Tell me about clinical feature of horners syndrome, explain more about enophthalmos
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
"Horner syndrome" AND enophthalmos
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Horner Syndrome - Clinical Features
Horner syndrome (also called oculosympathetic palsy or Bernard-Horner syndrome) results from interruption of the three-neuron sympathetic pathway supplying the eye and face. The classic triad is miosis, ptosis, and anhidrosis.
Sympathetic Pathway (Three Neurons)
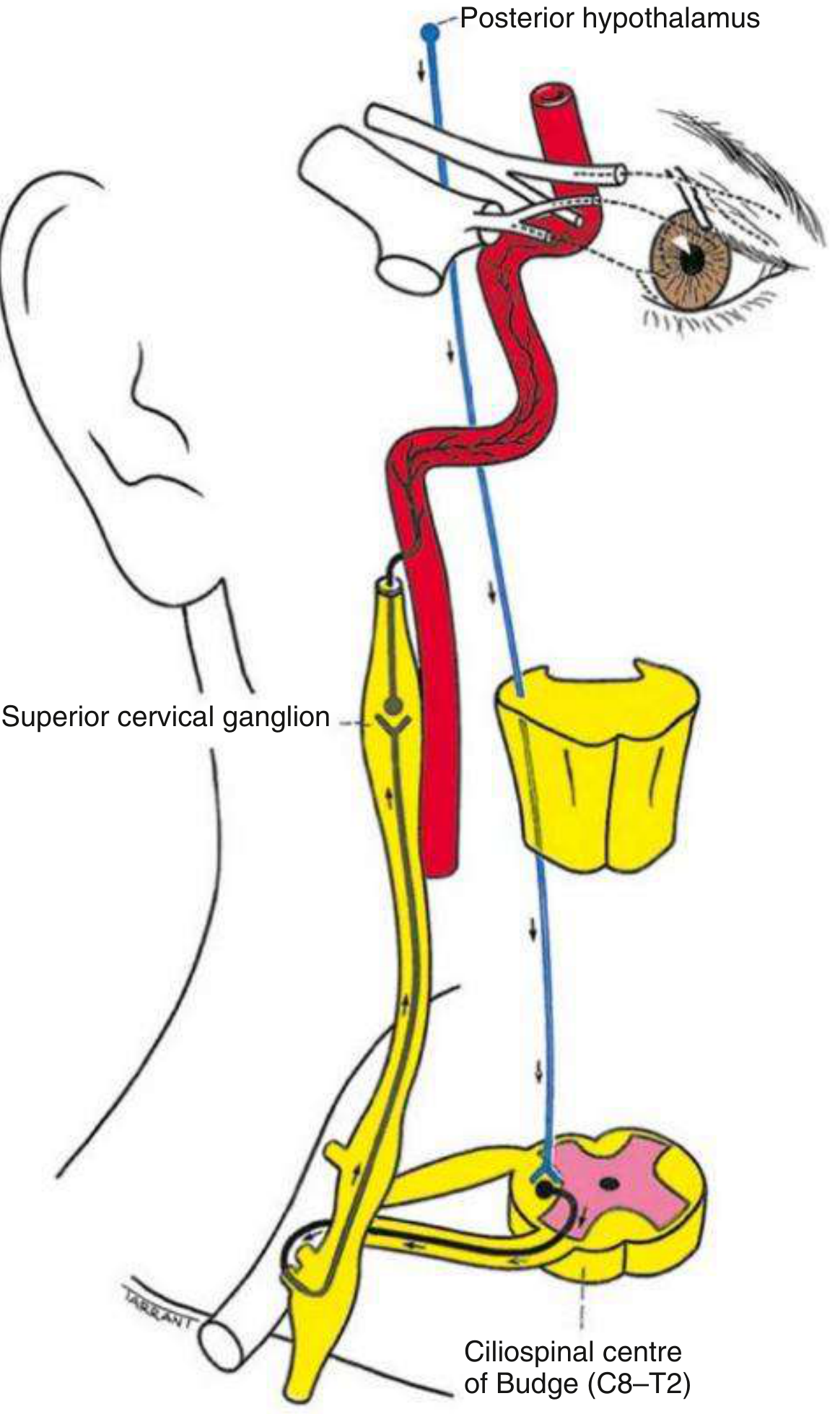
- 1st neuron (central): Posterior hypothalamus → descends uncrossed through the brainstem → terminates in the ciliospinal centre of Budge (C8-T2) in the intermediolateral horn of the spinal cord.
- 2nd neuron (preganglionic): Exits the ciliospinal centre → passes around the apex of the lung (vulnerable to Pancoast tumor) → synapses in the superior cervical ganglion.
- 3rd neuron (postganglionic): Ascends along the internal carotid artery → through the cavernous sinus → joins the ophthalmic division of V → reaches the dilator pupillae and tarsal muscles via the nasociliary and long ciliary nerves.
