Spina ventosa etiology pathology signs and symptoms investigation and treatment explain in detail with appropriate illustrative diagrams
spina ventosa tuberculous dactylitis etiology pathology signs symptoms treatment
https://openorthopaedicsjournal.com/VOLUME/6/PAGE/118/FULLTE…
spina ventosa tuberculous dactylitis
https://e-century.us/files/ajtr/16/8/ajtr0155687.pdf
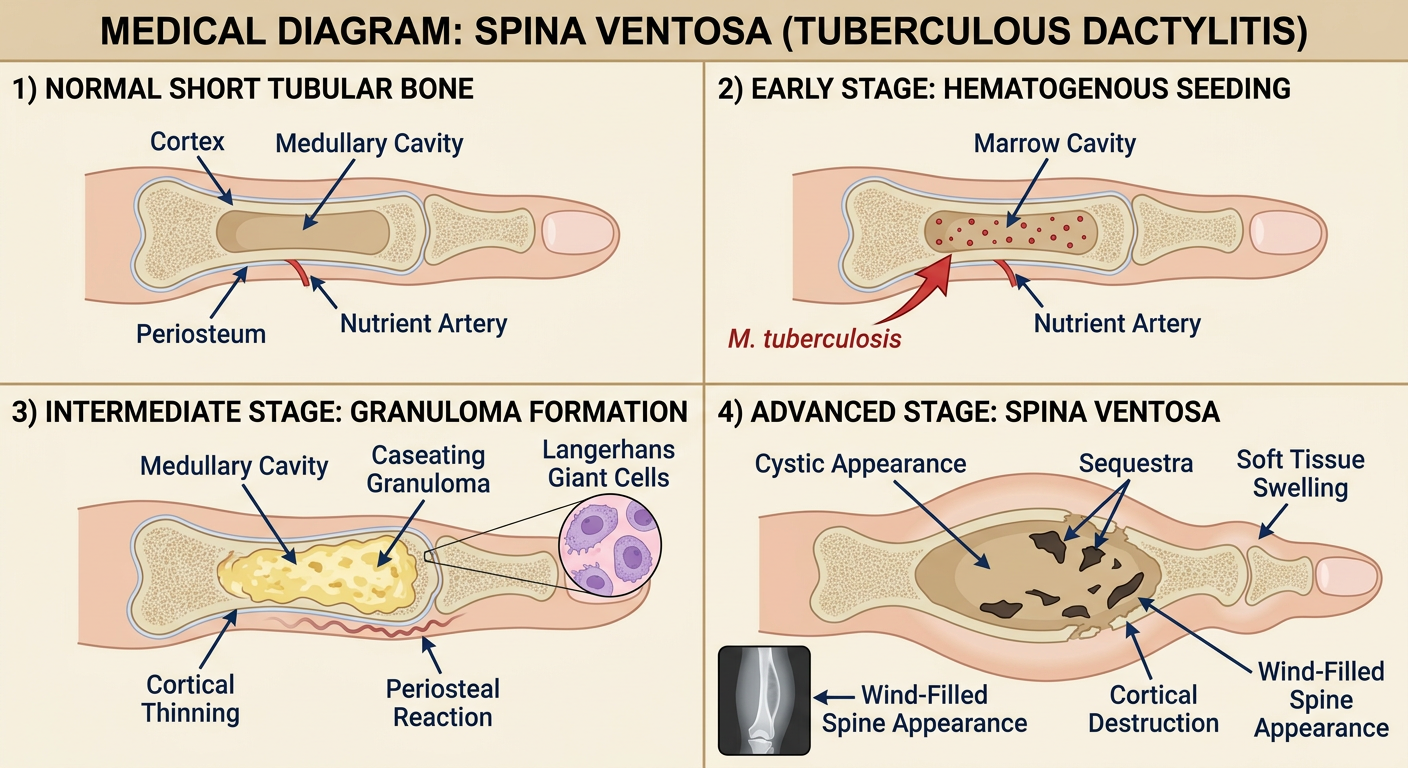
Medical diagram of Spina Ventosa (tuberculous dactylitis) showing: 1) Normal short tubular bone of hand with labeled parts (cortex, medullary cavity, periosteum, nutrient artery), 2) Early stage: hematogenous seeding of Mycobacterium tuberculosis lodging in center of marrow cavity via large nutrient artery, 3) Intermediate stage: formation of caseating tuberculous granuloma with Langerhans giant cells expanding the medullary cavity, cortical thinning, periosteal reaction beginning, 4) Advanced stage: classic spindle-shaped expansion of bone with cystic appearance (spina ventosa), sequestra, cortical destruction, soft tissue swelling creating "wind-filled spine" appearance on X-ray. Clean labeled anatomical cross-section style diagram with annotations, educational medical illustration
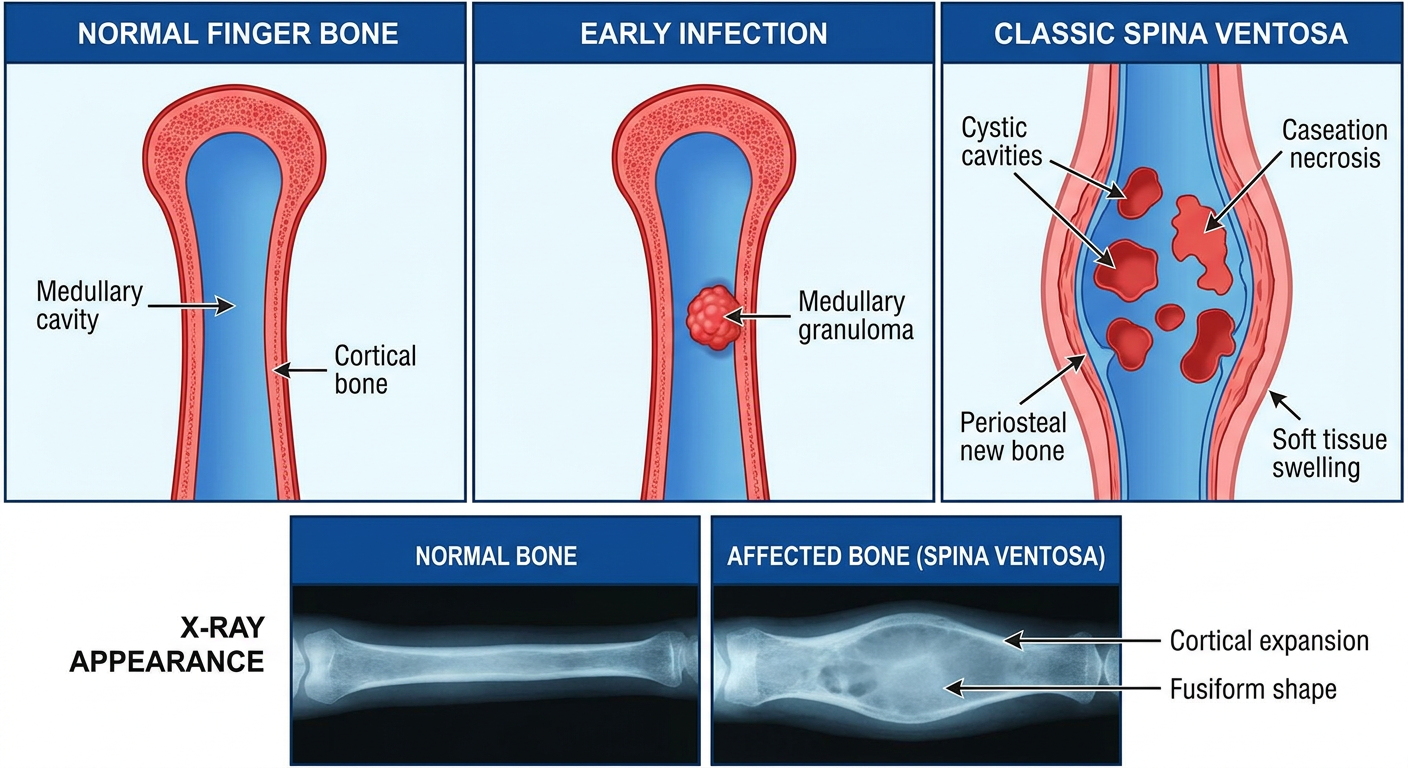
Medical educational diagram showing the pathological progression of Spina Ventosa (tuberculous dactylitis): Left panel shows normal finger bone, middle panel shows early infection with Mycobacterium tuberculosis granuloma in medullary cavity, right panel shows classic expanded fusiform bone lesion with cystic cavities labeled "Spina Ventosa". Below shows X-ray appearance comparison between normal and affected bone. Include labels for: Medullary granuloma, Caseation necrosis, Periosteal new bone, Cortical expansion, Soft tissue swelling. Medical textbook style diagram with blue and red color coding
