Management of SLE and SLE arthritis and anemia
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"systemic lupus erythematosus"[MeSH Terms] AND "management"[MeSH Terms]
Finding Sources
Searching PubMed
"lupus erythematosus" AND treatment
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
I now have comprehensive information from Harrison's 22E (2025). I have enough material to write a thorough, well-structured answer. Let me compile the full response.
Management of Systemic Lupus Erythematosus (SLE), SLE Arthritis, and SLE Anemia
Primary source: Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Overview
SLE is an autoimmune disease in which dysregulated innate and adaptive immunity causes tissue damage via autoantibodies and immune complexes. It affects women (~90% of cases) predominantly of childbearing age. Management is organ-system based, stratified by disease severity, and always anchored on two universal pillars: hydroxychloroquine (HCQ) and glucocorticoid minimization.
I. General/Non-Pharmacological Measures (All Patients)
All SLE patients should be counseled on:
- Daily sunscreen on sun-exposed areas
- Regular exercise and maintaining normal body weight
- Smoking cessation (tobacco reduces antimalarial efficacy)
- Balanced diet
- Up-to-date vaccinations
- Blood pressure, lipid, and glucose control
- Low-dose aspirin in antiphospholipid antibody (aPL)-positive patients
Treatment targets:
- Remission: Clinical SLEDAI = 0, on HCQ, prednisone ≤5 mg/day
- Low disease activity state (LLDAS): SLEDAI ≤4, HCQ, prednisone ≤5 mg/day, immunosuppressives at stable tolerated dose
II. Universal Therapy: Hydroxychloroquine (HCQ)
HCQ is first-line for all SLE patients unless contraindicated. Its benefits are extensive:
- Reduces disease flares
- Improves overall survival
- Decreases risk of renal disease and accelerated atherosclerosis
- Reduces flares during pregnancy
- Most useful drug for fatigue in SLE
- Safe in pregnancy and breastfeeding
Dosing: Up to 5 mg/kg/day (actual body weight). Baseline retinal exam and annual monitoring for maculopathy (risk increases with higher dose and longer duration, but remains low overall). Risk of retinopathy <1% at ≤5 years, <2% at 10 years at recommended doses.
Alternative antimalarials: chloroquine (higher retinal toxicity risk), quinacrine.
Tobacco use interferes with antimalarial efficacy.
III. Treatment of Non-Renal SLE (By Severity)
