ABGs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have everything needed for a thorough, well-cited ABG reference. Here is the complete guide:
Arterial Blood Gas (ABG) Interpretation
What an ABG Measures
An ABG directly measures pH, PaCO₂, and PaO₂, and calculates HCO₃⁻ from those values using the Henderson-Hasselbalch equation. Modern analyzers also often include lactate, hemoglobin, and electrolytes. It is the gold standard for assessing oxygenation, ventilation, and acid-base status.
- Murray & Nadel's Textbook of Respiratory Medicine
Normal Values
| Parameter | Normal Value | Range |
|---|---|---|
| pH | 7.40 | 7.35 - 7.45 |
| PaCO₂ | 40 mmHg | 38 - 42 mmHg |
| PaO₂ | 100 mmHg | 75 - 100 mmHg |
| HCO₃⁻ | 24 mEq/L | 22 - 26 mEq/L |
- Current Surgical Therapy, 14e
Stepwise Interpretation
Step 1 - Determine the Primary Process (pH)
- pH < 7.35 = Acidemia
- pH > 7.45 = Alkalemia
Step 2 - Identify Respiratory vs. Metabolic
| pH | PaCO₂ | Primary Disorder |
|---|---|---|
| ↓ | ↑ | Respiratory acidosis |
| ↓ | ↓ | Metabolic acidosis |
| ↑ | ↓ | Respiratory alkalosis |
| ↑ | ↑ | Metabolic alkalosis |
Step 3 - Assess Compensation
The body always compensates in the same direction as the primary disorder (i.e., respiratory compensation for metabolic and vice versa), but never over-compensates.
| Primary Disorder | Expected Compensation |
|---|---|
| Metabolic acidosis | PaCO₂ = 1.5 × [HCO₃⁻] + 8 ± 2 (Winter's formula) |
| Metabolic alkalosis | PaCO₂ = 0.7 × [HCO₃⁻] + 20 ± 5 |
| Acute respiratory acidosis | ↑ HCO₃⁻ by 1 mEq/L per 10 mmHg ↑ PaCO₂ |
| Chronic respiratory acidosis | ↑ HCO₃⁻ by 3.5-5 mEq/L per 10 mmHg ↑ PaCO₂ |
| Acute respiratory alkalosis | ↓ HCO₃⁻ by 2 mEq/L per 10 mmHg ↓ PaCO₂ |
| Chronic respiratory alkalosis | ↓ HCO₃⁻ by 4 mEq/L per 10 mmHg ↓ PaCO₂ |
If PaCO₂ is higher than expected in metabolic acidosis → concurrent respiratory acidosis. If lower → concurrent respiratory alkalosis.
- Barash Clinical Anesthesia 9e; Current Surgical Therapy 14e
Step 4 - Calculate the Anion Gap (AG)
AG = Na⁺ - (Cl⁻ + HCO₃⁻)
Normal AG < 12-13 mEq/L. Always correct for albumin:
Corrected AG = measured AG + 2.5 × (4 - albumin g/dL)
High-AG (MUDPILES):
- M - Methanol
- U - Uremia
- D - Diabetic ketoacidosis (also alcoholic / starvation ketoacidosis)
- P - Propylene glycol / Paracetamol (acetaminophen)
- I - Isoniazid / Iron
- L - Lactic acidosis (most common cause overall)
- E - Ethylene glycol
- S - Salicylates
An alternative modern mnemonic is GOLD MARK (Glycols, Oxoproline, L-lactate, D-lactate, Methanol, Aspirin, Renal failure, Ketoacidosis).
Normal-AG (hyperchloremic) acidosis - think GI bicarbonate loss (diarrhea) vs. renal loss (RTA).
Step 5 - Urine Anion Gap (if non-AG acidosis identified)
