
photo-1784453944471.jpg
Explain this
Reading File
analyse_media
This image is a page from a psychiatry/neuroscience textbook (ARISE Medical) covering Chapter 5: Sleep Disorders. Here's a full breakdown of all the notes:
1. REM Sleep (Paradoxical Sleep)
REM = Rapid Eye Movement
- Rate of Metabolism increases
- PR (Pulse Rate), BP (Blood Pressure), and O2 to Brain all increase
- Penile erection occurs - and this happens only during REM sleep (lasts ~15 min)
- This is physiologically normal and is used clinically to distinguish psychogenic from organic erectile dysfunction
- Total REM duration: ~8 hours per night (lifetime average across a full night)
- Males: 6-7 hours of REM
- Females: 7-8 hours of REM
- Dreams occur during REM - maximum dreaming happens here
- Recall of dreams is possible from REM sleep
2. NREM Sleep (Slow Wave Sleep)
NREM = Non-Rapid Eye Movement = Deep Sleep
- Occupies about 6.5 hours of a full night's sleep
- Associated with Somnambulism (Sleep Walking)
- Admission/observation period for sleepwalking = 30 days
- NREM is restorative/deep sleep - the body repairs and grows during this phase
3. Brain Waves (States of Consciousness)
The notes describe 4 states of brain wave activity:
| State | Description |
|---|---|
| Alpha (α) | Awake-like state (eyes closed, relaxed) |
| Beta (β) | Fully Awake |
| Theta (θ) | Entering deep sleep |
| Delta (δ) | Deep Sleep |
The note also mentions: "Whenever you are closing your eyes or wake with come even in meditation" - referring to the alpha wave state that appears when you close your eyes or meditate.
4. Forensic Psychiatry Note - Admission Period
- Admit = 30 days is written prominently
- This refers to the mandatory observation/admission period for psychiatric evaluation in medicolegal cases
5. Real vs. Fake Psychiatric Patient Comparison Table
This is a classic forensic psychiatry table used to distinguish genuine psychiatric illness from malingering (faking mental illness):
| Feature | Real Psychiatric Patient | Fake (Malingering) Patient |
|---|---|---|
| Who will be more cooperative? | ✓ (More cooperative) | ⊖ (Less cooperative, evasive) |
| Whose behavior will always be the same? | Same (consistent) | Changing (inconsistent) |
| Court follow-up (Court F/W/S) | ✓ (Present) | ⊖ (Avoids) |
| Dehydrated | ✓ (Present) | ⊖ (Not present) |
| Motive | ⊖ (No secondary gain motive) | N then ✓ (Has motive - e.g., to avoid legal punishment) |
Key clinical point: A real psychiatric patient tends to be more cooperative, shows consistent behavior, may be dehydrated (from neglect), and has no secondary gain motive. A malingerer (faker) tends to be uncooperative, shows inconsistent/changing behavior, avoids court follow-up, and clearly has a motive (like escaping criminal charges).
Summary: These notes cover the physiological differences between REM and NREM sleep, brain wave patterns across sleep stages, and forensic psychiatric criteria to detect malingering - a common exam topic in psychiatry and forensic medicine.
Explain me REM paradoxical sleep. And NREM slow wave sleep. Explain the difference between these two and all details.
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Here is a thorough, textbook-level explanation of REM and NREM sleep - all differences, physiology, and clinical relevance.
REM vs. NREM Sleep - Complete Guide
Sleep Architecture: The Big Picture
A full night of sleep is not uniform - you cycle between REM and NREM sleep approximately every 90 minutes, repeating 4-5 times per night. Early cycles are dominated by deep NREM; later cycles shift toward more REM.
