Cardiovascular system in msn
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content to write a thorough MSN-level cardiovascular system overview. Let me compile this into the full answer.
The Cardiovascular System - MSN Level Overview
This covers the core cardiovascular content expected in a Master of Science in Nursing (MSN) program: anatomy, physiology, hemodynamics, cardiac cycle, coronary circulation, cellular mechanics, and heart failure.
1. Gross Anatomy of the Heart
The heart is a phasic, electrically self-actuated, variable-speed hydraulic pump composed of two dual-component muscular chambers - each with an atrium and a ventricle - that simultaneously deliver equal volumes of blood to the pulmonary and systemic circulations.
Structural skeleton: The annulus of the valves, the aortic and pulmonary arterial roots, the central fibrous body, and the left and right fibrous trigones form the heart's flexible cartilaginous skeleton. This skeleton serves three functions:
- Supports the avascular cardiac valves
- Resists forces of developed pressure and blood flow
- Provides a site of insertion for superficial subepicardial muscle
The myocardium is not discrete layers but a continuum of interconnecting muscle fibers arranged in outer layers (which pull the apex toward the base) and inner circumferential layers (which constrict the lumen, especially of the left ventricle).
Right vs. Left Ventricle:
- The LV is thick-walled and ellipsoidal, ejecting oxygenated blood into the high-pressure arterial system. It can generate pressure-volume work 5-7x greater than the RV.
- The RV is thin-walled and crescent-shaped, pumping deoxygenated blood into the low-pressure, compliant pulmonary arterial tree. It contracts in a more peristaltic, "bellows-like" manner, moving toward the septum and relying partly on LV contraction for support.
(Source: Miller's Anesthesia, 10e / Morgan & Mikhail's Clinical Anesthesiology, 6e)
2. Cardiac Valves
Two pairs of valves ensure unidirectional blood flow:
| Valve | Location | Structure |
|---|---|---|
| Aortic | LV outlet | Trileaflet (right, left, non-coronary cusps) |
| Pulmonic | RV outlet | Trileaflet (right, left, anterior cusps) |
| Mitral | LA-LV junction | Bileaflet (anterior & posterior) + chordae tendinae + papillary muscles |
| Tricuspid | RA-RV junction | Trileaflet (anterior, posterior, septal) |
Mitral valve: The anterior leaflet occupies a greater central diameter; the posterior leaflet extends further around the annular circumference. Chordae tendinae attached to papillary muscles prevent leaflet inversion. Papillary muscle ischemia or infarction can cause both mitral regurgitation and LV systolic dysfunction by disrupting this apparatus.
The sinuses of Valsalva in the aortic root prevent the leaflets from occluding the coronary ostia by creating hydraulic eddy currents during ejection.
3. Conduction System
The electrical activation sequence determines mechanical function:
| Structure | Function |
|---|---|
| SA node | Primary pacemaker; initiates each cardiac cycle |
| Internodal pathways (anterior, middle/Wenckebach, posterior/Thorel) | Transmit depolarization through RA to AV node |
| Bachmann's bundle | Transmits SA depolarization from RA to LA across atrial septum |
| AV node | Slow-conducting delay; ensures sequential atrial-then-ventricular contraction |
| Bundle of His | Penetrates the fibrous skeleton into the interventricular septum |
| Right & Left bundle branches | Distribute impulse to RV and LV respectively |
| Purkinje fibers | Rapid activation of ventricular myocardium |
The fibrous cardiac skeleton acts as an electrical insulator, preventing indiscriminate spread of atrial depolarization to the ventricles. The normal AV nodal delay creates the P-R interval on ECG and allows atrial systole to complete before ventricular systole begins ("atrial kick").
4. Determinants of Cardiac Performance
Cardiac output (CO) = Stroke Volume (SV) x Heart Rate (HR). Four factors govern performance:
Preload
The degree of myocardial stretch immediately before contraction - defined clinically as end-diastolic pressure or volume. Per the Frank-Starling law, increased preload increases end-diastolic volume and enhances stroke volume (up to a physiologic limit). Left ventricular end-diastolic pressures >20-25 mmHg cause fluid exudation into alveoli and pulmonary edema.
Factors affecting preload:
- Blood volume and its distribution
- Body position, intrathoracic pressure, intrapericardial pressure
- Venous tone, skeletal muscle pump action
- Atrial contraction (the "atrial kick" contributes ~25% of LV filling)
Afterload
The resistance the ventricle must overcome to eject blood. In the intact heart, afterload = the tension in the ventricular wall during ejection, governed by Laplace's Law:
Wall tension = (Intraventricular Pressure × Ventricular Radius) / Wall Thickness
Clinically, afterload is reflected by systemic vascular resistance (SVR):
SVR = (MAP - CVP) / CO
When afterload increases (e.g., vasoconstriction, hypertension), stroke volume decreases. When the ventricle dilates (heart failure), radius increases, afterload rises further - a vicious cycle that worsens pump function.
Factors affecting afterload:
- Systemic vascular resistance
- Arterial elasticity and blood volume
- Ventricular wall tension (radius, thickness)
Myocardial Contractility
The intrinsic ability to generate force independent of preload or afterload. Contractility is modulated by:
| Factor | Effect |
|---|---|
| Sympathetic stimulation / catecholamines | ↑ |
| Inotropic agents (digoxin, dobutamine) | ↑ |
| Intramyocardial Ca²⁺ | ↑ |
| Myocardial ischemia | ↓ |
| Cardiomyopathy / cell death | ↓ |
| Chronic neurohormonal overactivation | ↓ |
| Ventricular remodeling / fibrosis | ↓ |
Heart Rate
A powerful, direct determinant of CO. The Bowditch phenomenon (positive force-frequency relationship) describes how contractility increases at higher heart rates - a necessary compensatory mechanism during exercise. Excessive tachycardia, however, limits diastolic filling time and can reduce CO.
