliary dilation | Treat strictures |
| Nasobiliary drain | External biliary drainage |
| Needle knife / precut sphincterotomy | When standard cannulation fails (higher risk) |
Complications
Complication rate overall is < 10%. The four major specific complications are:
| Complication | Details |
|---|---|
| Post-ERCP Pancreatitis (PEP) | Most common complication (~5%); pancreatography and difficult cannulation are key risk factors |
| Bleeding | Especially post-sphincterotomy; pure-cut current may increase bleeding risk |
| Perforation | Duodenal or retroperitoneal; rare but serious |
| Cholangitis | Most important risk factor = incomplete drainage of an obstructed system; seen in hilar strictures (Bismuth III/IV), PSC, post-liver transplant |
Also:
- Post-ERCP cholecystitis (1.9-12%, especially with metal stents)
- Cardiopulmonary events from sedation
- Infection from inadequate scope reprocessing (MDR organisms like Klebsiella, E. coli, Pseudomonas from the elevator mechanism)
Contraindications / Special Situations
- Roux-en-Y anatomy (e.g. post-gastric bypass): standard ERCP difficult or impossible; requires enteroscopy-assisted ERCP or surgical/radiologic access
- Coagulopathy: avoid sphincterotomy if INR is high
- Active pancreatitis: ERCP only if biliary obstruction/cholangitis present
ERCP vs. MRCP
| ERCP | MRCP | |
|---|---|---|
| Type | Invasive (endoscopic) | Non-invasive (MRI) |
| Use | Therapeutic + diagnostic | Diagnostic only |
| Risk | Pancreatitis, bleeding, perforation | None |
| When to choose | When intervention planned | When only imaging needed |
Connection to Previous Discussion
ERCP cannot be performed after a Roux-en-Y hepaticojejunostomy or Kasai portoenterostomy via standard technique, because the ampulla is bypassed by the biliary-enteric anastomosis. Accessing the hepaticojejunostomy anastomosis requires deep enteroscopy (balloon-assisted), and the intrahepatic ducts may only be accessible percutaneously or via EUS-guided approaches.
- Maingot's Abdominal Operations, pp. 65-66
- Clinical Gastrointestinal Endoscopy 3e, pp. 806, 841
- Sleisenger & Fordtran's GI and Liver Disease
Eeco vs mrcp
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Assuming you meant EUS vs MRCP (a very common typo for "EUS"). Here is a detailed comparison:
EUS vs MRCP - Biliary Imaging Comparison
Both EUS and MRCP are used to image the biliary and pancreatic ductal systems - primarily as alternatives to diagnostic ERCP (which carries procedural risk). They are the two most important non/minimally-invasive tools for evaluating the biliopancreatic tree.
What They Are
| EUS (Endoscopic Ultrasound) | MRCP (Magnetic Resonance Cholangiopancreatography) | |
|---|---|---|
| Type | Semi-invasive endoscopic procedure | Completely non-invasive imaging (MRI-based) |
| How it works | Ultrasound transducer mounted on endoscope tip, placed in stomach/duodenum adjacent to biliary structures | T2-weighted MRI sequences - bile appears bright (high signal); stones appear as dark filling defects |
| Frequency used | 7.5-12 MHz (resolution < 1 mm) | No radiation, no contrast needed |
| Sedation needed? | Yes (IV sedation) | No |
Accuracy for CBD Stones (Choledocholithiasis)
| Parameter | EUS | MRCP |
|---|---|---|
| Sensitivity | 98% | 81-100% (state-of-art: 90-100%) |
| Specificity | 99% | 92-100% |
| PPV | 99% | 95% |
| NPV | 98% | 97-100% |
| Overall accuracy | 97% | ~97% (for large stones) |
From Maingot's Abdominal Operations:
"EUS findings were verified in 463 patients: 237 true positive, 216 true negative, 2 false positives, and 4 false negatives (sensitivity 98%, specificity 99%, PPV 99%, NPV 98%, accuracy 97%). No complications were noted."