Clinical Features
Core (Classic) Triad
| Feature | Mechanism | Details |
|---|---|---|
| Miosis | Loss of sympathetic input to dilator pupillae; sphincter pupillae acts unopposed | Anisocoria is more pronounced in dim light (dilation lag); direct and consensual light reflexes remain intact |
| Ptosis (upper lid) | Paralysis of Müller's smooth muscle (superior tarsal muscle) | Usually mild, 1-2 mm; distinct from oculomotor nerve palsy |
| Anhidrosis | Loss of sudomotor fiber innervation | Ipsilateral face/neck; only present if lesion is below the superior cervical ganglion (sudomotor fibers run along the external carotid artery) |
Additional Signs
"Upside-down ptosis" (reverse ptosis / lower lid elevation)
The inferior tarsal smooth muscle also receives sympathetic innervation. Its paresis causes the lower eyelid to rise slightly, narrowing the palpebral fissure from below as well as above. This is sometimes called the "reverse ptosis sign."
Dilation lag
The Horner pupil redilates very slowly when lights are dimmed. There is more anisocoria at 5 seconds after lights off than at 15 seconds. This is the single most reliable clinical sign differentiating Horner syndrome from benign physiologic anisocoria, though it is demonstrable in only ~50% of cases.
Heterochromia iridis (hypochromic heterochromia)
The affected iris appears lighter/paler because melanin deposition in the iris requires intact sympathetic innervation. This is typically seen in congenital Horner syndrome (before age 2), or in longstanding acquired cases. In congenital cases, the affected iris is gray rather than brown.
Apparent enophthalmos - see detailed section below
Conjunctival hyperemia and transient ocular hypotony - especially in the acute phase, from loss of sympathetic vasoconstrictor tone.
Increased accommodation / accommodative paresis - patients may hold reading material closer than normal.
Ipsilateral vasodilation - from loss of sympathetic control of subcutaneous vessels; affected side may feel warmer.
Enophthalmos in Horner Syndrome - Detailed Explanation
Is it Real or Apparent?
This is a key teaching point. The "enophthalmos" of Horner syndrome is almost certainly apparent rather than true - meaning the eyeball is not actually recessed further back into the orbit. Multiple authoritative texts agree on this:
"Retraction of the eyeball (enophthalmos), considered a component of the syndrome, is probably an illusion created by narrowing of the palpebral fissure."
- Adams and Victor's Principles of Neurology, 12th Ed.
"Apparent enophthalmos" (used explicitly, not "true enophthalmos")
- Localization in Clinical Neurology, 8e
Why Does It Look Like the Eye Is Sunken?
The visual appearance of a sunken eye in Horner syndrome has two contributing mechanisms:
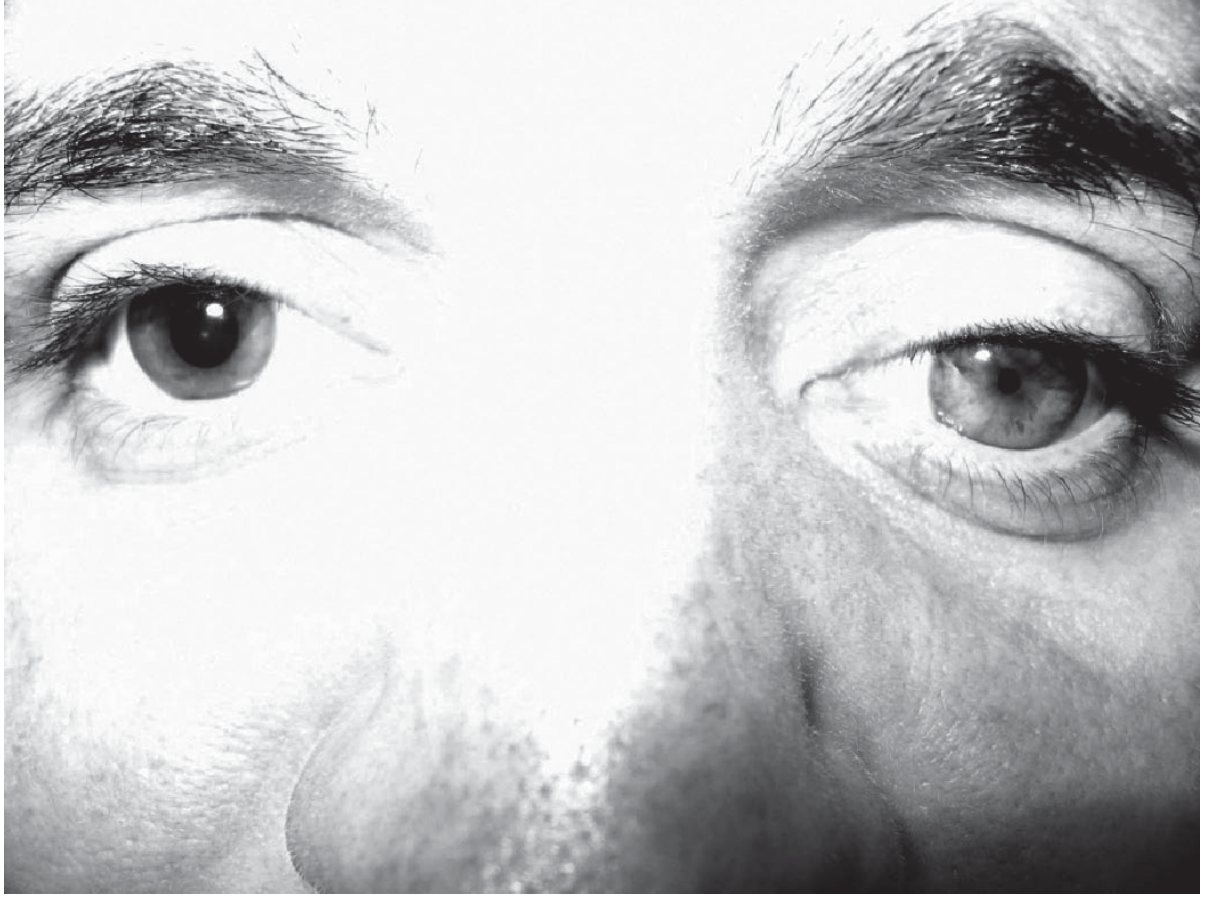
1. Narrowing of the palpebral fissure (the dominant explanation)
Both the upper and lower lids are affected:
- Upper lid drops (ptosis from Müller muscle paresis) - narrows the fissure from above
- Lower lid elevates (reverse ptosis from inferior tarsal muscle paresis) - narrows the fissure from below
This narrowing of the visible "window" around the eye creates the strong impression that the globe is set back further in the orbit. When you see less of a globe, it looks smaller and deeper. This is a purely optical illusion - the globe position has not changed.