Frank-Starling Curves (Ventricular Function)
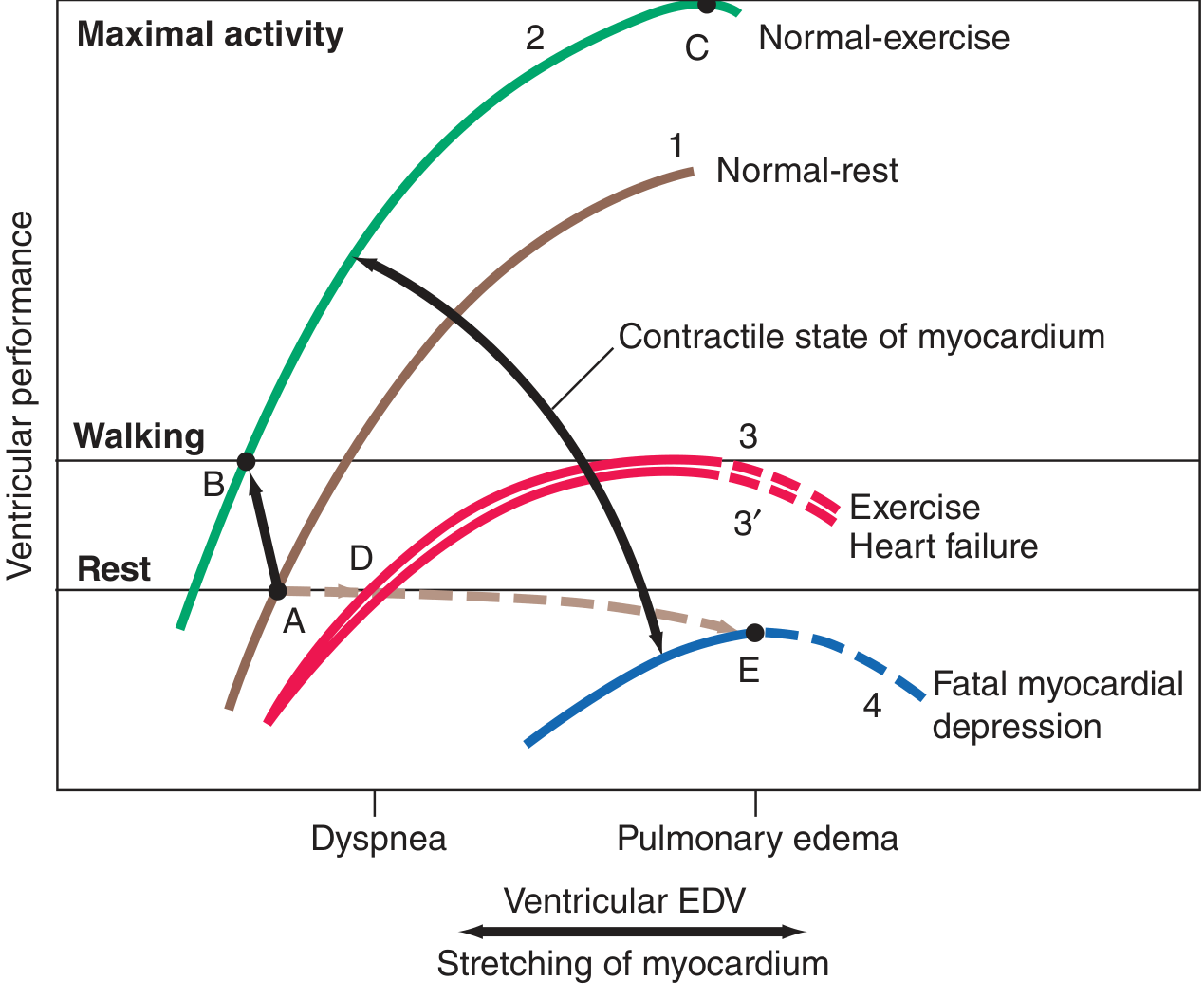
Figure: Ventricular performance vs. EDV curves. Curve 1 = normal at rest; Curve 2 = normal during exercise (increased contractility); Curve 3/3' = heart failure (reduced performance, dyspnea and pulmonary edema occur at lower preload). The failing heart operates on a depressed, flattened curve.
(Source: Harrison's Principles of Internal Medicine, 22e)
5. Cardiac Cycle
A coordinated series of electrical, mechanical, and valvular events:
| Phase | Events |
|---|---|
| Isovolumetric contraction | All valves closed; pressure builds; no volume change |
| Rapid ejection | Aortic/pulmonic valves open; SV ejected |
| Reduced ejection | Continued ejection at declining rate |
| Isovolumetric relaxation | All valves closed; pressure falls; no volume change |
| Rapid filling | Mitral/tricuspid valves open; passive ventricular filling (~75%) |
| Slow filling (diastasis) | Continued slow filling |
| Atrial systole | Active atrial contraction adds final ~25% of filling |
Normal pressures:
- LV systolic: ~120 mmHg | LV diastolic: ~8-12 mmHg
- Aorta systolic/diastolic: ~120/80 mmHg
- LA mean: ~8-12 mmHg
- RV systolic: ~25 mmHg | RV diastolic: ~0-8 mmHg
- PA systolic/diastolic: ~25/10 mmHg
6. Excitation-Contraction Coupling
The link between electrical depolarization and mechanical contraction is calcium:
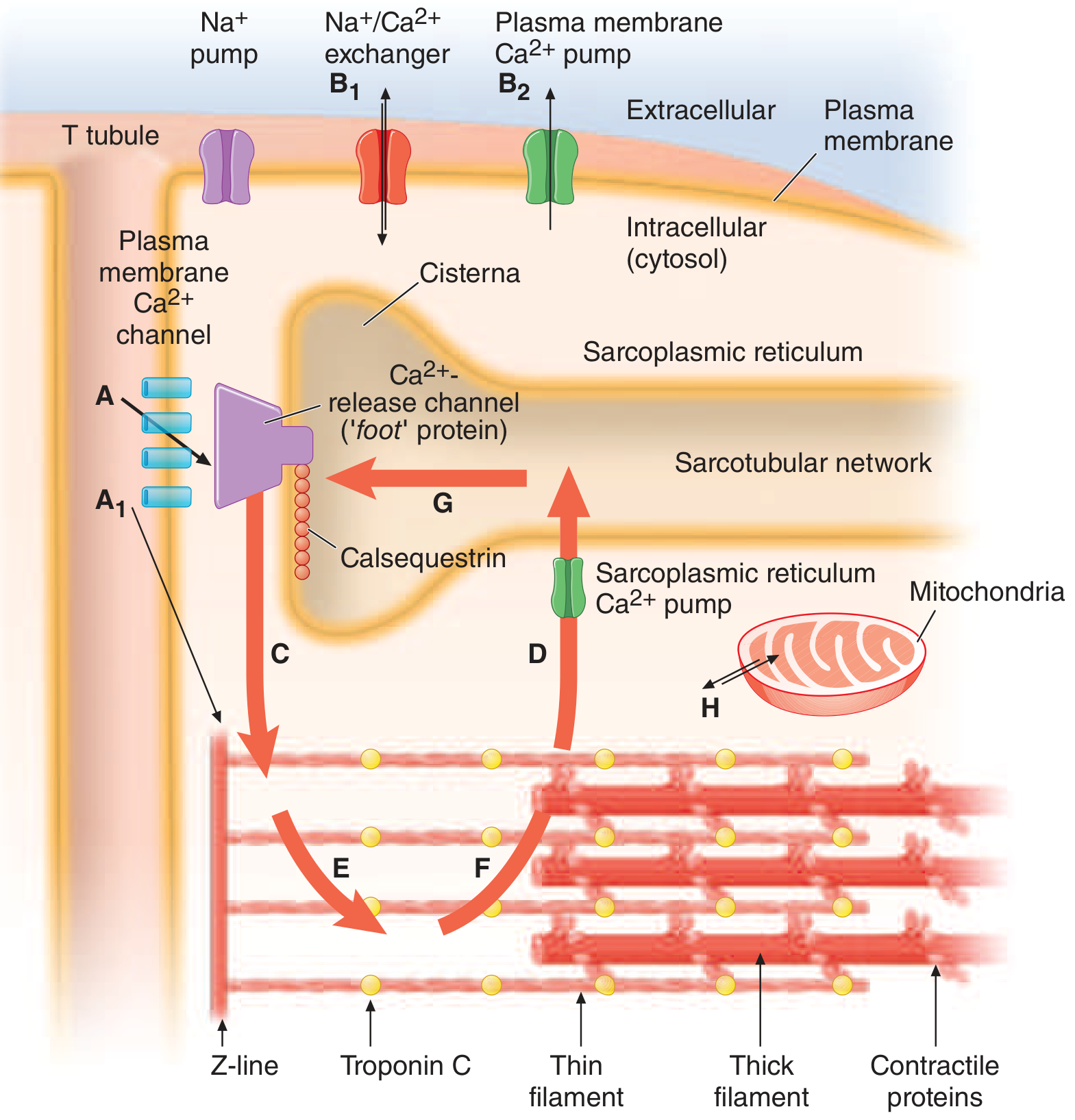
Figure: Cardiac excitation-contraction coupling. The larger intracellular Ca²⁺ cycle involves the sarcoplasmic reticulum (SR); the smaller extracellular cycle involves sarcolemmal channels.