For MRCP, stone size matters significantly:
- Stones 11-27 mm: sensitivity 100%
- Stones 6-10 mm: sensitivity 89%
- Stones 3-5 mm: sensitivity 71% (can miss small stones)
- Stones can be detected down to 2 mm with modern equipment
Key Differences
| Feature | EUS | MRCP |
|---|---|---|
| Small stones (< 5 mm) | Better - higher resolution | Can miss; sensitivity drops to ~71% for 3-5 mm |
| Ampullary stones | Better for ampullary region | Less reliable here |
| Intrahepatic duct stones | Limited (cannot visualize well) | Better - can image intrahepatic ducts |
| Microlithiasis / sludge | Better (intraductal detail) | May miss |
| Anatomy overview | Limited field of view | Better - whole biliary tree in one image |
| Stricture characterisation | Can biopsy (FNA) at same time | No tissue sampling |
| Complications | Very low (nearly none; large series show 0 complications) | None |
| Availability | Requires trained endoscopist | Widely available |
| Cost | Higher operator cost | Generally available at most centres |
| Contraindications | Uncooperative patient, coagulopathy | Pacemakers, metallic implants, claustrophobia, obesity |
| Can follow with therapy? | Yes - can do ERCP immediately after under same sedation | No - only diagnostic |
| Radiation | None | None |
Clinical Use: Which to Choose?
From Clinical GI Endoscopy:
"EUS has emerged as a preferred alternative to ERCP in patients at intermediate risk of bile duct stones... The majority of patients in the EUS arm did not have bile duct stones and did not require ERCP; those who did have ductal stones usually underwent ERCP immediately following EUS, under the same sedation."
| Clinical Scenario | Preferred Modality |
|---|---|
| Suspected CBD stone, intermediate risk | EUS (can proceed to ERCP in same session) |
| Suspected CBD stone, want to avoid any procedure | MRCP |
| Suspected small stone / microlithiasis | EUS |
| Suspected intrahepatic stones | MRCP |
| Staging pancreatic / biliary malignancy | EUS (+ FNA for tissue) |
| Pre-cholecystectomy workup to exclude CBD stones | Either (both very accurate) |
| Patient with pacemaker/metal implant | EUS (MRCP contraindicated) |
| Patient unfit for endoscopy | MRCP |
| Post-Roux-en-Y / altered anatomy | MRCP (EUS may still access; ERCP very difficult) |
The Optimal Pathway
The current standard approach when CBD stones are suspected:
Transabdominal USS (first)
↓
Intermediate risk?
↓
EUS or MRCP
↓
Stone confirmed? → ERCP (therapeutic)
Stone excluded? → Proceed to cholecystectomy only
Up to 70% of patients sent for ERCP based on clinical criteria alone do NOT actually have CBD stones. EUS/MRCP before ERCP prevents unnecessary invasive procedures in the majority of these patients.
Also in the Biliary Imaging Arsenal
-
CT (unenhanced helical): sensitivity 88%, specificity 97% for stones but poor for small stones (sensitivity only 22% for identifying stone vs. dilated duct)
-
Intraductal Ultrasound (IDUS): best of all for tiny stones - sensitivity 97% vs 81% for ERCP - but requires deep biliary cannulation during ERCP
-
PTC (Percutaneous Transhepatic Cholangiography): used when ERCP not accessible (e.g. post-hepaticojejunostomy)
-
Maingot's Abdominal Operations, p. 1034
-
Clinical Gastrointestinal Endoscopy 3e, pp. 4986-4988
-
Mulholland and Greenfield's Surgery 7e
Ercp vs mrcp
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Here is a comprehensive ERCP vs MRCP comparison:
ERCP vs MRCP
The single most important concept:
MRCP has largely replaced ERCP for diagnostic purposes. ERCP is now reserved primarily for therapy.
From Sleisenger & Fordtran's GI and Liver Disease:
"MRCP has largely replaced ERCP for diagnostic cholangiography as a result of improvements in image quality and the noninvasive nature of MRCP."
