Ecg
Asking for Preferences
Reading File
Finding Sources
Searching Images
ECG electrocardiogram basic components waves intervals
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
Now I have comprehensive material from the textbooks. Let me compile a thorough guide.
ECG: Basic Principles & How to Read One
Sources: Goldman-Cecil Medicine, Costanzo Physiology, Harrison's Principles of Internal Medicine
What Is an ECG?
An ECG (electrocardiogram) measures tiny voltage differences on the body surface caused by the timing and sequence of cardiac depolarization and repolarization. Because the heart depolarizes in a specific sequence — atria first, then ventricles — potential differences are detectable from skin electrodes.
The Cardiac Conduction Sequence
The electrical wave originates in the sinoatrial (SA) node (right atrium near the superior vena cava) → spreads through both atria via the Bachmann bundle → slows physiologically at the AV node → exits into the Bundle of His → divides into right and left bundle branches (left splits into anterior and posterior fascicles) → activates ventricular muscle via the Purkinje system.
ECG Waveforms, Intervals & Segments
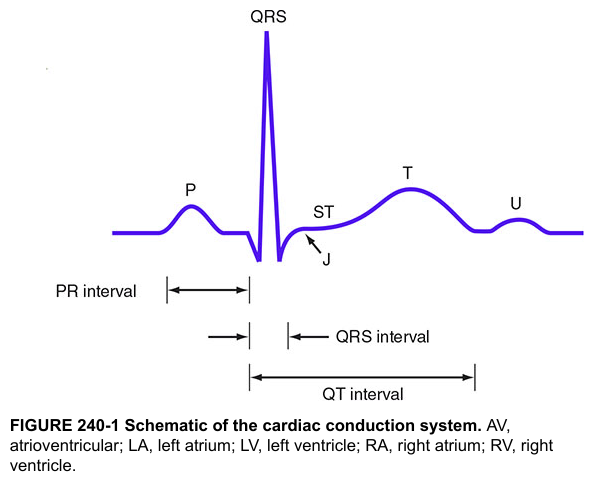

| Component | Represents | Normal Value |
|---|---|---|
| P wave | Atrial depolarization | Duration < 120 ms |
| PR interval | Onset of atrial depol → onset of ventricular depol (includes AV node delay) | 90–200 ms |
| QRS complex | Ventricular depolarization (Q = first negative, R = first positive, S = second negative deflection) | 75–110 ms |
| ST segment | Early ventricular repolarization (isoelectric normally) | At baseline |
| T wave | Ventricular repolarization | Upright in most leads |
| QT interval | QRS onset → T wave end (total ventricular depolarization + repolarization) | QTc ≤ 450 ms ♂, ≤ 460 ms ♀ |
| U wave | Small deflection after T wave (sometimes seen; mechanism debated) | Not always visible |
Key distinction: Intervals include waves; segments do not. Atrial repolarization is not visible because it is buried within the QRS complex.
The ventricular depolarizes as quickly as the atria (similar QRS and P durations) because the His-Purkinje system conducts far faster than atrial tissue.
