Thyroid
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive content to write a thorough, well-illustrated answer on thyroid anatomy and physiology.
The Thyroid Gland: Anatomy & Physiology
Gross Anatomy
The thyroid is a butterfly-shaped, highly vascular endocrine gland located in the anterior neck, below and lateral to the thyroid cartilage. It has two lateral lobes connected by a narrow isthmus, which crosses the anterior surfaces of the 2nd and 3rd tracheal cartilages. The lobes cover the anterolateral surfaces of the trachea, cricoid cartilage, and the lower thyroid cartilage.
The gland lies deep to the sternohyoid, sternothyroid, and omohyoid muscles, enclosed within the pretracheal layer of cervical fascia (the visceral compartment of the neck).
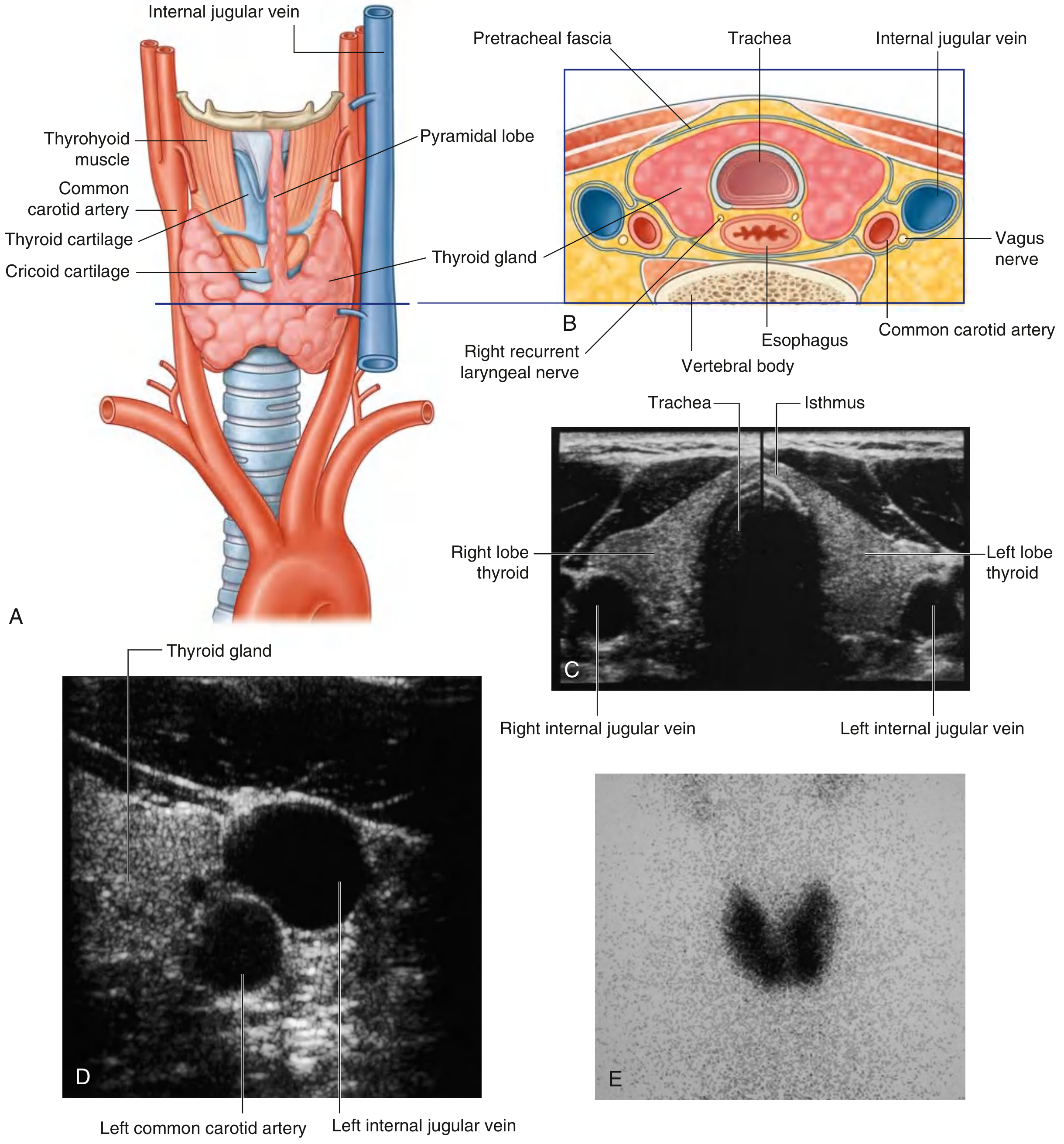
A pyramidal lobe may extend upward from the isthmus (usually on the left side) along the path of the thyroglossal duct.
