Clinical discussion of pih
Reading File
Finding Sources
Finding Sources
Searching PubMed
"preeclampsia" AND "management"
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks to provide a thorough clinical discussion. Let me compile the full response.
Pregnancy-Induced Hypertension (PIH): Clinical Discussion
1. Definition and Classification
PIH refers to hypertensive disorders that arise after 20 weeks of gestation in a previously normotensive woman, and completely resolve following delivery. It is an umbrella term covering a spectrum:
| Category | Definition |
|---|---|
| Gestational Hypertension | New BP ≥ 140/90 mmHg after 20 weeks; no proteinuria; resolves postpartum |
| Preeclampsia | Gestational hypertension + proteinuria (>300 mg/24 hr) or end-organ damage signs |
| Severe Preeclampsia | BP ≥ 160/110 mmHg with evidence of multi-organ dysfunction |
| Eclampsia | Seizures/coma in a preeclamptic patient (unexplained by another cause) |
| HELLP Syndrome | Hemolysis + Elevated Liver enzymes + Low Platelets; severe variant |
| Chronic hypertension with superimposed preeclampsia | Pre-existing HTN + new proteinuria or worsening BP after 20 weeks |
| Chronic/coincidental hypertension | Present before pregnancy or persisting >6 weeks postpartum |
Hypertension complicates up to 8-10% of all pregnancies. The incidence of hypertensive disorders of pregnancy is approximately 85 per 1000 deliveries in the United States. - Creasy & Resnik's Maternal-Fetal Medicine, p. 1057
2. Epidemiology and Risk Factors
- Nulliparity is the greatest population-attributable risk factor (32.3%)
- Young maternal age (< 20 years) and advanced age (> 35 years)
- Prior preeclampsia, family history, antiphospholipid syndrome
- Chronic hypertension: 25% will develop superimposed preeclampsia
- Pregestational diabetes: ~20% overall risk; up to 70% with vascular disease (White's class F/R)
- Connective tissue disorders (SLE), chronic renal disease
- Multiple gestation, molar pregnancy, obesity, hypercholesterolemia
- IVF pregnancies
- African-American race (particularly associated with more severe disease)
3. Pathophysiology
The fundamental defect is inadequate trophoblastic invasion of the spiral arteries.
Normal vs. Preeclampsia
