Knock knees
Reading File
Finding Sources
Searching the Web
knock knees genu valgum causes management treatment
Finding Sources
Searching PubMed
genu valgum knock knee treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Loading Image
Finding Sources
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer. Let me compile it.
Knock Knees (Genu Valgum)
Knock knees, or genu valgum, is a lower limb alignment deformity in which the knees angle inward (medially) while the feet and ankles remain apart. The term "knock knee" describes how the knees "knock" together during walking.
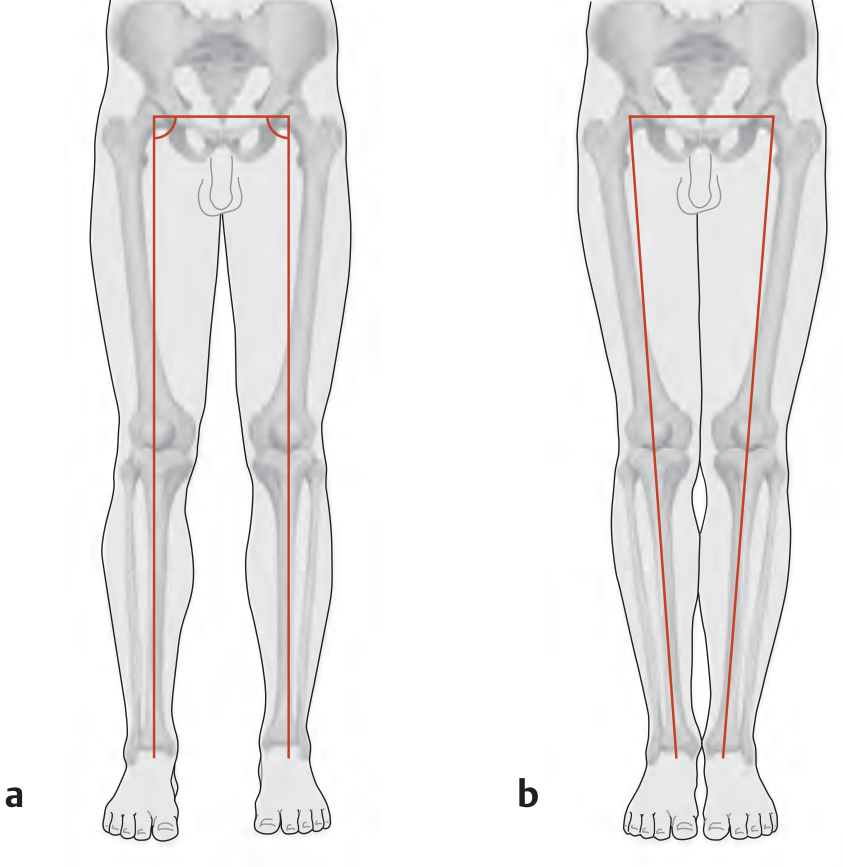
Left (a): normal alignment with the mechanical axis passing through the center of the knee. Right (b): genu valgum - knees deviate medially relative to the mechanical axis.
Definition and Anatomy
In genu valgum, the center of the knee joint lies medial to the mechanical axis (the line from the center of the femoral head to the center of the ankle). This causes unbalanced loading on the knee joint - specifically overloading the lateral compartment and placing abnormal tension on the medial structures. Over time, this asymmetric load leads to lateral compartment osteoarthritis and stretching of medial ligaments.
The femorotibial angle normally measures about 174° in the coronal plane. In genu valgum, this angle increases (more valgus). - General Anatomy and Musculoskeletal System (Thieme Atlas), p. 431
Measurement
The intermalleolar distance is the standard clinical measure:
- With the medial sides of the knees touching, measure the gap between the medial malleoli
- >5 cm intermalleolar distance is considered abnormal
- An intercondylar distance >3 cm (with feet together) indicates genu varum by comparison
"In case of genu valgum or knock knee, the degree of deformity can be estimated by the intermalleolar separation present when the inner sides of the knees are kept in apposition." - S Das Manual on Clinical Surgery, p. (examination section)
Physiological vs Pathological
Physiological (Normal Developmental)
-
Up to 10° of genu valgum is normal in children up to 2 years of age
-
Maximum valgus is typically seen between ages 3-4 years
-
Up to 15° at the knee is common in children aged 2-6 years
-
Spontaneous correction to straight legs occurs by school age (around 7 years)
-
Cases within the physiologic range do NOT require treatment
-
Miller's Review of Orthopaedics 9th Edition, p. 278
Pathological
Knock knees that persist beyond age 6, are severe (>15° or intermalleolar gap >10 cm), or are unilateral warrant further evaluation.