Sequence:
- Action potential depolarizes the sarcolemma and T-tubules
- Voltage-gated L-type Ca²⁺ channels open → small Ca²⁺ influx from extracellular fluid (arrow A)
- This triggers calcium-induced calcium release (CICR) from the SR cisternae (arrow C) - the dominant Ca²⁺ source for contraction
- Ca²⁺ binds to troponin C → shifts tropomyosin → exposes actin binding sites → myosin-actin cross-bridge cycling → contraction
- Relaxation: SR Ca²⁺-ATPase (SERCA) pumps Ca²⁺ back into SR (arrow D); Na⁺/Ca²⁺ exchanger and plasma membrane Ca²⁺-ATPase remove Ca²⁺ from the cell (arrows B₁, B₂)
Clinical relevance: Cardiac glycosides (digoxin) inhibit Na⁺/K⁺-ATPase → ↑ intracellular Na⁺ → less Ca²⁺ removed by Na⁺/Ca²⁺ exchanger → ↑ intracellular Ca²⁺ → positive inotropy.
(Source: Harrison's Principles of Internal Medicine, 22e)
7. Coronary Circulation
Blood supply:
- Right coronary artery (RCA): SA node (~60%), AV node (~80%), RV, inferior LV wall
- Left anterior descending (LAD): Anterior LV, anterior septum, apex - "artery of the heart"
- Left circumflex (LCx): Lateral and posterior LV wall
Coronary physiology:
- Resting coronary blood flow ≈ 250 mL/min (1 mL/min/g; ~5% of CO)
- LV blood flow occurs almost entirely during diastole - because the contracting LV compresses intramural vessels during systole
- RV flow occurs both in systole and diastole (lower intramural pressures)
- Coronary perfusion pressure = Aortic diastolic pressure - LV end-diastolic pressure
- Autoregulation: Maintained between perfusion pressures of ~60-140 mmHg
- LV O₂ extraction is near-maximal at baseline (~75%) - so increased demand must be met by increased flow, not extraction
Autonomic regulation:
- Alpha₁: large coronary arteries (minimal resistance effect)
- Alpha₂: arterioles (vasoconstriction)
- Beta₁: arterioles (vasodilation)
- M₃ (muscarinic): normal endothelium → vasodilation via NO; diseased endothelium → vasoconstriction
8. Diastolic Function
Diastolic function = the ability of a cardiac chamber to collect blood at a normal filling pressure. It has two components:
- Relaxation (active): ATP-dependent re-uptake of Ca²⁺ by SR; requires adequate O₂ supply
- Compliance (passive): Ventricular wall stiffness; reduced in hypertrophy, fibrosis, ischemia
The pericardium exerts important restraining forces that limit chamber filling and contribute to ventricular interdependence - the phenomenon whereby filling of one ventricle affects the other.
9. Heart Failure
Heart failure (HF) occurs when the LV cannot eject blood at a sufficient rate to meet metabolic demands, or cannot fill completely without elevated filling pressure.
Classification by EF:
| Type | EF | Primary Mechanism |
|---|---|---|
| HFrEF (Heart Failure with reduced EF) | <40% | LV systolic dysfunction; reduced contractility |
| HFmrEF (mildly reduced EF) | 40-49% | Mixed |
| HFpEF (Heart Failure with preserved EF) | ≥50% | LV diastolic dysfunction; impaired relaxation/compliance |
Pathophysiology of HFpEF includes: diastolic dysfunction, ventricular and arterial stiffening, LA dysfunction, pulmonary hypertension, and RV dysfunction.
Compensatory mechanisms (and their limits):
| Mechanism | Short-term benefit | Long-term harm |
|---|---|---|
| Frank-Starling (↑ preload) | Maintains SV | Pulmonary congestion, edema |
| Sympathetic activation (↑HR, ↑contractility) | Maintains CO | Tachycardia, arrhythmia, myocyte death |
| Ventricular hypertrophy | ↓ wall stress (Laplace) | Diastolic dysfunction, ischemia |
| RAAS activation (Na⁺/H₂O retention) | ↑ preload | Volume overload, worsens congestion |
| Ventricular remodeling | Initial adaptation | Dilatation → ↑ afterload → further ↓ EF |
Nursing implications for HF management (MSN-level):
- Monitor daily weights (>2 lbs/day = fluid accumulation alert)
- Fluid restriction typically 1.5-2 L/day
- Low-sodium diet (<2 g/day)
- Monitor electrolytes with diuretic therapy (hypokalemia risk with loop/thiazide diuretics)
- Titrate ACE inhibitors/ARBs and beta-blockers per evidence-based guidelines
- Educate on medication adherence, signs of decompensation (orthopnea, PND, dyspnea on exertion, leg edema)
- LVEF-directed therapy: beta-blockers (metoprolol succinate, carvedilol, bisoprolol), ACEi/ARBi, MRAs, and SGLT2 inhibitors reduce mortality in HFrEF
10. Cardiovascular Responses to Physiologic Stress
During exercise:
- O₂ consumption can increase up to 18-fold
- ~1/3 met by improved O₂ extraction (venous saturation drops from 75% to ~25%)
- ~2/3 met by up to 6-fold increase in CO (via HR increase from 60-70 to 170-200 bpm and ↑ contractility)
- Arterial vasodilation reduces aortic impedance (↓ afterload)
- Venous return increases to maintain preload (Frank-Starling)
- Physiologic hypertrophy (athlete's heart) should be distinguished from pathologic hypertrophy (hypertension, MI)
Summary Reference Table
| Parameter | Formula / Normal Value |
|---|---|
| Cardiac output | SV × HR; normal 4-8 L/min |
| Cardiac index | CO / BSA; normal 2.4-4.0 L/min/m² |
| Stroke volume | CO / HR; normal 60-100 mL/beat |
| Ejection fraction | SV / EDV × 100; normal ≥55% |
| SVR | (MAP - CVP) / CO × 80; normal 800-1200 dyn·s/cm⁵ |
| PVR | (mPAP - PCWP) / CO × 80; normal <250 dyn·s/cm⁵ |
| MAP | DBP + 1/3(SBP - DBP); normal 70-100 mmHg |
| Coronary perfusion pressure | Aortic DBP - LVEDP; normal >50 mmHg |
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 6e - Chapter 12: Cardiac Anatomy and Physiology
- Harrison's Principles of Internal Medicine, 22e - Chapter 244: Normal and Abnormal Myocardial Function
- Goldman-Cecil Medicine, International Edition - Chapter: Work of the Heart
Renal system
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from the nephrology textbooks. Let me compile the full MSN-level renal system overview.