In a normal pregnancy, trophoblasts invade the spiral arteries of the uterine endometrium, remodeling them into wide, low-resistance sinusoids. In preeclampsia, this vascular remodeling fails - the musculoelastic walls are retained and channels remain narrow, leading to placental ischemia.
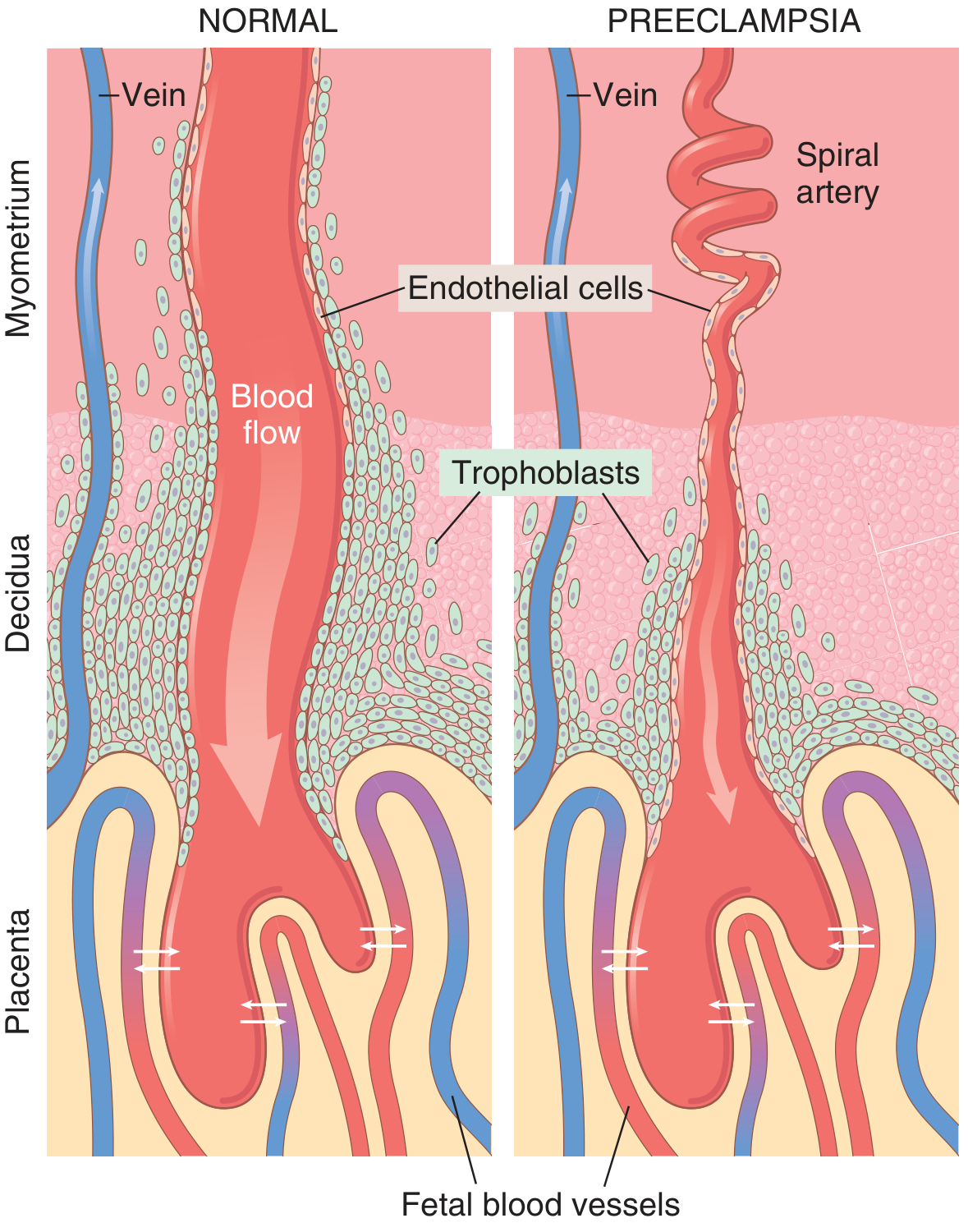
Figure: In normal pregnancy (left), trophoblasts fully invade and dilate the spiral arteries. In preeclampsia (right), inadequate invasion leaves narrow, high-resistance vessels with reduced placental perfusion. - Guyton & Hall Textbook of Medical Physiology
Cascade of Events
-
Placental ischemia/hypoxia → release of antiangiogenic factors into maternal circulation:
- Soluble Flt-1 (sFlt-1) - antagonizes VEGF
- Soluble endoglin - antagonizes TGF-β
- Increased inflammatory cytokines (TNF-α, IL-6)
-
Maternal endothelial dysfunction → systemic effects:
- Reduced production of vasodilators: prostacyclin (PGI₂), prostaglandin E₂
- Increased production of vasoconstrictor: thromboxane A₂
- Net result: vascular hyperreactivity and hypertension
-
Consequences:
- Hypertension from vasoconstriction
- Proteinuria from glomerular endotheliosis (thickened glomerular tufts with protein deposits in basement membranes)
- Hypercoagulability from endothelial dysfunction + decreased antithrombotic PGI₂
- Placental infarction from chronic hypoperfusion
- End-organ damage - kidneys, liver, brain
Note: Despite this being called "high output" early, in established preeclampsia the cardiac output drops as peripheral resistance rises markedly. - Rosen's Emergency Medicine
4. Pathological Morphology
Placenta
- Multiple infarcts (more numerous than in normal pregnancy)
- Retroplacental hemorrhage
- Ischemic changes: increased syncytial knots (aggregates of syncytial nuclei at terminal villi)
- Acute atherosis: fibrinoid necrosis + lipid-laden macrophages in decidual vessels
Kidneys
- Glomerular endotheliosis: thickened glomerular tufts, protein deposits in basement membranes
- Reduced GFR and renal blood flow (opposite of normal pregnancy)
Liver (in HELLP)
- Periportal hemorrhage, fibrin deposits in sinusoids
- Hepatocyte necrosis
Brain (in eclampsia)
- Cerebral edema, petechial hemorrhages, thrombotic microangiopathy
5. Clinical Features
Symptoms (onset usually after 34 weeks; earlier with molar pregnancy, pre-existing renal/hypertensive disease)
- Headache (frontal, severe, persistent)
- Visual disturbances - blurring, scotomata, photophobia