From Harrison's Principles of Internal Medicine 22e (2025):
"MRCP has mostly replaced ERCP for diagnostic assessment of the pancreatic duct."
Side-by-Side Comparison
| Feature | ERCP | MRCP |
|---|---|---|
| Full name | Endoscopic Retrograde Cholangiopancreatography | Magnetic Resonance Cholangiopancreatography |
| Type | Invasive endoscopic procedure | Non-invasive MRI-based imaging |
| Primary role | Therapeutic | Diagnostic |
| How it works | Side-viewing scope + fluoroscopy; contrast injected retrogradely via ampulla of Vater | Heavily T2-weighted MRI; bile/fluid = bright (high signal); stones/strictures = dark filling defects |
| Contrast needed? | Yes - iodinated contrast injected | No contrast required |
| Radiation? | Yes (fluoroscopy) | No |
| Sedation? | Yes (IV sedation or GA) | No |
| Invasiveness | Semi-invasive (scope into duodenum) | Completely non-invasive |
| Therapy possible? | Yes - sphincterotomy, stone removal, stenting, dilation, biopsy | No - imaging only |
| Tissue sampling? | Yes - brush cytology, biopsy, cholangioscopy | No |
| Complication rate | Up to 10% (pancreatitis, bleeding, perforation, cholangitis) | None |
| Intrahepatic ducts | Less accessible | Excellent - can image 4th-order intrahepatic ducts |
| Small stones (< 5 mm) | Can detect (gold standard) | May miss (sensitivity drops to ~71% for 3-5 mm stones) |
| PSC diagnosis | Historically gold standard; still used when MRCP equivocal | First-line now |
| Contraindications | Coagulopathy, post-Roux-en-Y anatomy, contrast allergy | Pacemakers, metallic implants, claustrophobia, severe obesity |
| Post-Roux-en-Y | Very difficult/impossible via standard scope | Works normally |
| Cost | Higher (procedure + personnel + theatre) | Moderate (MRI scanner time) |
How They Image the Ducts
MRCP - the physics:
"Very heavily T2-weighted images are used. Virtually all solid tissue has low signal (dark). Fluid within the biliary tree, gallbladder, and pancreatic duct retains signal intensity and therefore appears bright. Multiple projections similar to conventional cholangiography can be obtained." - Yamada's Textbook of Gastroenterology
- Entire biliary tree imaged in a single 20-second breath-hold
- Can visualise down to 4th-order intrahepatic bile ducts
- No instrumentation, no radiation, no dye injection
ERCP - direct cannulation:
- Ampulla cannulated at the duodenoscope tip
- Contrast injected under live fluoroscopy
- Bile duct (11 o'clock) and pancreatic duct (1 o'clock) selectively filled
Diagnostic Accuracy Compared
| Condition | ERCP | MRCP |
|---|---|---|
| CBD stones (overall) | ~100% (gold standard) | Sensitivity 90-100%, specificity 92-100% |
| Stones > 10 mm | ~100% | ~100% |
| Stones 3-5 mm | ~100% | ~71% |
| Biliary strictures | High | Sensitivity 85.7%, specificity 100% |
| PSC | Historically gold standard | Now first-line (meta-analysis: sufficiently sensitive/specific) |
| Pancreatic duct pathology | Good | Good (has largely replaced ERCP for this) |
When to Use Which
| Clinical Situation | Best Choice |
|---|---|
| Suspected CBD stone, want diagnosis first | MRCP |
| Suspected CBD stone, high probability - plan to treat | ERCP (diagnostic + therapeutic in one) |
| PSC work-up | MRCP first; ERCP if equivocal or therapy needed |
| Pancreatic cancer staging / biliary obstruction | MRCP for anatomy; ERCP for stenting/palliation |
| Cholangitis requiring urgent drainage | ERCP (immediate therapy) |
| Bile duct injury post-cholecystectomy | MRCP to map anatomy; ERCP for stenting |
| Chronic pancreatitis assessment | MRCP (non-invasive); ERCP if intervention needed |
| Contraindication to MRI (pacemaker) | ERCP or EUS |
| Post-Roux-en-Y or hepaticojejunostomy | MRCP (ERCP cannot reach ampulla) |
The Modern Decision Algorithm
Suspected biliary/pancreatic pathology
↓
Start with MRCP
(non-invasive, no risk)
↓
Positive / confirms pathology?