The Renal System - MSN Level Overview
1. Gross Anatomy of the Kidney
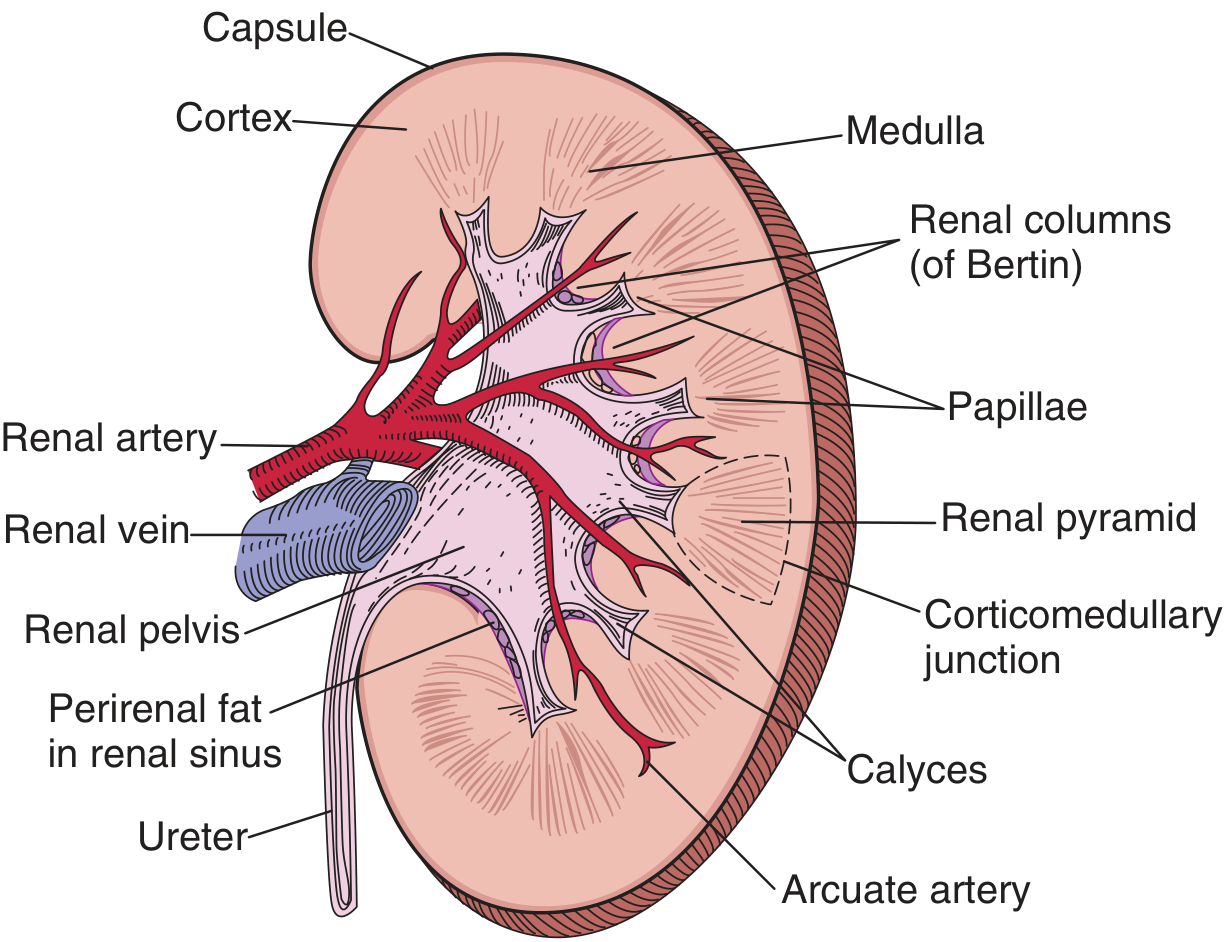
Fig. Anatomy of the bisected kidney showing key structural landmarks. (Brenner & Rector's The Kidney)
The kidneys are paired retroperitoneal organs, each approximately 11 cm long, 6 cm wide, and 150 g in weight. Each kidney contains:
| Structure | Description |
|---|---|
| Capsule | Fibrous outer covering |
| Cortex | Outer region; contains glomeruli, proximal/distal convoluted tubules |
| Medulla | Inner region; contains loops of Henle, collecting ducts; organized into renal pyramids |
| Renal columns (of Bertin) | Cortical tissue extending between pyramids |
| Papillae | Tips of pyramids; drain urine through area cribrosa into minor calyces |
| Renal pelvis | Funnel-like space collecting urine from major calyces |
| Ureter | Conducts urine from renal pelvis to bladder |
Renal blood supply:
- Renal artery → segmental arteries → interlobar arteries → arcuate arteries → interlobular arteries → afferent arterioles → glomerular capillaries → efferent arterioles → peritubular capillaries / vasa recta
- The kidneys receive ~20-25% of cardiac output (~1-1.2 L/min) despite being only ~0.5% of body weight
2. The Nephron - Functional Unit
The nephron is the functional unit of the kidney. Each human kidney contains approximately 900,000 to 1 million nephrons (range: 200,000 to 2.5 million per kidney). The number decreases substantially with age and is accelerated by hypertension.