- Epigastric / right upper quadrant pain - liver capsule distension
- Nausea, vomiting
- Rapid weight gain, oedema (face, hands - "non-dependent")
- Decreased urine output (oliguria)
Signs
- BP ≥ 140/90 mmHg (severe: ≥ 160/110 mmHg)
- Generalized oedema
- Proteinuria (dipstick ≥ 2+; confirmed by 24-hr urine or protein:creatinine ratio)
- Hyperreflexia with clonus (impending eclampsia)
- Papilloedema (in severe cases)
Eclampsia
- Grand mal convulsions - tonic-clonic
- May be preceded by visual aura, severe headache
- Can occur antepartum (most common), intrapartum, or postpartum (up to 48+ hours after delivery - ~20% of cases are postpartum)
- Seizures must be differentiated from epilepsy, hypoglycemia, drug overdose, intracranial pathology
6. HELLP Syndrome
A particularly severe variant. Diagnostic criteria:
- H - Hemolysis: microangiopathic hemolytic anemia, raised LDH, schistocytes on smear
- EL - Elevated Liver enzymes: ALT and AST > 70 U/L
- LP - Low Platelets: < 100,000/mL
Occurs in approximately 10% of severe preeclampsia cases. May be complicated by DIC.
High-risk groups: mothers with superimposed preeclampsia; older multiparas.
7. Investigations
| Investigation | Purpose |
|---|---|
| Full blood count + platelets | Thrombocytopenia (HELLP), haemoconcentration |
| Liver function tests (ALT, AST, LDH) | Hepatic involvement, HELLP |
| Urea, creatinine | Renal involvement |
| 24-hr urine protein (or spot protein:creatinine ratio) | Quantify proteinuria |
| Uric acid | Often elevated in preeclampsia |
| Coagulation screen (PT, aPTT, fibrinogen) | DIC screening in HELLP/severe disease |
| Blood film | Schistocytes - microangiopathic haemolysis |
| Urine output monitoring | Target > 25 mL/hr |
| Fetal assessment: CTG, biophysical profile, Doppler USS | Fetal wellbeing |
| CT head | If altered consciousness, persistent seizures, focal neurological signs |
8. Management
A. General Principles
The only definitive treatment is delivery. All other measures are temporizing to protect maternal organs and allow fetal maturity. Treatment depends on gestational age, severity, and organ involvement.
B. Antihypertensive Therapy
Initiate drug therapy when:
- Systolic BP > 160 mmHg or
- Diastolic BP > 105-110 mmHg (confirmed for ≥15 minutes)
Untreated severe hypertension is the leading cause of intracranial hemorrhage and maternal death in preeclampsia.