↓
Proceed to ERCP
(for therapeutic intervention)
↓
MRCP equivocal + high suspicion?
↓
Proceed to ERCP anyway
(more sensitive for small stones,
allows tissue sampling)
What ERCP Can Do That MRCP Cannot
- Sphincterotomy
- Stone extraction (balloon/basket)
- Biliary stent placement (plastic or SEMS)
- Stricture dilation
- Brush cytology / intraductal biopsy
- Cholangioscopy (Spyglass) - direct visualisation inside the duct
- Nasobiliary drain placement
- Immediate treatment of cholangitis
Summary in One Line
MRCP = look. ERCP = look AND fix.
Use MRCP whenever you only need a picture. Use ERCP when you need to do something inside the duct - or when MRCP has failed to give a definitive answer.
- Sleisenger & Fordtran's GI and Liver Disease, p. 1299
- Mulholland and Greenfield's Surgery 7e, p. 2788
- Yamada's Textbook of Gastroenterology 7e
- Harrison's Principles of Internal Medicine 22e (2025)
What is roux en y
Finding Sources
Finding Sources
Reading File
Reading File
Here is a complete explanation of the Roux-en-Y:
Roux-en-Y - What It Is
Roux-en-Y (pronounced "roo-en-why") is a surgical reconstruction technique that creates a Y-shaped configuration from the jejunum. It was developed by Swiss surgeon César Roux (1857-1934).
The Core Concept
The "Y" shape is created by:
- Dividing the jejunum about 10-15 cm distal to the ligament of Treitz
- This creates two limbs:
- Efferent (Roux) limb - the distal segment, brought up to connect to whatever structure needs drainage (stomach, bile duct, oesophagus, pancreas)
- Afferent (biliopancreatic) limb - the proximal segment (still attached to duodenum, carries bile + pancreatic juice)
- The afferent limb is then re-joined (jejunojejunostomy) to the efferent limb ~40-60 cm below the upper anastomosis
- This creates the "Y" shape
[Stomach / Bile duct / Oesophagus]
|
Upper anastomosis
|
EFFERENT LIMB (Roux limb)
~40-60 cm
|
Jejunojejunostomy ←── AFFERENT LIMB
| (carries bile +
Continues to pancreatic juice
distal bowel from duodenum)
Why It's Done - The Key Benefit
The critical purpose of the Roux-en-Y is to prevent bile and pancreatic juice from refluxing back into the connected structure (stomach, oesophagus, bile duct). By making the efferent limb at least 40 cm long, the biliopancreatic secretions drain into the bowel well below the upper anastomosis and cannot reflux back up.
From Clinical GI Endoscopy:
"The Roux-en-Y reconstruction prevents biliopancreatic fluids from refluxing into the stomach in patients who have undergone gastric resection... To be effective, the efferent limb has to measure at least 40 cm from the gastrojejunal anastomosis to the jejunojejunal anastomosis."