Embryology & Development
The thyroid develops as a midline outgrowth (evagination) of the pharyngeal epithelium (foregut endoderm) near the base of the developing tongue, at the site known as the foramen cecum. It descends via the thyroglossal duct to its adult position anterior to the trachea in the root of the neck.
- The thyroglossal duct usually disappears early in development
- Remnants can persist as a thyroglossal duct cyst (presents as a midline neck swelling) or fistula
- Arrest along the descent can produce ectopic thyroid tissue, including a lingual thyroid at the tongue base
(Gray's Anatomy for Students, p. 1157)
Blood Supply
Arterial
| Artery | Origin | Supplies |
|---|---|---|
| Superior thyroid artery | First branch of the external carotid artery | Superior pole; anterior branch anastomoses across isthmus; posterior branch may meet inferior thyroid artery |
| Inferior thyroid artery | Thyrocervical trunk (from 1st part of subclavian artery) | Lower pole; ascending branch supplies parathyroid glands |
| Thyroid ima artery (occasional) | Brachiocephalic trunk or aortic arch | Anterior surface of trachea/isthmus |
Venous Drainage
Three veins drain the thyroid:
- Superior thyroid vein → internal jugular vein
- Middle thyroid vein → internal jugular vein
- Inferior thyroid veins → right and left brachiocephalic veins respectively
(Gray's Anatomy for Students, p. 1158-1159)
Lymphatic Drainage
Lymphatics drain to paratracheal nodes beside the trachea and to deep cervical nodes (inferior to the omohyoid muscle along the internal jugular vein). This is clinically important in thyroid cancer staging.
Nerve Supply & Key Surgical Relations
The thyroid has an intimate relationship with the recurrent laryngeal nerves (RLN), branches of the vagus nerve [CN X]:
- The right RLN loops around the right subclavian artery
- The left RLN loops around the arch of the aorta
- Both ascend in the tracheo-esophageal groove and pass deep to the posteromedial surface of the lateral thyroid lobes before entering the larynx
The RLN runs near the inferior thyroid artery and may pass through Berry's ligament (the ligament of Gruber), which binds the thyroid to the trachea and cricoid cartilage. Damage to the RLN during thyroid surgery causes hoarseness (unilateral) or potentially fatal airway compromise (bilateral).