Here is how sleep stages distribute across age groups (from Adams and Victor's Principles of Neurology):
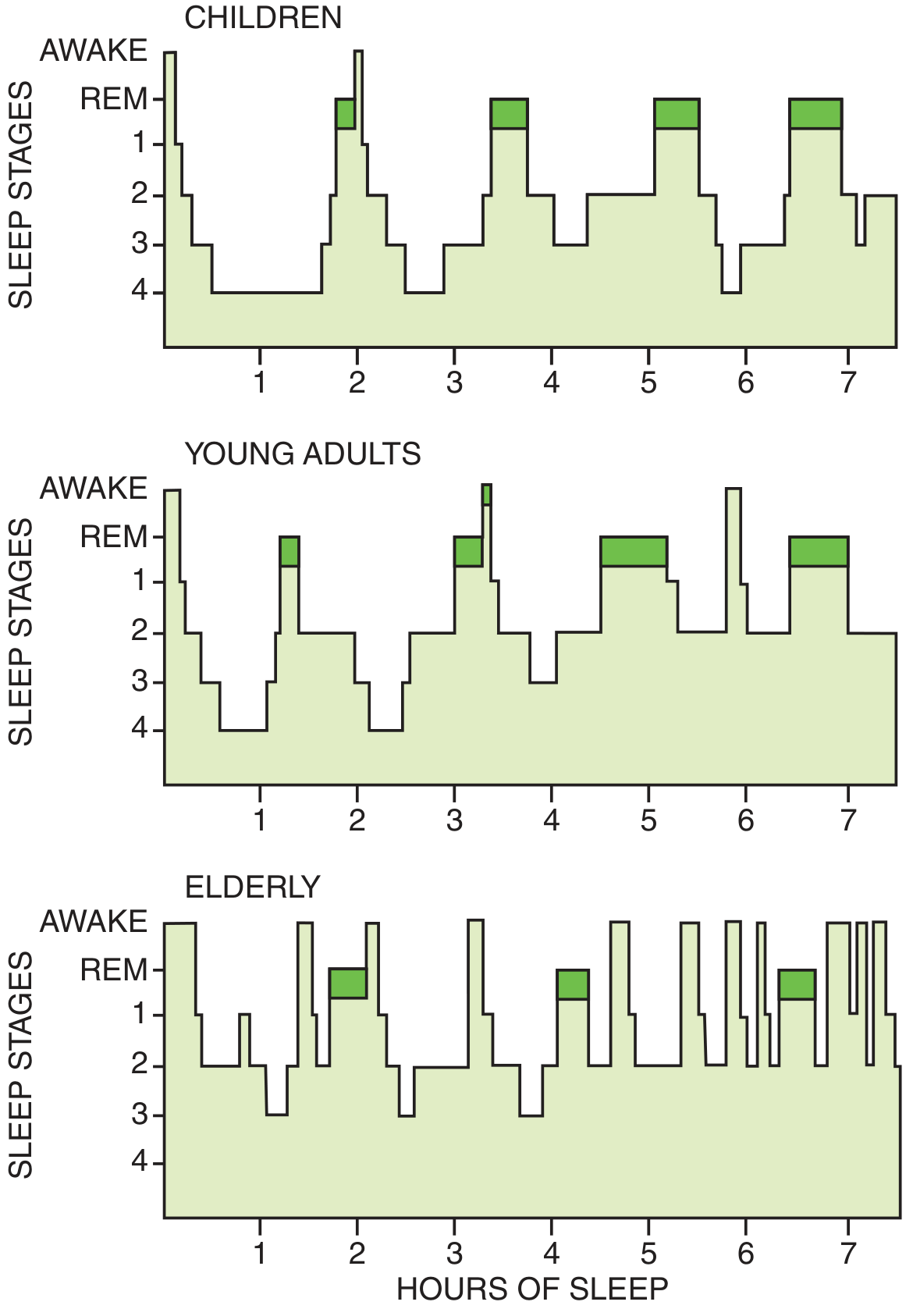
Notice: deep sleep (Stage 4) nearly disappears in the elderly, while REM remains relatively preserved.
NREM Sleep (Non-Rapid Eye Movement = Slow Wave Sleep)
What it is
NREM is the first type of sleep you enter. It has three stages (N1, N2, N3) progressing from light to deep.
NREM Stages
| Stage | Old Name | EEG Waves | State |
|---|---|---|---|
| N1 | Stage 1 | Theta (4-7 Hz) | Drowsy / falling asleep |
| N2 | Stage 2 | Sleep spindles + K complexes (12-14 Hz) | Light sleep |
| N3 | Stages 3+4 | High-voltage Delta waves | Deep sleep (Slow Wave Sleep) |
- As you enter sleep, EEG slows from alpha (8-12 Hz, awake/relaxed) -> theta (N1) -> spindles/K-complexes (N2) -> delta (N3)
- Cortical neurons fire in synchronized bursts - this is why EEG shows large, slow waves
- N3 = Slow Wave Sleep - this is the deepest, most restorative stage
NREM Physiology
Cardiovascular & Autonomic:
- Heart rate slows and becomes regular
- Blood pressure decreases
- Sympathetic activity decreases; parasympathetic (vagal) tone increases
- Cerebral blood flow and brain metabolism markedly reduced
Respiratory:
- Breathing is slow and regular
- Only the metabolic (automatic) respiratory system is active
- Muscle tone in upper airway decreases slightly
- Tidal volume decreases; CO2 rises mildly (2-8 mmHg), O2 drops slightly
Temperature:
- Body temperature falls - most of the nightly temperature decline occurs in NREM
Hormones:
- Growth Hormone (GH) is secreted maximally during N3 slow wave sleep - critical for tissue repair, muscle growth, and immunity
Muscle tone:
- Present but reduced
Arousal:
- Hard to wake someone from N3 - they are confused and disoriented if forcibly awakened (called "sleep inertia")
Brain activity:
- Neuron firing rates decrease during NREM
Clinical conditions arising from NREM (specifically N3):
- Somnambulism (Sleepwalking) - arises from N3
- Night terrors - arise from N3
- Bedwetting (nocturnal enuresis) - occurs in N3
- These are called parasomnias of arousal because they occur when someone partially wakes from deep NREM
REM Sleep (Rapid Eye Movement = Paradoxical Sleep)
Why "Paradoxical"?