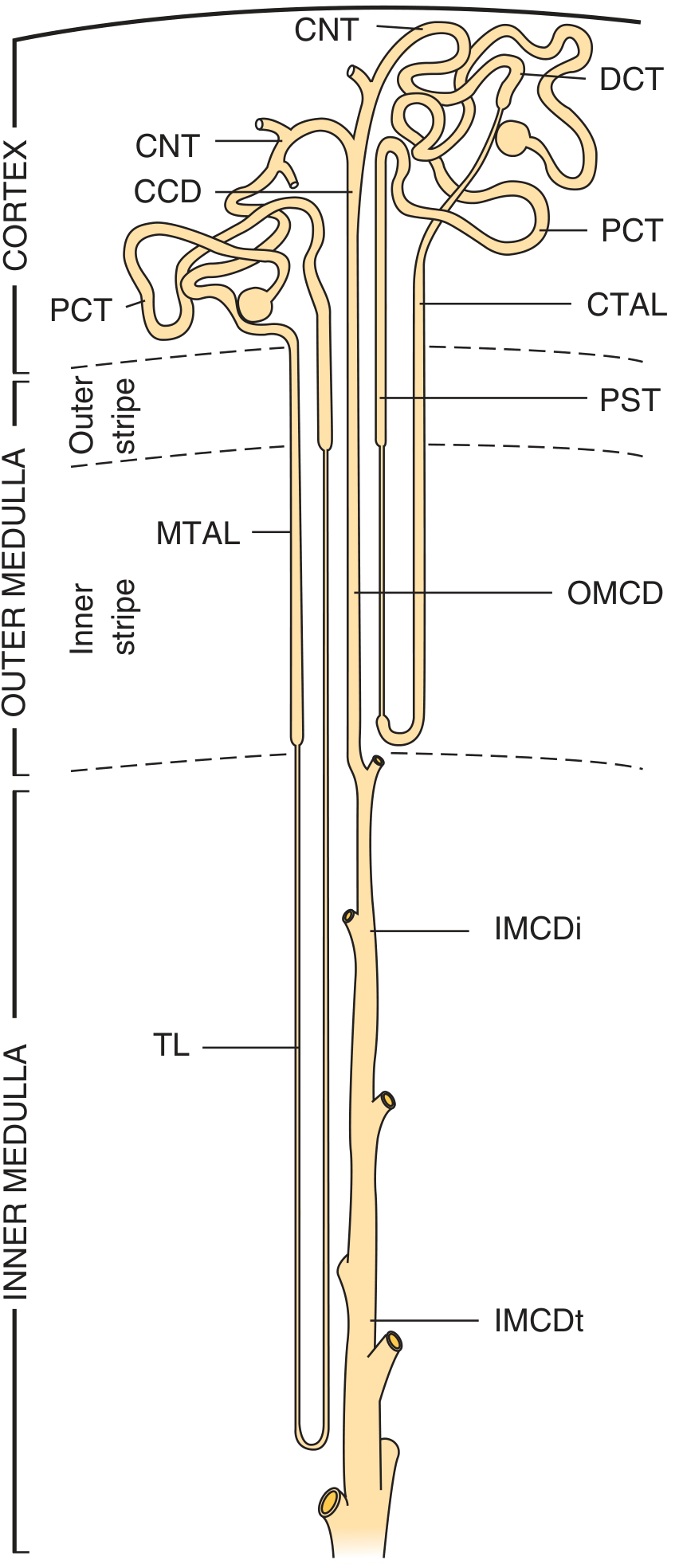
Fig. Superficial and juxtamedullary nephrons. PCT = proximal convoluted tubule; PST = proximal straight tubule; CTAL/MTAL = cortical/medullary thick ascending limb; DCT = distal convoluted tubule; CNT = connecting tubule; CCD/OMCD/IMCDi/IMCDt = collecting duct segments; TL = thin limb. (Brenner & Rector's The Kidney)
Nephron components:
- Renal corpuscle = glomerulus + Bowman's capsule
- Proximal convoluted tubule (PCT)
- Proximal straight tubule (PST / pars recta)
- Thin descending limb of Henle
- Thin ascending limb of Henle
- Thick ascending limb (TAL)
- Distal convoluted tubule (DCT)
- Connecting tubule (CNT)
The collecting duct (cortical CCD → outer medullary OMCD → inner medullary IMCDi/IMCDt) is technically a separate system (different embryologic origin - the ureteric bud) but functionally integrated.
Types of nephrons:
- Superficial/cortical nephrons (~85%): Short loops of Henle that bend within the outer medulla; involved primarily in urine dilution
- Juxtamedullary nephrons (~15%): Long loops extending deep into the inner medulla; critical for urine concentration
3. Renal Corpuscle and Glomerular Filtration
Each nephron begins in a renal corpuscle (~200 μm diameter), containing:
- Glomerular capillary tuft: Fenestrated endothelium
- Glomerular (Bowman's) capsule: Double-walled epithelial cup
- Visceral layer = podocytes (foot processes with filtration slits)
- Parietal layer = outer wall
- Capsular (urinary) space: Receives the ultrafiltrate
- Vascular pole: Afferent arteriole enters; efferent arteriole exits
- Tubular pole: PCT begins
Glomerular filtration barrier (3 layers):
- Fenestrated capillary endothelium (restricts cells)
- Glomerular basement membrane (GBM) - negatively charged (restricts anionic proteins)
- Podocyte foot processes with filtration slit diaphragms (restricts large proteins)
Starling Forces Governing Filtration
GFR = Kf × [(Pgc - Pbs) - (πgc - πbs)]
| Force | Value (approx.) | Effect |
|---|---|---|
| Glomerular capillary hydrostatic pressure (Pgc) | ~55 mmHg | Favors filtration |
| Bowman's space hydrostatic pressure (Pbs) | ~15 mmHg | Opposes filtration |
| Glomerular oncotic pressure (πgc) | ~30 mmHg | Opposes filtration |
| Bowman's space oncotic pressure (πbs) | ~0 mmHg | Favors filtration |
| Net filtration pressure | ~10 mmHg |
Normal GFR: ~120-125 mL/min (180 L/day filtered); only ~1.5-2 L excreted as urine
Autoregulation of GFR (between mean arterial pressure 80-180 mmHg):
- Myogenic reflex: Afferent arteriole constricts with increased pressure
- Tubuloglomerular feedback (TGF): Macula densa cells in TAL detect increased NaCl delivery → release adenosine → constricts afferent arteriole → ↓ GFR
4. Tubular Segments: Structure, Function, and Transport
Proximal Convoluted Tubule (PCT) - "The Workhorse"
Reabsorbs >60% of the filtered load. Features a prominent luminal brush border of microvilli to maximize surface area. Cells are highly metabolically active (rich in mitochondria).
What is reabsorbed in the PCT:
- ~67% of filtered Na⁺ (via NHE3 - Na⁺/H⁺ exchanger)
- ~100% of filtered glucose (via SGLT1/2 - sodium-glucose cotransporters)
- ~100% of filtered amino acids
- ~85% of filtered bicarbonate (via NHE3 + carbonic anhydrase)
- ~65% of filtered water (isosmotic, via Aquaporin-1)
- Phosphate (regulated by PTH - PTH inhibits Na⁺/phosphate cotransporter → phosphaturia)
- Uric acid, urea, potassium
Clinical relevance:
- SGLT2 inhibitors (empagliflozin, dapagliflozin) block glucose reabsorption → glycosuria → reduce blood glucose, body weight, BP, and have cardiorenal protective effects
- Carbonic anhydrase inhibitors (acetazolamide) block bicarbonate reclamation → metabolic acidosis + mild diuresis
Loop of Henle - "The Concentrating Segment"
The key segment for creating the medullary concentration gradient - the only compartment in the body with higher osmolality than serum.