Drugs safe in pregnancy:
| Drug | Route | Dose | Notes |
|---|---|---|---|
| Labetalol | IV (acute) | 20 mg IV bolus; escalate to 40 mg at 10 min; max 300 mg total | Combined α/β blocker; preferred acute agent |
| Oral (chronic) | 100 mg twice daily | ||
| Hydralazine | IV/IM (acute) | 5-10 mg IV/IM; repeat q 20-30 min | Widely used; vasodilator |
| Nifedipine | Oral (acute/chronic) | 30 mg once daily (slow-release) | CCB; good evidence of safety |
| Methyldopa | Oral (chronic) | 250 mg twice daily | Central α-agonist; FDA category B; first-line chronic |
Contraindicated: ACE inhibitors (e.g., enalapril), Angiotensin receptor blockers - unequivocal evidence of fetal harm (renal dysplasia, oligohydramnios, fetal/neonatal death).
C. Seizure Prophylaxis and Treatment - Magnesium Sulfate
Magnesium sulfate (MgSO₄) is the cornerstone of eclampsia prevention and treatment.
- Mechanism: NMDA receptor antagonism (not primarily antihypertensive)
- Has the advantage of maintaining uterine and fetal blood flow
- Indicated in: severe preeclampsia (prophylaxis), eclampsia (treatment), CNS symptoms (headache, visual disturbance, altered sensorium)
- Also consider postpartum if CNS symptoms develop (up to 48 hrs)
Protocol:
- Loading dose: 4-6 g IV over 15-20 minutes
- Maintenance: 2 g/hr IV infusion
Toxicity monitoring (Magnesium toxicity):
- Loss of deep tendon reflexes: ~10 mg/dL (earliest sign - check every 1-2 hours)
- Respiratory depression: ~12 mg/dL
- Cardiac arrest: >15 mg/dL
Antidote: Calcium gluconate 1 g IV (given slowly) reverses hypermagnesemia.
Stop infusion if: respiratory rate < 12/min or reflexes disappear.
D. Fluid Management
- Limit IV fluids to avoid pulmonary oedema (these patients have reduced oncotic pressure + increased capillary leak)
- Target urine output > 25 mL/hr
- Avoid diuretics and hyperosmotic agents routinely
- Use diuretics only for frank pulmonary oedema
E. Delivery
- Severe preeclampsia / eclampsia at any gestational age: deliver after stabilization
- Mild preeclampsia ≥37 weeks: deliver
- Mild preeclampsia <37 weeks: individualized management (hospitalization, close monitoring, aim for fetal maturity)
- HELLP syndrome: deliver promptly regardless of gestational age; early recognition is critical
Proteinuria and hypertension typically resolve within 1-2 weeks after delivery with no lasting sequelae in most cases. - Robbins Basic Pathology
F. Postpartum Considerations
- ~20% of eclamptic seizures occur >48 hours postpartum
- Continue MgSO₄ for 24-48 hours postpartum in eclampsia/severe preeclampsia
- BP ≥ 160/110 in postpartum period requires urgent antihypertensive therapy + obstetrics consultation
- Long-term: women with preeclampsia have increased lifetime risk of cardiovascular disease
9. Fetal Complications
- Intrauterine growth restriction (IUGR) - from chronic placental hypoperfusion
- Placental abruption
- Preterm birth (iatrogenic or spontaneous)
- Fetal distress / hypoxia
- Intrauterine death
10. Prevention
- Low-dose aspirin (75-150 mg/day from 12-16 weeks) in high-risk patients - reduces thromboxane/prostacyclin imbalance; shown to reduce risk
- Calcium supplementation in calcium-deficient populations
- Management of modifiable risk factors (obesity, diabetes, hypertension)
11. Prognosis
- Eclampsia (maternal death): now rare with modern management
- Leading causes of PIH-related maternal death:
- Intracranial hemorrhage (most common) - from undertreated severe hypertension
- Liver failure (HELLP)
- Pulmonary complications
- Recurrence risk: 20-50% in subsequent pregnancies depending on severity and gestational age of onset
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice - Chapters 45 & 47
- Guyton & Hall Textbook of Medical Physiology, p. 1041
- Robbins & Kumar Basic Pathology (Robbins Pathology), p. 702
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, p. 14
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Chapter 173
This is a shared conversation. Sign in to Orris to start your own chat.