2. Paralysis of the orbitalis muscle (proposed anatomical cause)
Gray's Anatomy for Students explains:
"Enophthalmos (sinking of the eye) - believed to result from paralysis of the orbitalis muscle, although this is an uncommon feature of Horner's syndrome. The orbitalis muscle is composed of smooth muscle fibers that span the inferior orbital fissure and helps maintain the forward position of orbital contents."
The orbitalis (of Müller) is a smooth muscle band that bridges the inferior orbital fissure. It receives sympathetic innervation and normally acts to push orbital contents slightly forward. When sympathetic input is lost, this muscle relaxes, theoretically allowing the globe to drift posteriorly. However, most modern clinicians and texts consider this a minor, often undetectable contribution compared to the palpebral fissure effect.
Practical Clinical Implication
Because enophthalmos in Horner syndrome is apparent (not true), formal exophthalmometry (Hertel measurements) typically does not confirm real globe recession. If true enophthalmos is measured by exophthalmometry, you should look for other causes (orbital floor fracture with fat herniation, metastatic scirrhous breast carcinoma causing orbital fibrosis, etc.) rather than attributing it to Horner syndrome alone.
Harrison's Principles of Internal Medicine (22e, 2025) reinforces this:
"A small globe or Horner's syndrome can give the appearance of enophthalmos."
Causes by Neuron Level
| Level | Examples |
|---|---|
| 1st neuron (central) | Lateral medullary (Wallenberg) infarct, brainstem tumor, syringomyelia, demyelination, cervical cord lesion |
| 2nd neuron (preganglionic) | Pancoast tumor, carotid/aortic dissection or aneurysm, thoracic cord lesion, neck trauma/surgery, enlarged lymph nodes |
| 3rd neuron (postganglionic) | Internal carotid artery dissection (painful, acute - must rule out urgently), cavernous sinus mass, nasopharyngeal tumor, cluster headache, otitis media |
Clinical pearl: Painful acute Horner syndrome, especially with ipsilateral neck/face pain, should immediately raise the suspicion of carotid artery dissection and warrants urgent vascular imaging (MRI/MRA or CTA). Most isolated postganglionic Horner syndromes without pain are microvascular in etiology.
Pharmacological Testing
| Drug | Purpose | Horner pupil result |
|---|---|---|
| Apraclonidine 0.5-1% (preferred) | Confirms diagnosis | Dilates (denervation supersensitivity to alpha agonist); normal pupil unaffected. Also improves ptosis. |
| Cocaine 4-10% | Confirms diagnosis (blocks NE reuptake) | Fails to dilate (no NE to accumulate at synapse) |
| Hydroxyamphetamine 1% | Localizes lesion (pre vs. postganglionic) | Dilates in preganglionic; fails to dilate in postganglionic (no NE stores in degenerated 3rd neuron) |
Note: There is a latent period of approximately 7 days before the apraclonidine test becomes positive in acute Horner syndrome.
Sources: Adams and Victor's Principles of Neurology 12e | Kanski's Clinical Ophthalmology 10e | Neuroanatomy through Clinical Cases 3e | Localization in Clinical Neurology 8e | Gray's Anatomy for Students | Harrison's Principles of Internal Medicine 22e (2025) | Ganong's Review of Medical Physiology 26e
This is a shared conversation. Sign in to Orris to start your own chat.