Thin descending limb:
- Highly permeable to water (Aquaporin-1)
- Water exits passively into the hypertonic medullary interstitium → tubular fluid becomes concentrated
- Poorly permeable to solutes
Thin ascending limb:
- Impermeable to water
- Passively permeable to NaCl
Thick ascending limb (TAL) - "The Diluting Segment":
- Impermeable to water
- Active transport via NKCC2 (Na⁺/K⁺/2Cl⁻ cotransporter) → removes solute without water → dilutes tubular fluid and concentrates interstitium
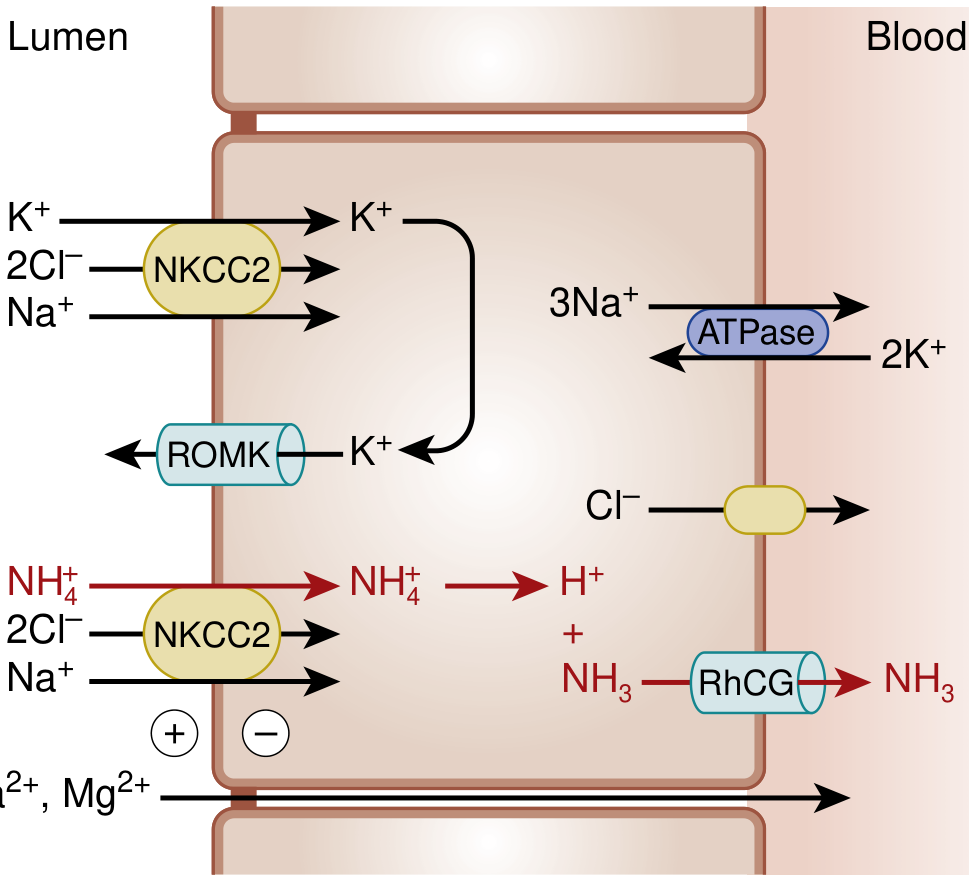
Fig. Transport in the thick ascending limb. NKCC2 is the target of loop diuretics. ROMK recycles K⁺ into the lumen, generating a lumen-positive charge that drives paracellular reabsorption of Ca²⁺ and Mg²⁺. (NKF Primer on Kidney Diseases, 8e)
Genetic conditions affecting the TAL:
- Bartter syndrome: Loss-of-function mutations in NKCC2, ROMK, or chloride channels → renal salt wasting, hypokalemia, metabolic alkalosis (similar to chronic loop diuretic use)
Loop diuretics (furosemide, bumetanide, torsemide) inhibit NKCC2 → block up to 25% of sodium reabsorption → most potent diuretics.
Distal Convoluted Tubule (DCT) - "The Diluting Segment"
- Very short segment (10-12 mm)
- Impermeable to water
- Contains NCC (Na⁺/Cl⁻ cotransporter) - reabsorbs ~5% of filtered Na⁺
- Contains TRPV5 Ca²⁺ channel on luminal membrane (activated by calcitriol and PTH → Ca²⁺ reabsorption)
Thiazide diuretics (hydrochlorothiazide, chlorthalidone) inhibit NCC → moderate natriuresis + increased Ca²⁺ reabsorption (used in hypercalciuria/kidney stone prevention).
Genetic conditions:
- Gitelman syndrome: Loss-of-function in NCC → hypokalemia, hypomagnesemia, metabolic alkalosis, hypocalciuria (mirror of chronic thiazide use)
Collecting Duct - "Final Regulator of Urine Composition"
The collecting duct contains two cell types that act in concert:
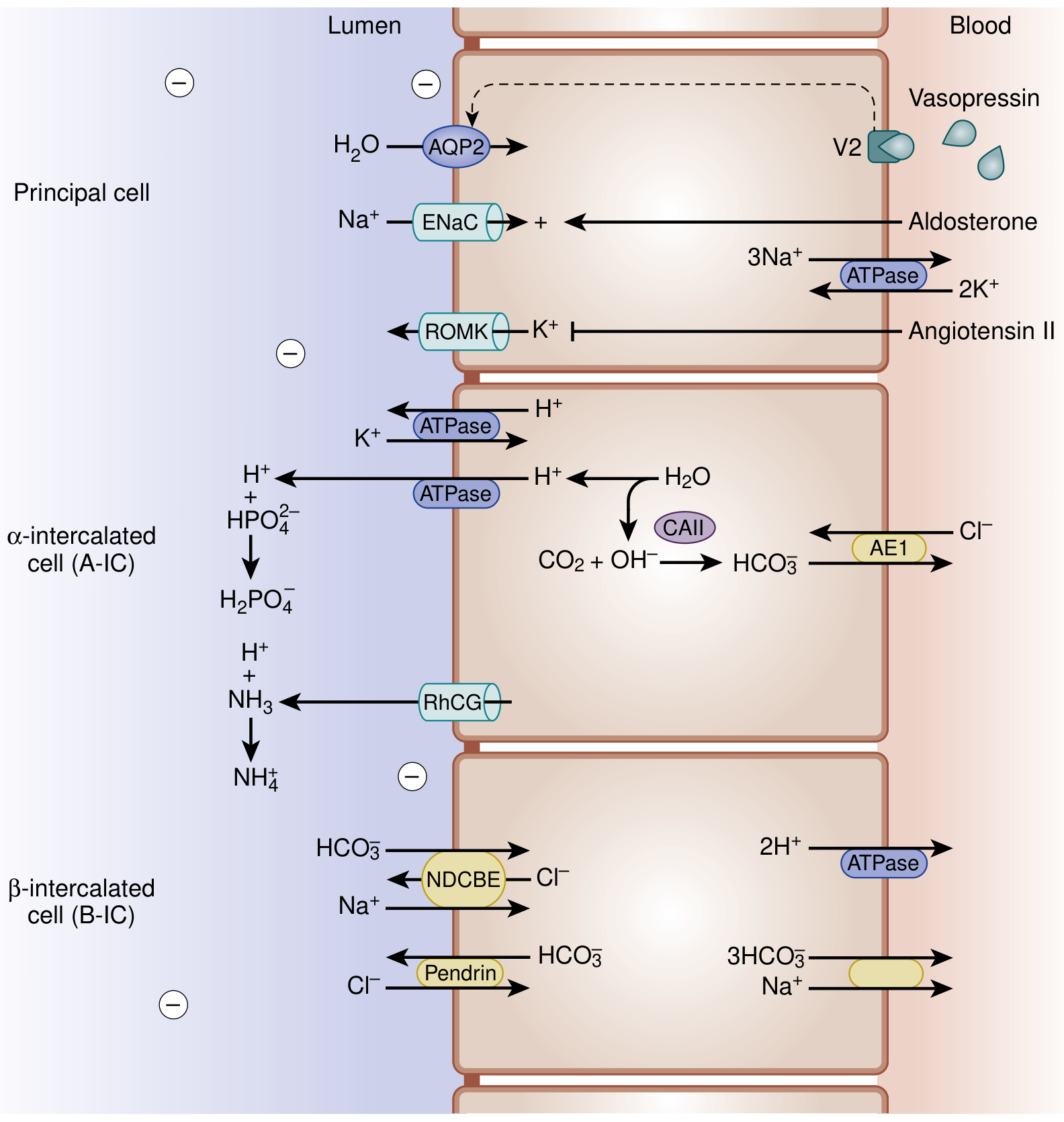
Fig. Collecting duct transport. Principal cells respond to vasopressin (AQP2) and aldosterone (ENaC). α-intercalated cells secrete H⁺. β-intercalated cells secrete HCO₃⁻. (NKF Primer on Kidney Diseases, 8e)
Principal cells:
- Vasopressin (ADH) binds V2 receptor → cAMP → Aquaporin-2 (AQP2) translocates to luminal membrane → water reabsorption → concentrated urine
- Aldosterone → ↑ ENaC (epithelial Na⁺ channel) expression → Na⁺ reabsorption → lumen becomes electronegative → K⁺ secretion via ROMK
- Angiotensin II inhibits ROMK (reduces K⁺ secretion while maintaining Na⁺ reabsorption)
α-intercalated cells (A-IC):
- Luminal H⁺-ATPase secretes H⁺ into urine
- Intracellular carbonic anhydrase II (CAII): CO₂ + H₂O → H⁺ + HCO₃⁻
- HCO₃⁻ exits basolaterally via AE1 (anion exchanger 1) → "new bicarbonate" added to blood
- H⁺ excreted with titratable acids (phosphate) or ammonia → net acid excretion
β-intercalated cells (B-IC):
- Secrete HCO₃⁻ into lumen (via pendrin) while reabsorbing Cl⁻
- Active in metabolic alkalosis to excrete excess bicarbonate
Genetic conditions:
- Liddle syndrome: Gain-of-function ENaC mutation → hypertension, hypokalemia, suppressed renin/aldosterone (treat with amiloride/triamterene, NOT spironolactone)
- Pseudohypoaldosteronism type 1: Loss-of-function ENaC → salt wasting despite high aldosterone
Potassium-sparing diuretics:
- Amiloride/triamterene: Direct ENaC blockers
- Spironolactone/eplerenone: Mineralocorticoid receptor (aldosterone) antagonists → ↓ ENaC → ↓ K⁺ secretion
5. Tubular Sodium Reabsorption - Summary
Under normal conditions, of the ~25,200 mEq/day of filtered sodium:
| Segment | % Reabsorbed | Transporter | Diuretic Target |
|---|---|---|---|
| Proximal tubule | ~67% | NHE3 | Carbonic anhydrase inhibitors (weak) |
| Loop of Henle (TAL) | ~25% | NKCC2 | Loop diuretics (furosemide) |
| Distal convoluted tubule | ~5% | NCC | Thiazide diuretics |