(Gray's Anatomy for Students, p. 1159-1160)
Histology
The thyroid is the only endocrine gland that stores its secretory product extracellularly - and in large quantities (enough for up to 3 months without further synthesis).
Structural organisation:
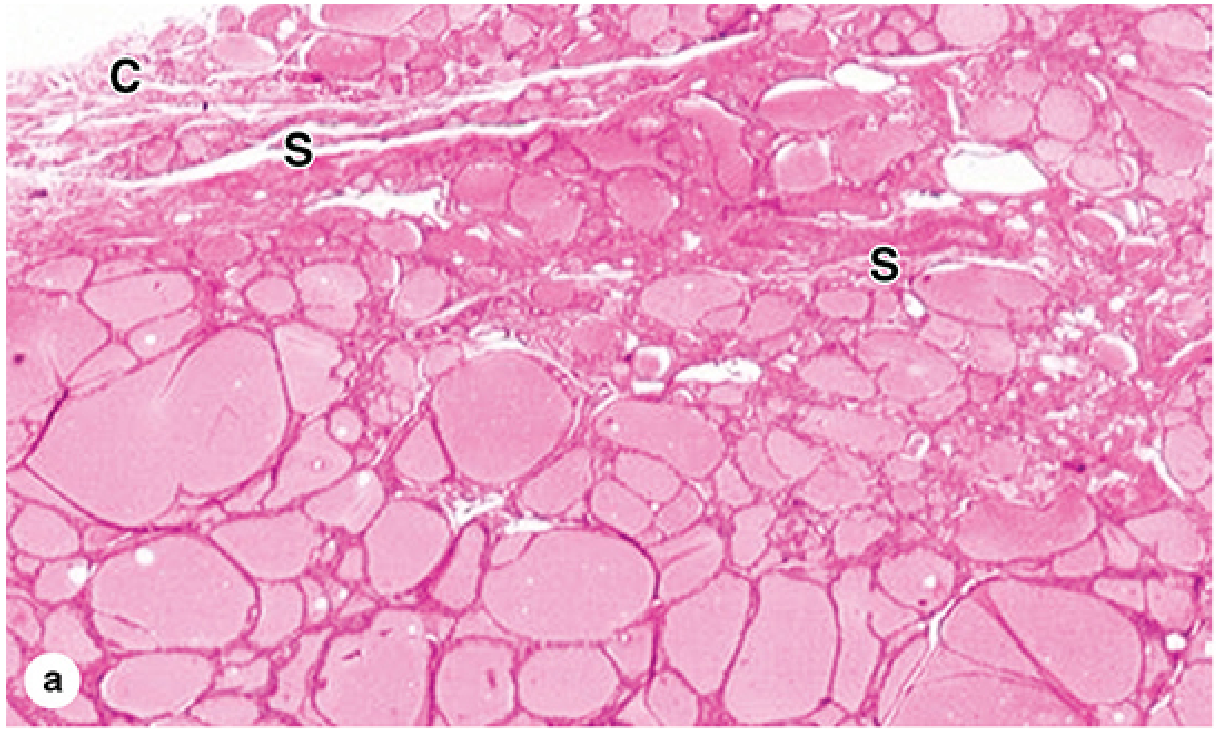
- Covered by a fibrous capsule; septa extend inward dividing the parenchyma into lobules carrying blood vessels, nerves, and lymphatics
- Each lobule contains 20-40 follicles
Thyroid follicle - the functional unit:
- A spherical structure lined by simple follicular epithelium (thyrocytes)
- Central lumen densely filled with colloid - a gelatinous, acidophilic material containing thyroglobulin (a 660 kDa glycoprotein), the precursor to thyroid hormones
- Thyrocytes range from squamous (hypoactive gland) to low columnar (active gland) - their height is a direct indicator of functional activity
- Thyrocytes are rich in rough ER basally, and have Golgi complexes, secretory granules, lysosomes, and microvilli apically (facing the colloid)
Parafollicular cells (C cells):
- Located in or between follicles, within the basement membrane but not touching the colloid
- Larger, paler-staining than thyrocytes
- Secrete calcitonin - a polypeptide involved in calcium metabolism (lowers serum calcium by inhibiting osteoclasts)
- Derived from neural crest cells (not from foregut endoderm like thyrocytes)
- Origin of medullary thyroid carcinoma
(Junqueira's Basic Histology, p. 1034-1036)
Physiology: Hormone Synthesis & the HPT Axis
The thyroid produces two main hormones: T4 (thyroxine / tetraiodothyronine) and T3 (triiodothyronine), and regulates a third: calcitonin.
Hypothalamus-Pituitary-Thyroid (HPT) Axis
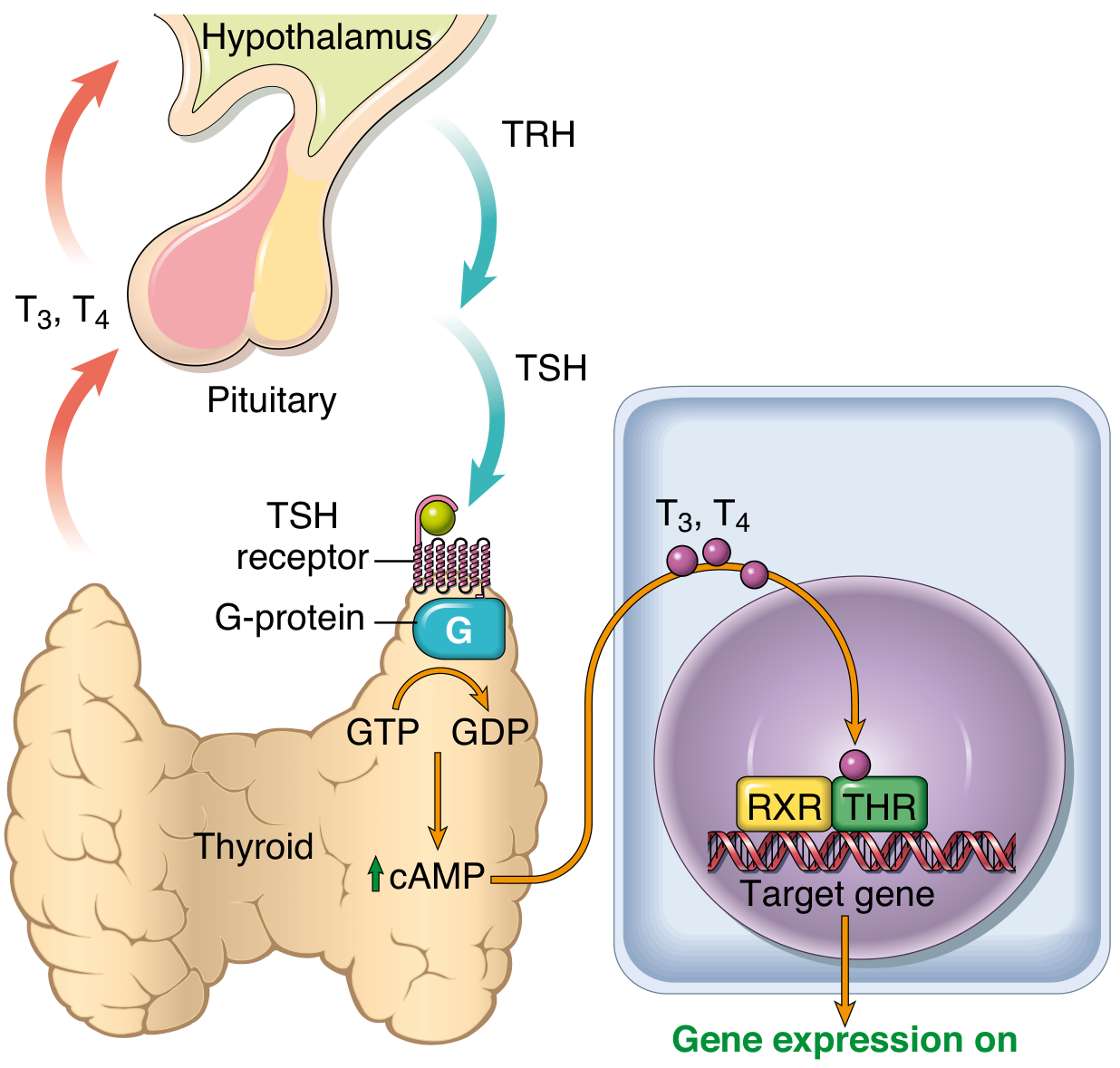
- Hypothalamus releases TRH (thyrotropin-releasing hormone)
- TRH stimulates anterior pituitary thyrotrophs to release TSH (thyroid-stimulating hormone / thyrotropin)
- TSH binds to the TSH receptor on thyroid follicular cells - a Gs protein-coupled receptor
- Gs protein activation → ↑ cAMP → activates cAMP-dependent protein kinases
- This stimulates thyroid growth and T3/T4 synthesis and release
- Rising T3/T4 provide negative feedback to both the hypothalamus and pituitary
T3/T4 Synthesis Steps (in follicular cells)
- Iodide uptake from blood via the sodium-iodide symporter (NIS) at the basolateral membrane