Urine AG = Urine (Na⁺ + K⁺ - Cl⁻)
- Negative urine AG → kidneys excreting NH₄⁺ appropriately → GI loss (diarrhea)
- Positive urine AG → impaired NH₄⁺ excretion → renal tubular acidosis (RTA)
Step 6 - Delta-Delta Ratio (ΔΔ) if AG elevated
ΔΔ = ΔAG / ΔHCO₃⁻ = (measured AG - 12) / (24 - measured HCO₃⁻)
| ΔΔ | Interpretation |
|---|---|
| < 1.0 | Mixed AG + non-AG metabolic acidosis |
| 1.0 - 2.0 | Pure AG metabolic acidosis |
| > 2.0 | AG metabolic acidosis + concurrent metabolic alkalosis (or chronic compensated respiratory acidosis) |
Step 7 - Evaluate PaO₂ / Oxygenation
Never overlook oxygenation. Calculate the A-a gradient:
- A-a gradient = PAO₂ - PaO₂
- PAO₂ = (FiO₂ × 713) - (PaCO₂ / 0.8)
- Normal ~10 mmHg (increases with age)
- Normal A-a gradient → pure hypoventilation (CNS, neuromuscular)
- Elevated A-a gradient → V/Q mismatch, diffusion impairment, shunt
Base Deficit
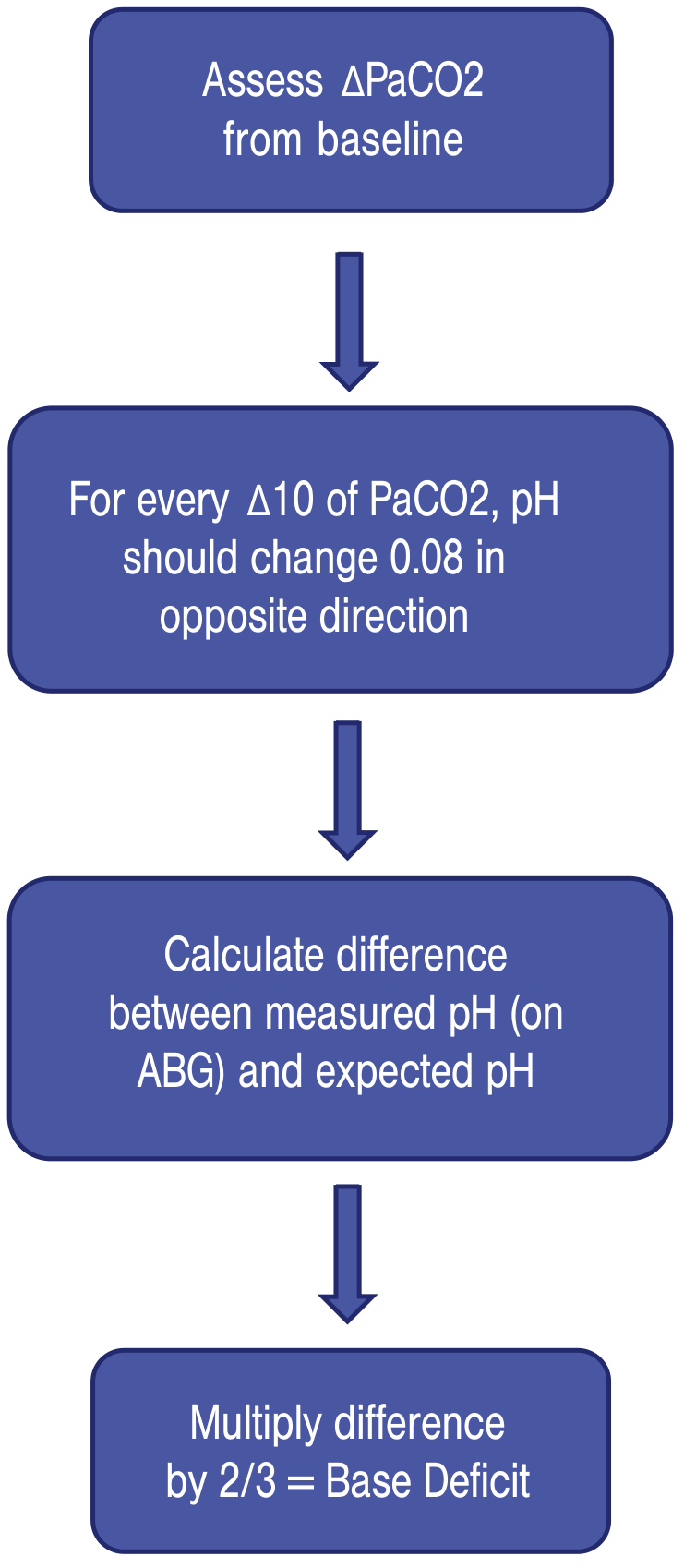
Base deficit is a derived value: for every Δ10 mmHg in PaCO₂, pH should change by 0.08 in the opposite direction. The difference between measured and expected pH, multiplied by 2/3, gives the base deficit. A practical shortcut: in metabolic acidosis, the expected PaCO₂ roughly equals the last two decimal digits of the pH (e.g., pH 7.23 → expected PaCO₂ ≈ 23 mmHg).
- Roberts and Hedges' Clinical Procedures in Emergency Medicine; Current Surgical Therapy 14e
Acute vs. Chronic Hypercapnia
| PaCO₂ | pH | HCO₃⁻ | |
|---|---|---|---|
| Acute respiratory acidosis | > 45 | < 7.35 | ↑ ~1 per 10 mmHg ↑CO₂ |
| Chronic respiratory acidosis | > 45 | Normal or near-normal | ↑ 3.5-5 per 10 mmHg ↑CO₂ |
Renal compensation takes 3-5 days to reach steady state, so acute-on-chronic hypercapnia shows intermediate values.
- Murray & Nadel's Textbook of Respiratory Medicine
Venous vs. Arterial
Arterial blood is the reference standard. However, in clinical practice:
- Venous pH correlates closely with arterial (difference ±0.05) - useful for pH trending
- Venous PaCO₂ trends with arterial but can vary ±20 mmHg
- Venous PO₂ cannot substitute for arterial PO₂ - the values do not correlate
A normal venous PaCO₂ is predictive of a normal arterial PaCO₂ (useful to rule out hypercapnia). Mildly elevated venous lactate should be confirmed with an arterial sample when clinically important.
- Tintinalli's Emergency Medicine
Quick Summary Mnemonics
- ROME: Respiratory Opposite, Metabolic Equal (pH and the primary parameter move in the same direction in metabolic disorders, opposite in respiratory)
- Winter's formula: PaCO₂ = 1.5 × HCO₃⁻ + 8 ± 2 (expected respiratory compensation for metabolic acidosis)
- MUDPILES / GOLD MARK: causes of high-anion-gap metabolic acidosis
This is a shared conversation. Sign in to Orris to start your own chat.