Causes
| Category | Examples |
|---|---|
| Physiological | Normal developmental variant (ages 2-6) |
| Metabolic bone disease | Rickets, renal osteodystrophy (most common pathological bilateral cause), endemic fluorosis |
| Skeletal dysplasias | Dwarfism (disproportionate short trunk type), Morquio syndrome, osteochondromas |
| Connective tissue | Osteogenesis imperfecta (repeated fractures), ligamentous laxity |
| Trauma/Infection | Proximal tibial fractures (Cozen phenomenon), infections stimulating asymmetric physeal growth |
| Degenerative | Lateral compartment OA (loss of lateral articular cartilage leads to secondary valgus) |
| Syndromic | Proteus syndrome, neurodevelopmental disorders with rickets |
| Hormonal | Klinefelter syndrome (tendency to genu valgum due to tall stature and ligamentous laxity) |
Clinical Features
- Knees touch/knock together while walking and standing
- Ankles remain spaced apart when knees are together
- Awkward or waddling gait
- Difficulty standing with feet together
- Knee pain (lateral compartment) in pathological cases
- In children: may coincide with flat feet (pes planus)
- Associated femoral anteversion and external tibial torsion can worsen the apparent deformity
Investigations
- Standing AP radiograph of lower limbs (full-length) - to measure the mechanical and anatomical axes and femorotibial angle
- Weight-bearing PA knee X-ray in adults to evaluate joint space (lateral compartment narrowing)
- Blood work if metabolic cause suspected: calcium, phosphate, ALP, PTH, vitamin D, renal function
- Urine keratan sulfate if Morquio syndrome suspected
Treatment
Conservative
- Observation for physiological genu valgum (2-6 years of age) - resolves spontaneously
- Treat underlying metabolic cause (e.g., vitamin D supplementation for rickets)
- Conservative treatment is ineffective in pathological genu valgum - braces (e.g., used in osteogenesis imperfecta) are cumbersome and may promote ligamentous laxity
Surgical - Indications
Surgery is considered when:
- Child is older than 10 years AND
- Intermalleolar distance >10 cm OR valgus angulation >15°
- Significant patellar instability secondary to genu valgum
- Rapidly progressive deformity
Surgical Options
| Option | Principle | Best For |
|---|---|---|
| Hemiepiphysiodesis (guided growth) | Temporary compression of medial distal femoral physis (Heuter-Volkmann law: compression inhibits growth) | Children with open physes; gradual correction by differential growth |
| Stapling / 8-plate | Hardware placed across medial physis to retard medial growth | Skeletally immature patients |
| Osteotomy | Bone cut at the site of deformity to realign mechanical axis | Skeletally mature patients; severe/fixed deformities |
| Distal femoral osteotomy | Corrects femoral component of valgus | Adults; also used for recurrent patellar instability in genu valgum (Moran et al., 2024) |
Guided growth (hemiepiphysiodesis) relies on the Heuter-Volkmann principle that growth is inhibited by increased compression, and returns to normal once the hardware is removed. - Miller's Review of Orthopaedics 9th Edition
A 2025 systematic review (Hong & Loh, PMID 40966823) confirms guided growth is effective for pediatric knee alignment correction.
Complications of Untreated Genu Valgum
- Lateral compartment knee osteoarthritis
- Patellar instability and patellofemoral pain
- Abnormal gait biomechanics
- Medial ligament and capsule stretching
- Compensatory foot deformities (fallen pedal arch)
Key Points Summary
| Feature | Detail |
|---|---|
| Definition | Knees deviate medially; mechanical axis passes medial to knee center |
| Measurement | Intermalleolar distance (>5 cm abnormal) |
| Physiological age | 2-6 years, peaks at 3-4 years, resolves by age 7 |
| Most common pathological cause (bilateral) | Renal osteodystrophy |
| Surgical threshold | >10 years old, >15° valgus, or >10 cm intermalleolar gap |
| Preferred surgery in growing children | Guided growth hemiepiphysiodesis |
| Preferred in skeletally mature | Osteotomy at site of deformity |
Cozens test
Reading File
Finding Sources
Searching the Web
Cozen's test lateral epicondylitis tennis elbow clinical examination procedure
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I have comprehensive information. Here is the full answer.
Cozen's Test (for Lateral Epicondylitis / Tennis Elbow)
What It Tests
Cozen's test is a provocative clinical examination used to diagnose lateral epicondylitis (tennis elbow) - a painful degenerative tendinopathy at the origin of the extensor carpi radialis brevis (ECRB) at the lateral epicondyle of the humerus.