The figure below from Harrison's 22E (EULAR 2023 recommendations) illustrates the tiered approach:
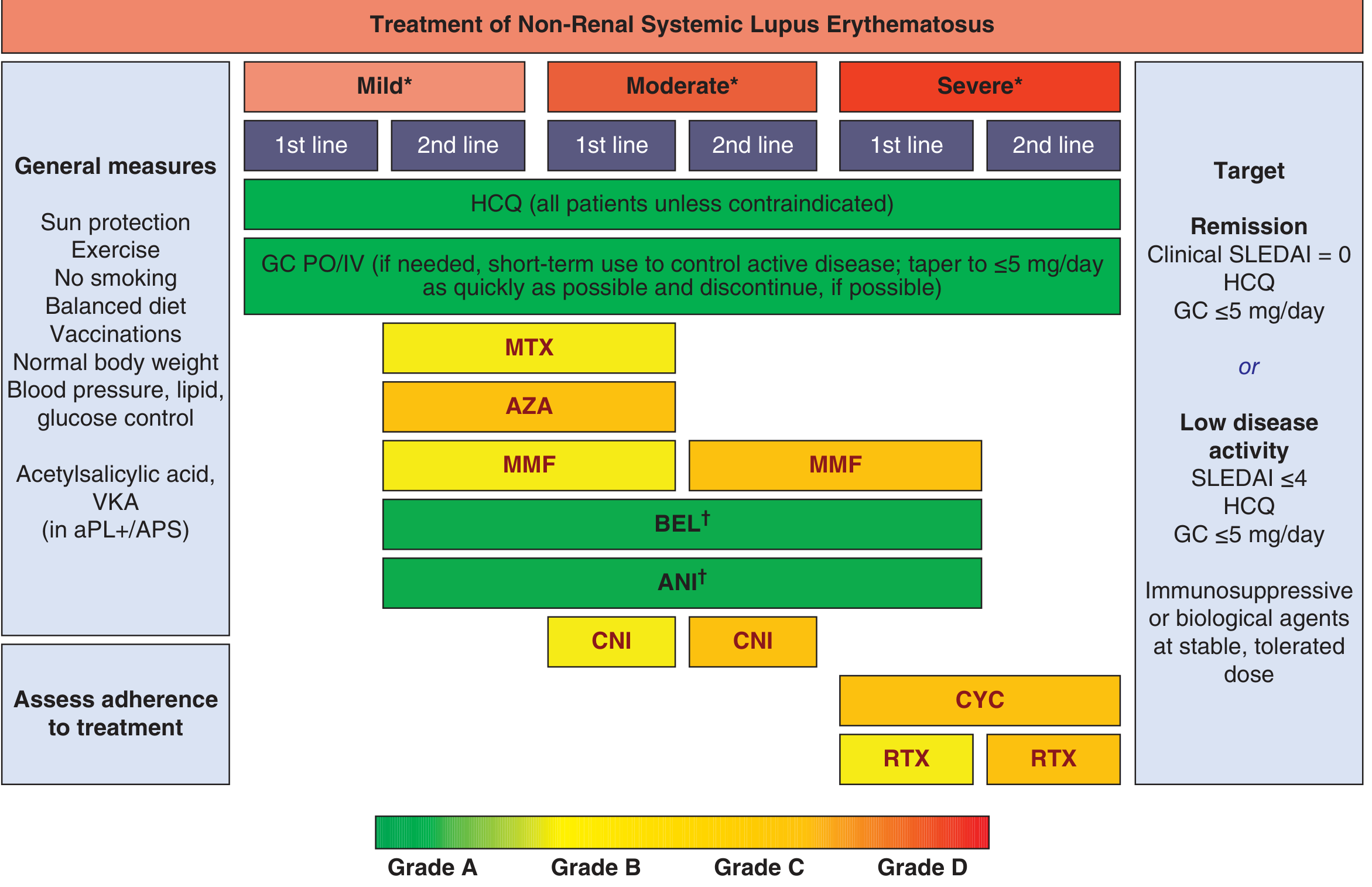
Disease Severity Definitions:
| Severity | Criteria |
|---|---|
| Mild | Constitutional symptoms; mild arthritis; rash <9% BSA; PLT 50-100 × 10⁹/L; SLEDAI ≤6; BILAG C or ≤1 BILAG B |
| Moderate | Moderate-severe arthritis; rash 9-18% BSA; PLT 20-50 × 10⁹/L; serositis; SLEDAI 7-12; ≥2 BILAG B |
| Severe | Major organ-threatening disease (cerebritis, myelitis, pneumonitis, mesenteric vasculitis); PLT <20 × 10⁹/L; TTP-like; rash >18% BSA; SLEDAI >12; ≥1 BILAG A |
Drug Summary by Tier
| Severity | 1st Line | 2nd Line |
|---|---|---|
| All | HCQ + short-term GC (taper to ≤5 mg/day as quickly as possible) | - |
| Mild | MTX or AZA | MMF, BEL, ANI |
| Moderate | MMF, BEL, or ANI | CNI |
| Severe | CYC or RTX | RTX, CYC |
Key drugs:
- MTX (methotrexate): arthritis and skin; folinic acid antagonist
- AZA (azathioprine): skin, arthritis; screen TPMT gene before use
- MMF (mycophenolate mofetil): skin, joints, nephritis; purine synthesis inhibitor
- BEL (belimumab): anti-BAFF biologic; IV or SC; FDA-approved; improves glucocorticoid-sparing
- ANI (anifrolumab): anti-type I IFN receptor; FDA-approved; especially for severe skin disease; NOT for severe neuropsychiatric SLE
- CYC (cyclophosphamide): alkylating agent; IV for severe/organ-threatening disease
- RTX (rituximab): anti-CD20; used in refractory disease
IV. SLE Arthritis - Specific Management
Musculoskeletal involvement (arthralgia, myalgia, polyarthritis, Jaccoud deformity) is among the most common SLE manifestations.
Step-wise approach:
- HCQ - first-line for all SLE arthritis; highly effective for mild-to-moderate joint disease
- NSAIDs - adjunctive for pain and inflammation in mild disease; use cautiously (renal/CV risk in SLE)
- Short-course glucocorticoids (oral or IM) - for flares; minimize duration and taper quickly to ≤5 mg/day prednisone or discontinue
- Methotrexate (MTX) - particularly effective for arthritis; 7.5-15 mg/week orally; leflunomide is an alternative
- Azathioprine (AZA) - especially if concomitant skin or hematologic disease
- MMF - equal option to MTX/AZA for moderate disease
- Belimumab or anifrolumab - for persistent moderate-to-severe arthritis despite above
Note: MTX, AZA, and MMF are considered equal options for second-line therapy in mild disease and first-line for moderate disease. Ordering does not imply preference.