- Iodide is oxidised to iodine by thyroid peroxidase (TPO) at the apical surface
- Thyroglobulin (synthesised in follicular cells) is secreted into the colloid
- Organification: iodine is attached to tyrosine residues on thyroglobulin to form MIT (monoiodotyrosine) and DIT (diiodotyrosine)
- Coupling: MIT + DIT → T3; DIT + DIT → T4
- On TSH stimulation, follicular cells endocytose colloid droplets (pseudopodia extend into the lumen)
- Lysosomes digest thyroglobulin, releasing T3 and T4 into the bloodstream
Transport & Peripheral Conversion
- Most circulating T3 and T4 are bound to thyroxine-binding globulin (TBG), transthyretin, and albumin
- Only free (unbound) hormone is biologically active
- In peripheral tissues, the majority of free T4 is deiodinated to T3
- T3 binds thyroid hormone nuclear receptors (TR-alpha, TR-beta) with 10-fold greater affinity than T4 - it is the more potent form
- TR forms a heterodimer with RXR and binds thyroid response elements (TREs) in target gene promoters → gene expression
Physiological Effects of Thyroid Hormones
| System | Effect |
|---|---|
| Metabolism | ↑ basal metabolic rate; stimulates carbohydrate and lipid catabolism; promotes protein synthesis |
| Cardiovascular | ↑ heart rate and cardiac output; sensitises heart to catecholamines |
| Nervous system | Critical for fetal and neonatal brain development (deficiency causes cretinism/intellectual disability) |
| Bone | Normal linear growth and skeletal maturation |
| Thermogenesis | ↑ heat production (calorigenic effect) |
(Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 993-995)
Receptor Mutations & Clinical Correlations
- THRB gene mutations (TR-beta): tissue resistance to thyroid hormone → elevated T3/T4 levels with ineffective feedback inhibition of hypothalamus/pituitary
- THRA gene mutations (TR-alpha): mildly low T4, elevated T3/T4 ratio, skeletal abnormalities
- Thyroglossal duct cyst: midline neck mass, moves up on tongue protrusion; treated by Sistrunk procedure (removal of cyst + mid-portion of hyoid bone)
Sources:
- Gray's Anatomy for Students (Gray's, p. 1157-1160)
- Junqueira's Basic Histology, 17th ed. (p. 1034-1036)
- Robbins, Cotran & Kumar Pathologic Basis of Disease (p. 993-995)
This is a shared conversation. Sign in to Orris to start your own chat.