The Three Limbs of a Roux-en-Y
| Limb | Also called | Contents | Connected to |
|---|---|---|---|
| Efferent / Roux limb | Alimentary limb | Food (and eventually bile lower down) | Upper structure (stomach, bile duct, etc.) |
| Afferent / biliopancreatic limb | Biliary limb | Bile + pancreatic juice | Reconnected to efferent limb ~40-60 cm below |
| Common channel | Distal intestine | Food + bile + pancreatic juice mixed | Continues to ileum and colon |
Applications - Where Roux-en-Y is Used
The same Y-shaped bowel configuration is applied in many different situations:
| Procedure | Upper Anastomosis | Why Roux-en-Y Used |
|---|---|---|
| Roux-en-Y Gastrojejunostomy (after gastrectomy) | Gastric remnant → jejunum | Prevent bile reflux gastritis |
| Roux-en-Y Gastric Bypass (bariatric) | Small gastric pouch → jejunum | Weight loss + reduce reflux |
| Roux-en-Y Hepaticojejunostomy | Hepatic bile duct → jejunum | Biliary reconstruction after CBD injury/resection, choledochal cyst, Whipple |
| Kasai Portoenterostomy | Porta hepatis → jejunum | Biliary drainage in biliary atresia |
| Roux-en-Y Oesophagojejunostomy | Oesophagus → jejunum | After total gastrectomy |