| Collecting duct | ~3% | ENaC | Potassium-sparing diuretics |
| Excreted | <1% |
Fractional Excretion of Sodium (FENa):
FENa = (UNa × PCr) / (PNa × UCr) × 100%
| FENa | Interpretation |
|---|---|
| <1% | Pre-renal AKI (kidney conserving Na⁺; tubules intact) |
| >2% | Intrinsic renal AKI (tubular damage, cannot conserve Na⁺) |
| >3% | Post-renal or established ATN |
Note: FENa is unreliable in patients on diuretics - use FEUrea instead
6. Urine Concentration and the Countercurrent Mechanism
The kidney can produce urine ranging from 50 mOsm/L (maximum dilution) to 1200 mOsm/L (maximum concentration), vs. plasma at ~290 mOsm/L.
Creating the medullary gradient:
- TAL actively transports NaCl (not water) into the medullary interstitium → builds hyperosmotic interstitium
- Thin descending limb (water-permeable) loses water to the hypertonic interstitium → tubular fluid concentrates to ~800-1200 mOsm/L at the hairpin turn
- Vasa recta (countercurrent exchange): Blood flowing down loses water and gains solute; blood flowing up gains water and loses solute → prevents washout of the medullary gradient
- Urea: Vasopressin activates urea transporters in the inner medullary collecting duct → urea enters interstitium → contributes ~400-500 mOsm/L of medullary osmolality
Tubular fluid osmolality along the nephron:
| Segment | Osmolality (mOsm/L) |
|---|---|
| Glomerular filtrate | ~290 (isosmotic) |
| End of proximal tubule | ~290 (isosmotic reabsorption) |
| Hairpin turn (descending limb) | ~800-1200 |
| Macula densa (end of TAL) | ~290 (diluted by NaCl removal) |
| End of DCT | ~50-100 (maximum dilution) |
| Final urine (with ADH) | Up to 1200 |
| Final urine (without ADH) | 50-100 (dilute) |
7. Volume and Sodium Homeostasis
The Effective Arterial Blood Volume (EABV) is the key regulated variable - the portion of circulation sensed by baroreceptors that controls renal sodium handling. The ECF volume and total body sodium are primarily regulated by the kidney.
Sensors of EABV:
- Low-pressure: Right atrium, central veins, pulmonary vessels
- High-pressure: Afferent arteriole (juxtaglomerular apparatus), carotid sinus, aortic arch, LV
Regulators of sodium excretion:
| Regulator | Stimulus | Renal Effect |
|---|---|---|
| RAAS | ↓ EABV, ↓ NaCl at macula densa, ↑ SNS | ↑ Na⁺ reabsorption |
| Sympathetic NS | ↓ EABV | ↑ Na⁺ reabsorption; ↑ renin |
| Vasopressin (ADH) | ↑ plasma osmolality, ↓ EABV | ↑ water reabsorption (AQP2) |
| Atrial natriuretic peptide (ANP) | ↑ atrial stretch (volume overload) | ↑ Na⁺ excretion (natriuresis); ↓ renin |
The Renin-Angiotensin-Aldosterone System (RAAS)
Three stimuli for renin release (from juxtaglomerular cells of afferent arteriole):
- Decreased pressure at the afferent arteriole baroreceptor
- Macula densa signals decreased NaCl delivery (via NKCC2)
- Increased sympathetic outflow (β₁-adrenergic stimulation)
Cascade:
Angiotensinogen (liver) → Renin → Angiotensin I → ACE (lung/kidney) → Angiotensin II → Aldosterone (adrenal cortex)
Actions of Angiotensin II:
- Constricts efferent arteriole (maintains GFR when renal perfusion is reduced)
- Direct Na⁺ reabsorption in proximal tubule
- Stimulates aldosterone release
- Vasoconstriction (↑ SVR)
- ADH release
- Thirst/water intake
Actions of Aldosterone:
- Binds mineralocorticoid receptor in collecting duct principal cells
- ↑ ENaC expression → Na⁺ reabsorption
- ↑ ROMK → K⁺ secretion (explains the hypokalemia with hyperaldosteronism)
- ↑ H⁺-ATPase in α-IC cells → H⁺ secretion (explains metabolic alkalosis)
RAAS in Heart Failure and Cirrhosis:
EABV is decreased despite increased total body Na⁺ and ECF volume → RAAS activated → maladaptive Na⁺ and water retention → edema, ascites. This is why ACE inhibitors, ARBs, and spironolactone are cornerstones of HF management.