Technique
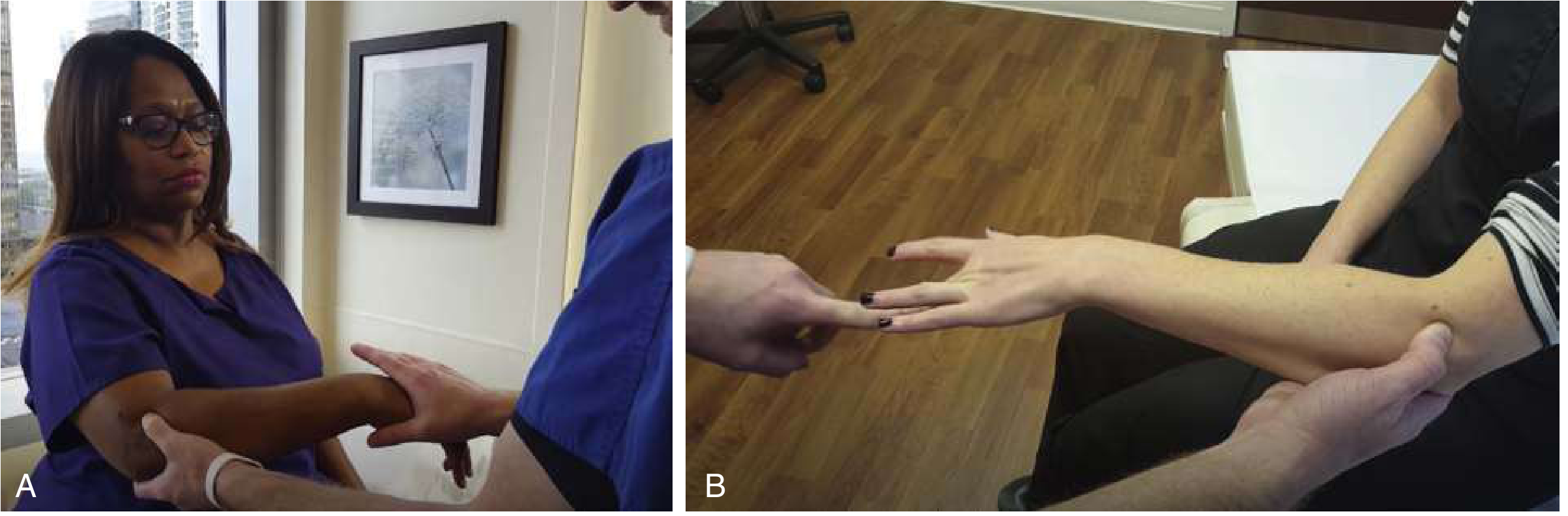
(A) Cozen's test - examiner grasps and stabilizes the forearm while resisting wrist extension. (B) Maudsley's test shown alongside for comparison.
Step-by-step procedure:
- The examiner stabilizes the patient's elbow with one hand, with the thumb palpating/pressing over the lateral epicondyle
- The patient makes a clenched fist and pronates the forearm
- The patient then radially deviates and actively extends the wrist against resistance applied by the examiner's other hand
- The elbow is kept in slight flexion or full extension depending on variation
Positive test: Reproduction of sharp pain at the lateral epicondyle (where the common extensor tendons originate)
- Rosen's Emergency Medicine, p. 2349
- S Das Manual on Clinical Surgery, p. 235
Clinical Image (from S Das Manual)
Anatomical Basis
The test stresses the extensor carpi radialis brevis (ECRB) tendon at its origin on the lateral epicondyle. In lateral epicondylitis, histologic examination reveals angiofibroblastic hyperplasia (degenerative tendinopathy, not true inflammation despite the "-itis" name). The wrist extension and radial deviation against resistance maximally load this tendon origin, provoking pain. - Miller's Review of Orthopaedics 9th Ed
Diagnostic Accuracy
| Metric | Value |
|---|---|
| Sensitivity | ~74% |
| Specificity | Poor (low) |
| Clinical utility | Best used as part of a cluster of tests, not in isolation |
Because of its poor specificity, Cozen's test should not be used alone - a positive result must be interpreted alongside history, tenderness to palpation just distal to the lateral epicondyle, and other tests. - Rosen's Emergency Medicine, p. 2349
Comparison with Related Tests
| Test | Maneuver | Structures stressed |
|---|---|---|
| Cozen's | Resisted wrist extension + radial deviation with clenched fist | ECRB origin at lateral epicondyle |
| Maudsley's test | Active extension of the middle finger (3rd digit) against resistance, elbow extended | ECRB (via extensor digitorum communis) |
| Mill's manoeuvre | Passive wrist flexion with forearm pronated | Common extensor tendon stretched passively |
All three reproduce pain at the lateral epicondyle when positive for lateral epicondylitis.
"Mill's manoeuvre i.e. the patient's wrist is passively flexed when his forearm is pronated. This gives rise to tremendous pain on the attachment of the common extensor tendons." - S Das Manual on Clinical Surgery, p. 235
Context: Lateral Epicondylitis (Tennis Elbow)
- Affects the ECRB origin at the lateral epicondyle
- Despite the name, <5% of patients actually play tennis - more common in workers doing repetitive wrist extension (screwdrivers, wrenches, assembly line)
- Prevalence in the workforce: up to 14.5%
- Symptoms: dull ache along the lateral elbow, worsened by grasping, twisting, turning door handles, or pouring
- Tenderness just distal to the lateral epicondyle over the ECRB origin is the most reliable finding on palpation
- Treatment: conservative first (rest, NSAIDs, physiotherapy, counterforce bracing); corticosteroid injections have no clear long-term benefit; surgery (open or arthroscopic debridement) for recalcitrant cases - Miller's Review of Orthopaedics 9th Ed
Note on the "Cozen Phenomenon" (Different Context)
The term "Cozen" also appears in orthopaedics in a different context: the Cozen phenomenon refers to progressive valgus deformity (knock knee) following a proximal tibial fracture in children - this is a separate entity and should not be confused with Cozen's test for tennis elbow. - Campbell's Operative Orthopaedics 15th Ed 2026
This is a shared conversation. Sign in to Orris to start your own chat.