| Roux-en-Y Pancreaticojejunostomy | Pancreatic duct → jejunum | Whipple procedure, chronic pancreatitis |
| Roux-en-Y Choledochojejunostomy | CBD → jejunum | Biliary bypass for malignant obstruction |
Why Not Just Use a Simple Loop?
A simple loop gastrojejunostomy (Billroth II) connects the stomach to a loop of bowel - but bile can still reflux back into the stomach through the short afferent limb. The Roux-en-Y eliminates this because the biliopancreatic limb joins at a point 40-60 cm downstream, making reflux mechanically impossible against intestinal peristalsis.
Potential Complication: Roux Stasis Syndrome
One downside of the Roux-en-Y is Roux stasis (or Roux limb syndrome) - the efferent limb can lose normal peristaltic coordination after being divided, leading to delayed gastric emptying and food stasis. This is more common with longer Roux limbs.
Why ERCP Becomes Difficult After Roux-en-Y
As discussed earlier - after a Roux-en-Y reconstruction, the ampulla of Vater is now far away, accessed only by travelling down the short afferent limb from the jejunojejunostomy. A standard duodenoscope cannot reach this far. Balloon-assisted enteroscopy-ERCP or percutaneous/EUS-guided approaches are required instead.
- Maingot's Abdominal Operations, p. 495
- Clinical Gastrointestinal Endoscopy 3e, p. 130
Any imaging illustration?
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here are three excellent textbook illustrations:
1. Roux-en-Y Gastric Bypass (Bariatric) - showing the Y anatomy clearly
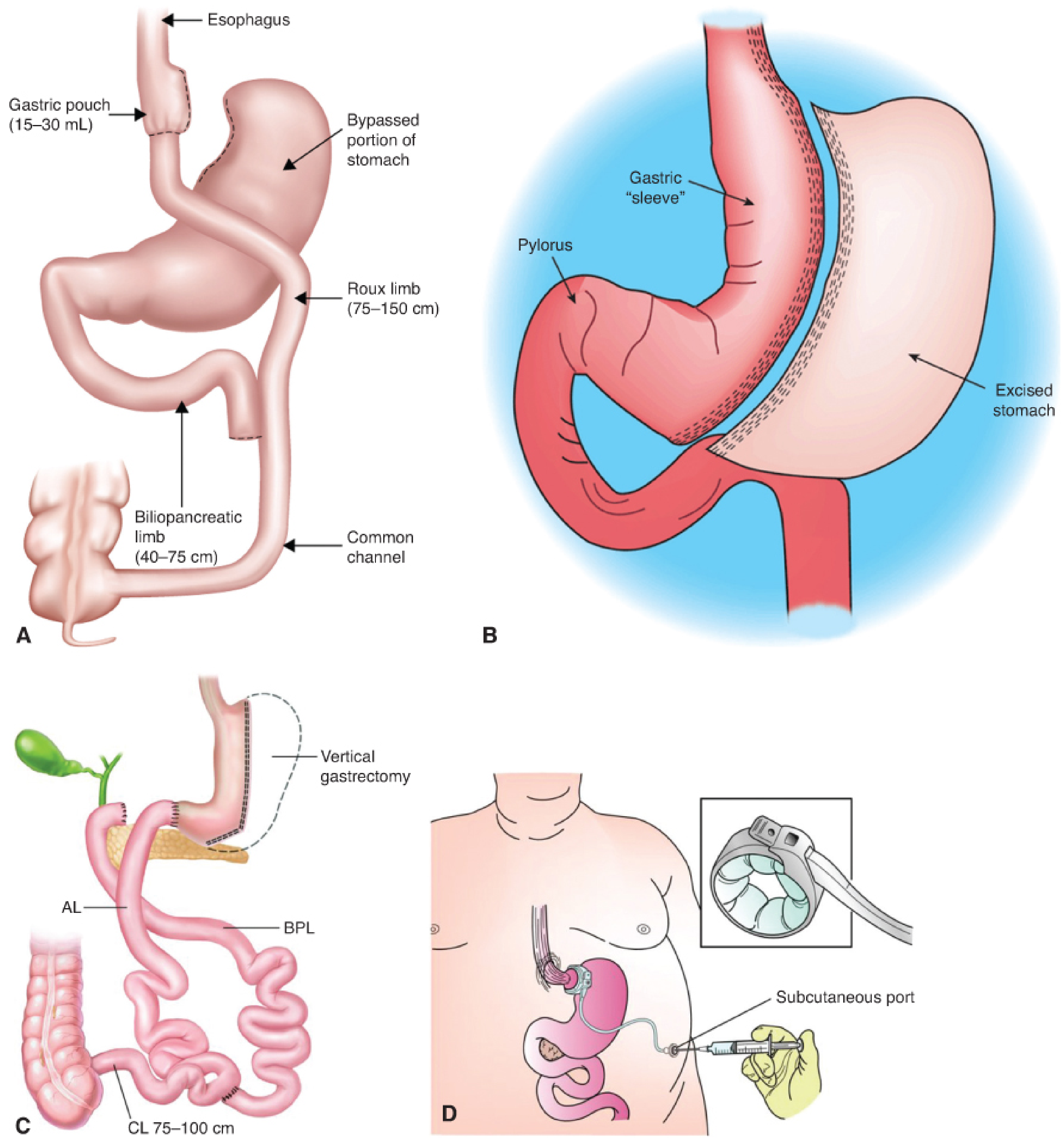
Panel A is the clearest illustration of the Roux-en-Y concept. You can see:
- Small gastric pouch (15-30 mL) at the top connected to the oesophagus
- The Roux (efferent/alimentary) limb (75-150 cm) - brings food down
- The biliopancreatic limb (40-75 cm) - carries bile and pancreatic juice
- The common channel where they join - food mixes with bile/enzymes here
- The bypassed (excluded) stomach and duodenum below
The Y-junction at the bottom is exactly what the name refers to.
2. Roux-en-Y Hepaticojejunostomy - step by step surgical illustration
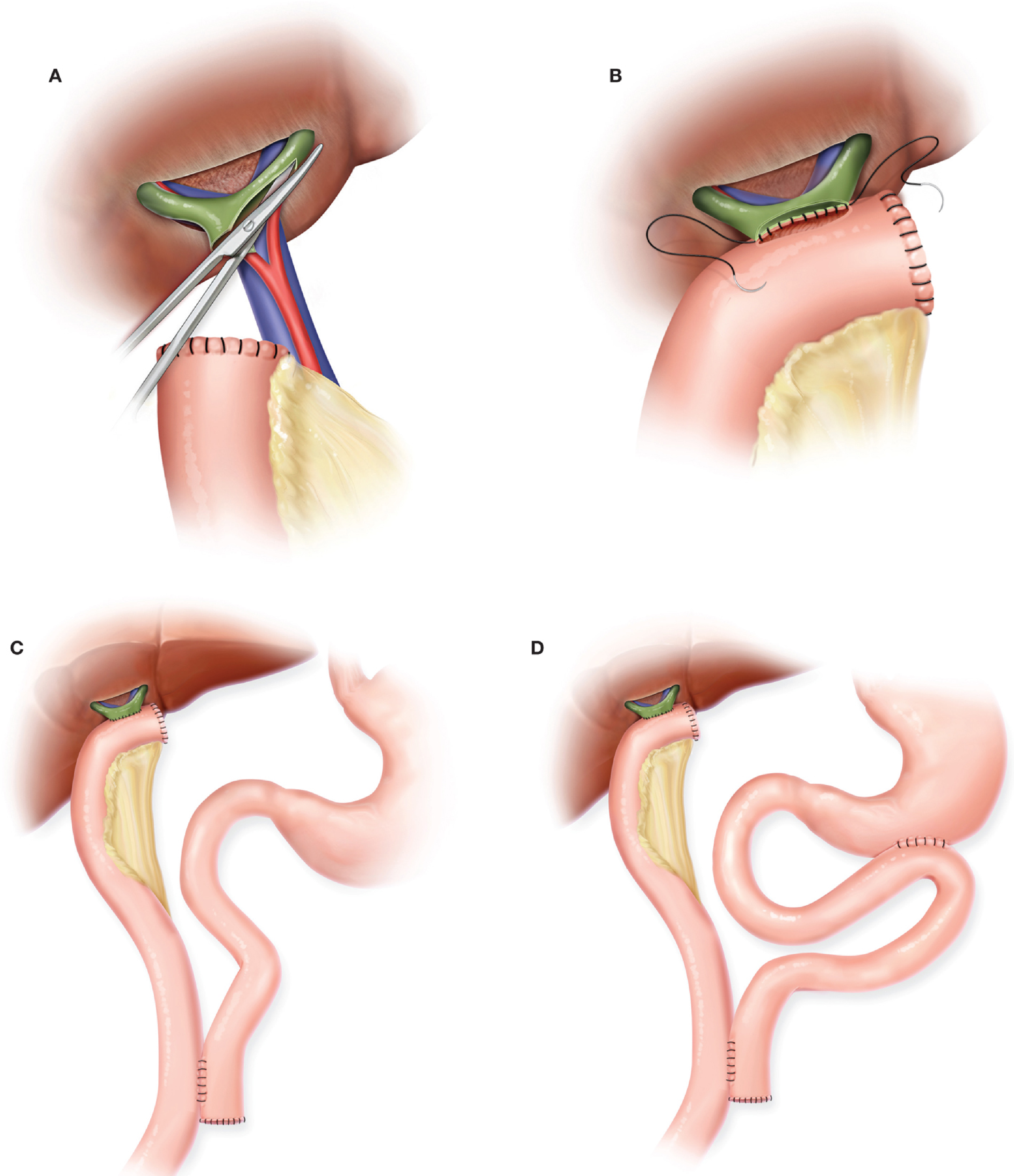
From Fischer's Mastery of Surgery. This shows:
- A: Dissection at the porta hepatis, identifying bile duct (green), portal vein (blue), hepatic artery (red)
- B: Running suture anastomosis being performed between bile duct and jejunum
- C: Final configuration of the Roux-en-Y hepaticojejunostomy - note the Y shape of the jejunum below
- D: Same with a loop gastrojejunostomy added alongside
3. Bilioenteric Anastomoses - Roux-en-Y Hepaticojejunostomy vs Choledochoduodenostomy
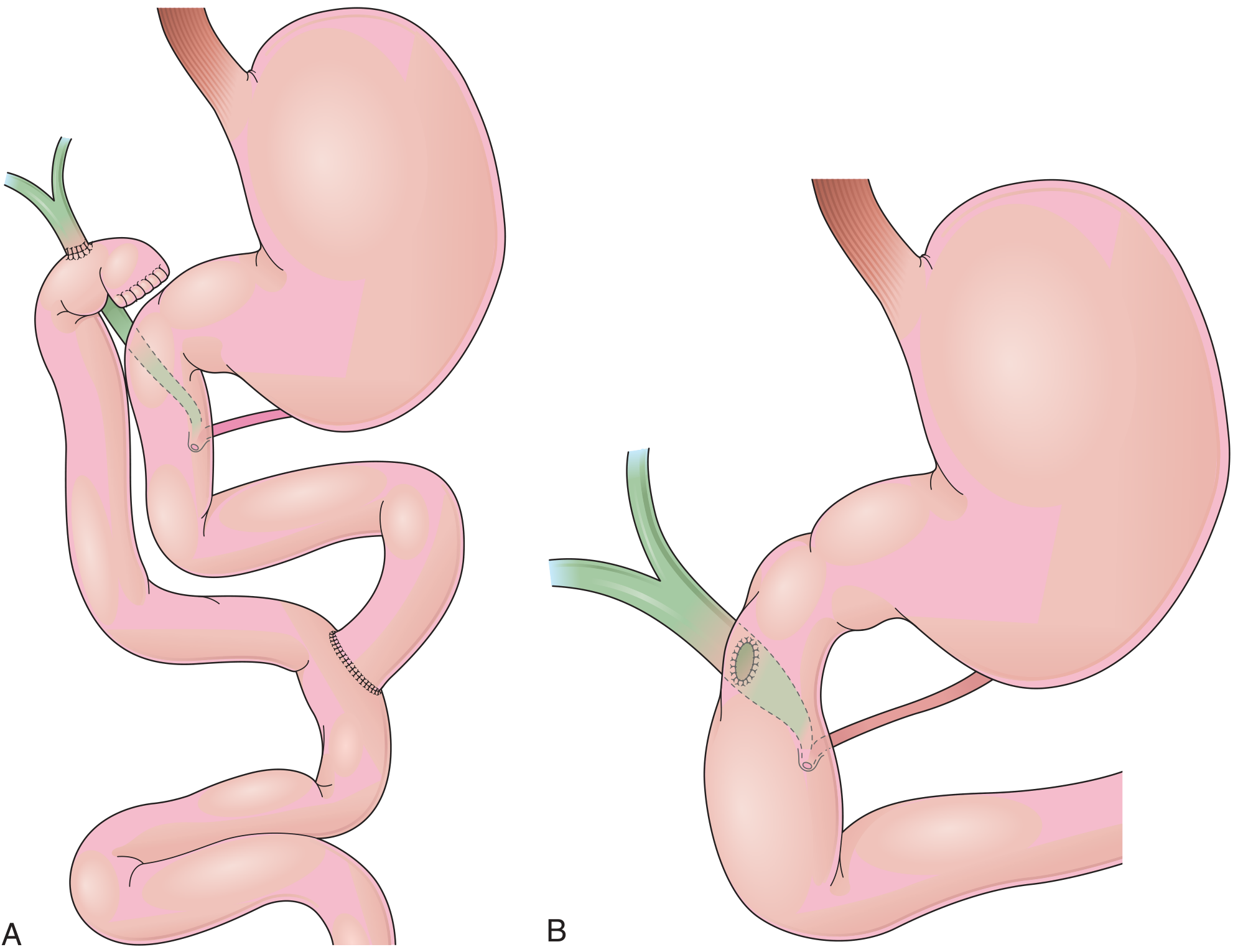
From Clinical GI Endoscopy. Panel A (left) shows the Roux-en-Y hepaticojejunostomy - the green bile duct anastomosed to the jejunal limb, with the stomach and duodenum completely untouched above. Panel B (right) shows a choledochoduodenostomy for comparison (bile duct anastomosed directly to duodenum instead).
These three images together give a complete picture of the Roux-en-Y configuration across its different applications - from bariatric surgery (gastric bypass) to biliary reconstruction (hepaticojejunostomy).
- Fischer's Mastery of Surgery 8e, Fig. 170.3
- Clinical GI Endoscopy 3e, Fig. 12.15
- Fischer's Mastery of Surgery 8e, Fig. 115.5
This is a shared conversation. Sign in to Orris to start your own chat.