For severe RA-like arthritis (joint destruction), the approach escalates similarly to RA therapy. Jaccoud deformity (non-erosive) is characteristic of SLE and reflects tendon/capsular laxity rather than true erosions.
V. SLE Anemia - Classification and Management
Anemia is the most common hematologic manifestation of SLE, present in >50% of patients.
Types of Anemia in SLE
| Type | Mechanism | Frequency/Notes |
|---|---|---|
| Anemia of chronic disease | Inflammatory cytokine-mediated iron sequestration; normocytic, normochromic | ~1/3 of SLE anemia cases |
| Iron deficiency anemia | Blood loss, poor intake, GI involvement | Microcytic, hypochromic |
| Autoimmune hemolytic anemia (AIHA) | Warm IgG anti-RBC antibodies; Coombs-positive | Direct antiglobulin test (DAT) positive |
| Aplastic anemia | Immune suppression of marrow | Rare, pancytopenia |
| Microangiopathic hemolytic anemia (MAHA) | Thrombotic microangiopathy/atypical HUS | Schistocytes on smear, elevated LDH, low ADAMTS13 |
| Medication effect | Azathioprine, mycophenolate, others | Check timing with new drugs |
Hematologic Cytopenias Beyond Anemia
- Leukopenia (<4000/µL): Common (~50% of SLE patients); usually lymphopenia (<1500/µL) rather than neutropenia
- Thrombocytopenia (<150,000/µL): Usually mild, immune-mediated; can be severe (<50,000/µL); associated with APS/aPL antibodies
Treatment of SLE Anemia and Cytopenias
Anemia of chronic disease:
- Control the underlying SLE disease activity with HCQ + immunosuppressives
- Iron supplementation only if true concurrent iron deficiency documented
Autoimmune hemolytic anemia (AIHA):
- Glucocorticoids - prednisone 1 mg/kg/day; first-line
- Anti-CD20 agents (rituximab) - indicated for lupus-related AIHA and severe thrombocytopenia; FDA-recognized use
- Azathioprine or MMF - steroid-sparing maintenance
- IVIG (intravenous immunoglobulin) - for acute, severe hemolysis or thrombocytopenia
- Splenectomy - reserved for refractory cases
Severe thrombocytopenia (<50,000/µL):
- Glucocorticoids + IVIG (for acute bleeding risk)
- Rituximab for refractory disease
- Platelet growth factors (TPO-RA) for resistant cases
- Splenectomy in resistant cases