8. Potassium Regulation
The kidney is the primary regulator of K⁺ balance (~90% excreted by kidneys). Normal plasma K⁺: 3.5-5.0 mEq/L.
Determinants of urinary K⁺ excretion (at the collecting duct):
- Aldosterone → ↑ ENaC → ↑ lumen-negative potential → ↑ K⁺ secretion via ROMK
- Tubular flow rate: Higher flow → ↑ K⁺ secretion (dilutes luminal K⁺, maintaining gradient)
- Plasma K⁺: Hyperkalemia directly stimulates K⁺ secretion and aldosterone
- Acid-base status: Acidosis → K⁺ shifts out of cells → hyperkalemia + H⁺/K⁺ exchange in collecting duct reduces K⁺ secretion; alkalosis promotes K⁺ secretion
Internal K⁺ distribution (ECF vs. ICF):
- 98% of total body K⁺ is intracellular (mainly muscle)
- Insulin → K⁺ into cells (used emergently in hyperkalemia)
- Catecholamines (β₂) → K⁺ into cells
- Acidosis → K⁺ out of cells (for every 0.1 unit ↓ pH, plasma K⁺ rises ~0.5-0.6 mEq/L)
9. Acid-Base Regulation by the Kidney
The kidney regulates acid-base balance through three mechanisms:
1. Bicarbonate Reabsorption (Proximal Tubule - ~85%)
- H⁺ secreted via NHE3 into lumen + HCO₃⁻ in lumen → H₂CO₃ → CO₂ + H₂O (carbonic anhydrase on brush border)
- CO₂ diffuses into cell → regenerated as H⁺ + HCO₃⁻ inside (carbonic anhydrase II)
- HCO₃⁻ exits basolaterally → returned to blood
2. Titratable Acid Excretion (Collecting Duct)
- α-IC cells secrete H⁺ via H⁺-ATPase
- H⁺ combines with filtered phosphate (HPO₄²⁻ → H₂PO₄⁻) → excreted
- Each H⁺ excreted with a titratable acid generates one "new" HCO₃⁻ added to the blood
3. Ammoniagenesis (Proximal Tubule + Collecting Duct)
- Glutamine → NH₄⁺ in proximal tubule (via glutaminase)
- NH₄⁺ secreted via NHE3 (substitutes for H⁺)
- NH₄⁺ reabsorbed in TAL (via NKCC2 in K⁺ position) → concentrated in medullary interstitium
- NH₃ diffuses into collecting duct lumen → combines with secreted H⁺ → NH₄⁺ excreted in urine
- Each NH₄⁺ excreted generates one "new" HCO₃⁻ → most important buffer in chronic metabolic acidosis
In chronic metabolic acidosis, ammoniagenesis can increase 5-10-fold to compensate.
10. GFR Measurement and Staging of CKD
Estimation equations:
| Equation | Formula |
|---|---|
| CKD-EPI (preferred) | Based on serum creatinine, age, sex |
| MDRD | 4-variable version |
| Cockcroft-Gault | CrCl = [(140-age) × weight] / (72 × SCr) × 0.85 (female) |
CKD Staging (KDIGO):
| Stage | GFR (mL/min/1.73m²) | Description |
|---|---|---|
| G1 | ≥90 | Normal or high (with kidney damage markers) |
| G2 | 60-89 | Mildly decreased |
| G3a | 45-59 | Mildly to moderately decreased |
| G3b | 30-44 | Moderately to severely decreased |
| G4 | 15-29 | Severely decreased |
| G5 | <15 | Kidney failure |
Albuminuria categories (KDIGO):
| Category | Albumin/Creatinine Ratio (ACR) |
|---|---|
| A1 | <30 mg/g (normal to mildly increased) |
| A2 | 30-300 mg/g (moderately increased) |
| A3 | >300 mg/g (severely increased) |
Both GFR and albuminuria independently predict CKD progression, CVD risk, and mortality.
11. Acute Kidney Injury (AKI) - MSN Framework
KDIGO definition: Increase in SCr ≥0.3 mg/dL within 48 hrs, or ≥1.5× baseline within 7 days, or UO <0.5 mL/kg/hr for >6 hrs.
Classification:
| Category | Mechanism | FENa | BUN:Cr ratio | Urine Na | Urine osmolality |
|---|---|---|---|---|---|
| Pre-renal | ↓ perfusion | <1% | >20:1 | <20 mEq/L | >500 mOsm/L |
| Intrinsic renal (ATN) | Tubular damage | >2% | ~10-15:1 | >40 mEq/L | ~300 mOsm/L (isosthenuria) |
| Post-renal | Obstruction | Variable | >20:1 | Variable | Variable |
12. Key Renal Hormones and Functions Summary
| Hormone/Substance | Source | Renal Effect |
|---|---|---|
| ADH (vasopressin) | Posterior pituitary | ↑ AQP2 in CD → water reabsorption |
| Aldosterone | Adrenal cortex | ↑ ENaC → Na⁺ reabsorption; ↑ K⁺/H⁺ secretion |
| ANP/BNP | Atria/ventricles | Natriuresis, ↓ renin, ↓ aldosterone, vasodilation |
| PTH | Parathyroid | ↑ Ca²⁺ reabsorption (DCT); ↓ phosphate reabsorption (PCT); ↑ calcitriol synthesis |
| Calcitriol (1,25-OH₂ D₃) | Kidney (1α-hydroxylase) | ↑ Ca²⁺ and phosphate absorption from gut |
| Erythropoietin (EPO) | Peritubular fibroblasts | Stimulates RBC production in bone marrow |
| Prostaglandins (PGE₂, PGI₂) | Kidney | Vasodilate afferent arteriole; maintain GFR under stress |
Clinical note: NSAIDs inhibit prostaglandin synthesis → afferent arteriolar constriction → ↓ GFR → can precipitate AKI especially in volume-depleted patients, elderly, or those with CKD or HF.
Quick Reference - Normal Renal Values
| Parameter | Normal Value |
|---|---|
| GFR | 90-120 mL/min/1.73m² |
| Daily urine output | 800-2000 mL/day |
| Urine osmolality | 50-1200 mOsm/L |
| Urine specific gravity | 1.001-1.035 |
| Urine Na⁺ | 40-220 mEq/day (diet-dependent) |
| FENa (pre-renal) | <1% |
| Serum creatinine (male) | 0.7-1.3 mg/dL |
| Serum creatinine (female) | 0.5-1.1 mg/dL |
| BUN | 7-20 mg/dL |
| BUN:Creatinine ratio | 10:1-20:1 |
Sources:
- Brenner & Rector's The Kidney, 2-Volume Set - Chapter 2: The Nephron
- NKF Primer on Kidney Diseases, 8e - Chapters 1: Nephron Segments, Salt and Volume Regulation, Countercurrent Mechanism
- Goldman-Cecil Medicine - Bicarbonate and the Kidney in Acid-Base Balance
- Wheater's Functional Histology - Renal Corpuscles & Blood Filtration
This is a shared conversation. Sign in to Orris to start your own chat.