It is called paradoxical because the brain is highly active (EEG looks like wakefulness) yet the person is deeply asleep and cannot be easily woken by routine stimuli. The brain is "awake" but the body is paralyzed.
What happens in REM
EEG:
- Desynchronized, low-voltage, fast - looks like the waking EEG
- Theta waves dominate
- Cortical neurons fire in non-synchronized bursts (like wakefulness)
Eye Movements:
- Rapid conjugate eye movements in all directions (more horizontal than vertical)
- Visible through closed eyelids - this is how it was first discovered by Aserinsky and Kleitman in 1953
Muscle Tone:
- Atonia - nearly complete loss of muscle tone (the body is paralyzed)
- Only the diaphragm (breathing) and extraocular muscles retain activity
- This prevents you from physically acting out your dreams
- Small twitches in facial and finger/toe muscles still occur
Cardiovascular & Autonomic - Phasic vs. Tonic REM:
REM has two components - tonic (background) and phasic (bursts):
- Tonic REM: parasympathetic tone increases further; heart rate and BP relatively stable
- Phasic REM: sympathetic bursts cause fluctuating heart rate, blood pressure, and respiration - pupil dilation/constriction alternates
- This is why heart attacks, angina, and strokes are more common in early morning (when REM is longest)
Cerebral Blood Flow & Metabolism:
- Restored to waking levels during REM - the brain is metabolically as active as when awake
Temperature:
- Thermoregulation is suspended during REM - body temperature floats toward ambient temperature (like a poikilotherm)
Respiratory:
- Irregular breathing
- Intercostal muscle tone is markedly suppressed
- Most dangerous period for respiratory compromise in sleep apnea, obesity, neuromuscular disease
Penile Erections:
- Occur exclusively during REM (the image notes state this)
- Clinically useful: if a man has erections during sleep (normal physiology), his erectile dysfunction when awake is likely psychogenic, not organic
Dreams:
- The most vivid, narrative, complex, emotional dreams occur in REM
- Dreams can be recalled if the person wakes during or just after REM
- Some dreaming (more passive) also occurs in NREM, but is less well-recalled
Arousal:
- Easy to wake from REM sleep (lighter sleep relative to N3)
REM proportions across a night:
- Young adults spend ~20-25% of total sleep in REM
- First REM bout: only 5-10 minutes
- REM bouts get longer as the night progresses - so most dreaming happens in the last 2-3 hours of sleep
Side-by-Side Comparison Table
| Feature | NREM Sleep | REM Sleep |
|---|---|---|
| Other names | Slow wave sleep | Paradoxical sleep, Desynchronized sleep |
| Stages | N1, N2, N3 | R (single stage) |
| EEG | Slow, synchronized (delta/theta/spindles) | Fast, desynchronized (like waking) |
| Eye movements | Slow or absent | Rapid, conjugate |
| Muscle tone | Reduced | Nearly absent (atonia) |
| Heart rate | Slow, regular | Variable (phasic bursts) |
| Blood pressure | Decreased, stable | Fluctuating |
| Breathing | Regular, slow | Irregular |
| Cerebral blood flow | Markedly reduced | Restored to waking levels |
| Brain metabolism | Reduced | Equal to wakefulness |
| Body temperature | Falls (thermoregulation active) | Suspended (poikilothermic) |
| Dreaming | Passive/fragmentary | Vivid, narrative, recalled |
| Penile erection | No | Yes |
| Growth Hormone release | Yes (N3) | No |
| Arousability | Hard to wake from N3 | Relatively easy to wake |
| Parasomnia | Sleepwalking, night terrors (N3) | REM sleep behavior disorder |
| % of total sleep | ~75-80% | ~20-25% |
| When dominant | Early in night | Late in night (early morning) |
| Autonomic | Decreased sympathetic | Phasic sympathetic surges |
The Sleep Cycle Across a Night
- You fall asleep -> N1 -> N2 -> N3 (takes ~45-60 min)
- You briefly ascend back to N1
- First REM bout occurs (~5-10 min)
- Repeat - each cycle ~90 min
- With each cycle: N3 gets shorter, REM gets longer
- By the last cycle: almost no N3; mostly N2 and long REM bouts
Key Memory Points (Exam Focus)
- REM = paradoxical because EEG is awake-like but person is asleep
- NREM N3 = slow wave because of high-voltage delta waves
- Sleepwalking, night terrors come from NREM N3 (not REM - common exam mistake)
- REM sleep behavior disorder = acting out dreams because atonia fails
- Penile erections only in REM - test for psychogenic vs. organic ED
- Growth hormone only in N3 - why children need deep sleep to grow
- Most dreaming recalled from REM - but dreaming occurs in both
- REM atonia protects you from acting out dreams; its failure = REM sleep behavior disorder (associated with Parkinson's disease and Lewy body dementia)
Sources: Adams and Victor's Principles of Neurology 12th Ed.; Bradley and Daroff's Neurology in Clinical Practice; Plum and Posner's Diagnosis and Treatment of Stupor and Coma
This is a shared conversation. Sign in to Orris to start your own chat.