Atypical HUS / MAHA:
- Plasmapheresis + high-dose glucocorticoids (potentially lifesaving)
- Rituximab and the C5 inhibitor eculizumab in refractory atypical HUS
VI. Lupus Nephritis Management
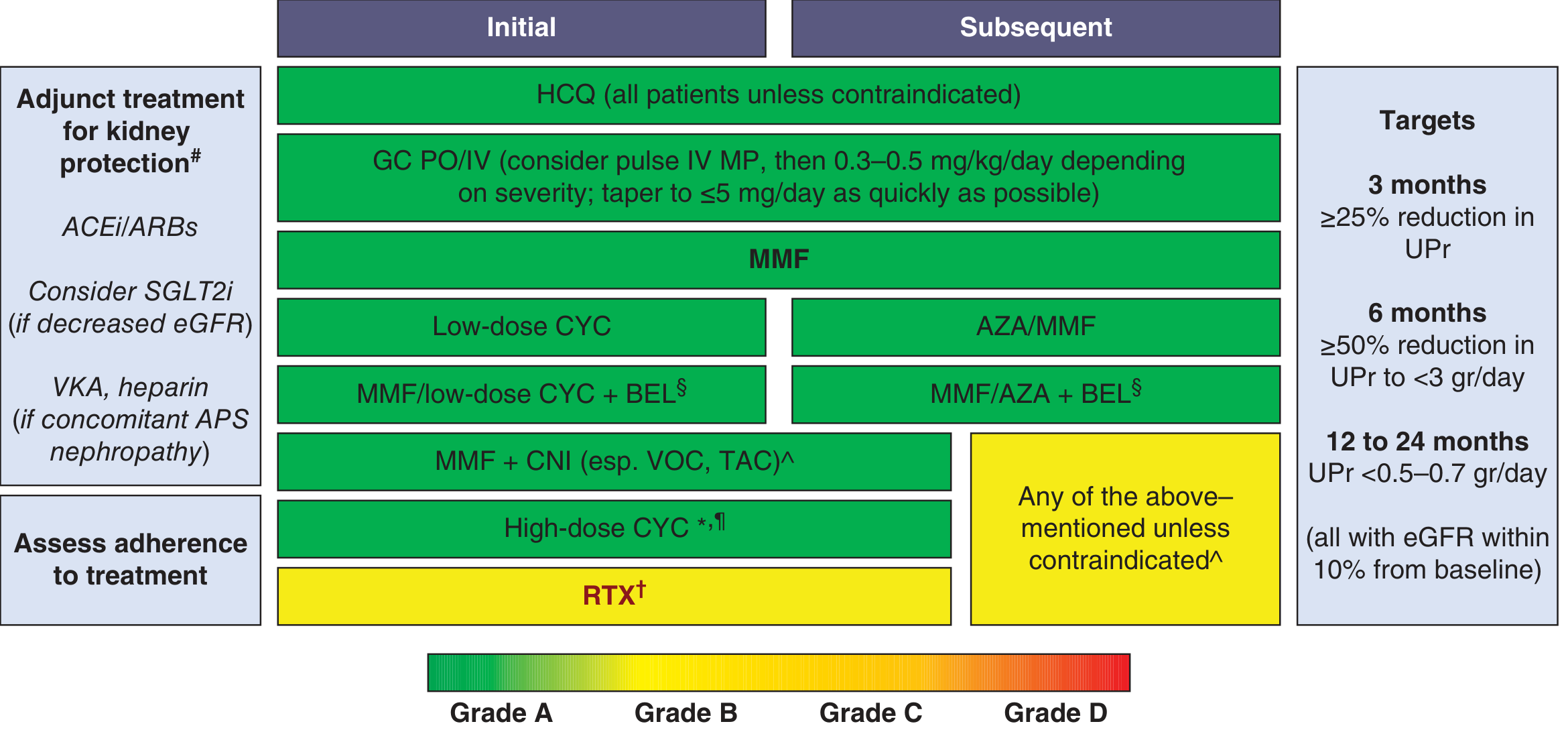
Key points for class III/IV nephritis:
- Initial: MMF (preferred in Black/Hispanic patients) OR low-dose cyclophosphamide + glucocorticoids
- Add-on options: Belimumab (approved 2020) or voclosporin (approved 2021) as triple therapy with MMF + GC
- Maintenance: MMF preferred over AZA for preserving renal function; AZA preferred in pregnancy
- Adjuncts: ACEi/ARB for all class III/IV/V nephritis; SGLT2i if decreased eGFR
- Targets: ≥25% reduction in UPCR at 3 months; ≥50% reduction to <3 g/day at 6 months; <0.5-0.7 g/day at 12-24 months
VII. Pregnancy Considerations
- HCQ: safe and standard of care for all SLE pregnancies; reduces flares
- AZA and tacrolimus: safe in pregnancy
- MMF and MTX: teratogenic - avoid
- Belimumab, anifrolumab, voclosporin: avoid (insufficient safety data)
- Low-dose aspirin: for preeclampsia prevention
- LMWH: for APS-related pregnancy morbidity
VIII. Emerging Therapies (2025)
- Obinutuzumab (anti-CD20 mAb): phase 3 data for lupus nephritis; also being studied in non-renal SLE
- SGLT2 inhibitors: being studied for nephroprotective effects in lupus nephritis
- Iberdomide / KZR-616: novel small molecules targeting immune pathways in trials
- CAR-T therapy targeting autoreactive B and T cells: early-phase trials showing remission in refractory SLE
Recent Evidence (EULAR 2023 Update)
The 2024 EULAR systematic literature review informing the 2023 recommendations (Kostopoulou et al., Ann Rheum Dis 2024, PMID 38777375) confirmed treat-to-target strategies targeting LLDAS or remission. The EULAR non-pharmacological management guidelines (Parodis et al., Ann Rheum Dis 2024, PMID 37433575) emphasize lifestyle, vaccination, CV risk reduction, and patient education.
Sources: Harrison's Principles of Internal Medicine, 22nd Edition (2025), pp. 2871-2880; EULAR 2023 SLE Recommendations (Fanouriakis et al., Ann Rheum Dis 83:15, 2024).
This is a shared conversation. Sign in to Orris to start your own chat.