The ECG Paper & Calibration
- Standard speed: 25 mm/sec
- 1 small box (1 mm) = 0.04 sec (40 ms)
- 1 large box (5 mm) = 0.20 sec (200 ms)
- Voltage: 10 mm = 1 mV
- A standard ECG records 10 seconds total; each lead group (I, II, III / aVR, aVL, aVF / V1–3 / V4–6) records for 2.5 sec simultaneously
The 12 Leads
A standard ECG uses 10 electrodes to generate 12 vantage points:
Limb leads (frontal plane)
- Bipolar: I, II, III
- Lead I: right arm (−) vs. left arm (+)
- Lead II: right arm (−) vs. left leg (+)
- Lead III: left arm (−) vs. left leg (+)
- Augmented unipolar: aVR, aVL, aVF
- aVR looks at the heart from the right shoulder; P and QRS are normally inverted
- aVL from left shoulder; aVF from feet
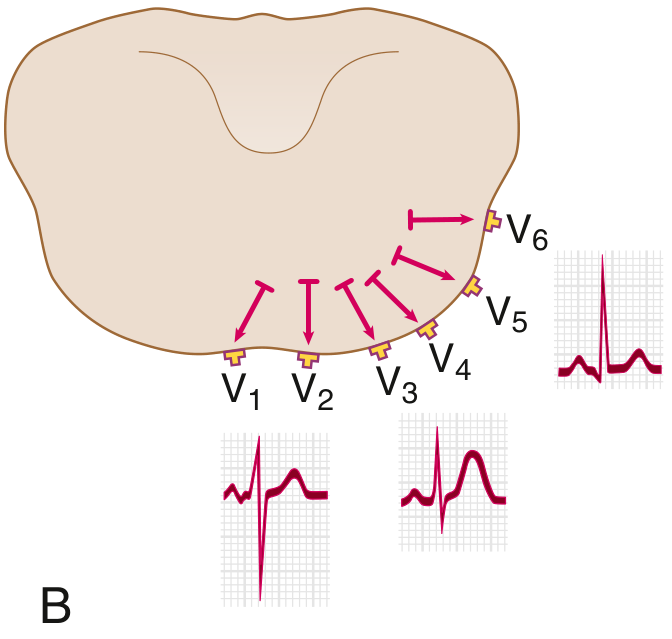
Precordial leads (horizontal plane)
- V1–V6 placed on the chest wall; V1 is rightmost (rS pattern), V6 is leftmost (tall R)
- Normal R-wave progression: R grows from V1→V6; transition (R:S = 1:1) occurs at V3–V4
Calculating Heart Rate
$$HR = \frac{60{,}000}{\text{RR interval (ms)}}$$
Quick method (regular rhythm): count big boxes between two R waves:
- 1 box → 300 bpm
- 2 boxes → 150 bpm
- 3 boxes → 100 bpm
- 4 boxes → 75 bpm
- 5 boxes → 60 bpm
For irregular rhythms (e.g., atrial fibrillation): multiply total beats on a 10-second strip × 6.
Normal resting rate: 50–100 bpm (physiologically 50–90 bpm may better represent normal)
Normal QRS Axis
- The QRS axis reflects the dominant direction of ventricular depolarization in the frontal plane
- Normal: −30° to +90°
- Left axis deviation (LAD): −30° to −90°
- Right axis deviation (RAD): +90° to +180°
Quick estimate: If QRS is upright in both leads I and II, axis is normal. If upright in I but negative in II → LAD. If negative in I → RAD.
Stepwise Approach to Reading an ECG
(Table 42-2, Goldman-Cecil Medicine)
- Rate — calculate from RR interval
- Rhythm — regular vs. irregular?
- P waves — present? Before every QRS? Upright in II?
- PR interval — normal (90–200 ms)? Fixed or varying?
- QRS duration — narrow (< 120 ms) or wide (≥ 120 ms)?
- QRS axis — normal, LAD, RAD?
- QRS morphology — R-wave progression in precordial leads; bundle branch block pattern?
- ST segments — elevated, depressed, or at baseline? (regional groupings: inferior II/III/aVF, anterior V1–V4, lateral I/aVL/V5–V6)
- T waves — upright, inverted, peaked?
- QT/QTc — prolonged?
Normal Values Summary
| Parameter | Normal |
|---|---|
| Heart rate | 50–100 bpm |
| P wave duration | < 120 ms |
| PR interval | 90–200 ms |
| QRS duration | 75–110 ms |
| QTc | ≤ 450 ms (♂), ≤ 460 ms (♀) |
| QRS axis | −30° to +90° |
What Abnormalities Look Like (Brief Overview)
| Finding | Common Causes |
|---|---|
| Wide QRS (≥ 120 ms) | Bundle branch block, hyperkalemia, pre-excitation (WPW) |
| Long PR (> 200 ms) | First-degree AV block, AV nodal disease |
| ST elevation | MI (STEMI), pericarditis |
| ST depression | Ischemia, subendocardial infarction |
| Peaked T waves | Hyperkalemia |
| Prolonged QTc | Drugs, hypokalemia, hypomagnesemia, congenital long QT |
| P wave absent | Atrial fibrillation, junctional rhythm |
| Delta wave (slurred QRS upstroke) | Wolff-Parkinson-White syndrome |
Want to go deeper on any part of this — axis calculation, a specific lead group, arrhythmia recognition, or bundle branch blocks?
This is a shared conversation. Sign in to Orris to start your own chat.