Spina Ventosa (Tuberculous Dactylitis) - Complete Guide
Definition and Etymology
"Spina Ventosa is a destructive cortical lesion surrounding the medullary canal along with progressive subperiosteal hyperplasia, resembling roentgenographically like a tumour." - American Journal of Translational Research, 2024
Etiology
Causative Organism
- Mycobacterium tuberculosis is the primary pathogen
- Rarely, atypical (nontuberculous) mycobacteria may cause a similar picture - as emphasized in Campbell's Operative Orthopaedics 15th Ed 2026
Route of Infection
- Haematogenous spread (lympho-hematogenous) is the dominant route - the lung acts as the primary focus in approximately 75% of cases
- Less commonly: direct inoculation or contiguous spread from adjacent structures
Risk Factors and Epidemiology
- Primarily a disease of children under 6 years (most common under 5 years); rare after age 6 due to changes in blood supply pattern
- Males and females equally affected
- Poverty, malnutrition, overcrowding, and immunocompromise (HIV) are major risk factors
- Endemic in South Asia, Sub-Saharan Africa, and Southeast Asia
- Exposure to an adult with pulmonary tuberculosis is often traceable
- Skeletal TB accounts for only 1-5% of all TB cases; of those, spina ventosa is uncommon but characteristic
Why Short Tubular Bones?
Pathology
Gross Pathology - Stage by Stage
- Mycobacteria carried in blood lodge in the centre of the marrow cavity through the large nutrient artery
- The nutrient artery of the short tubular bone enters centrally, depositing the first inoculum in the medullary canal
- The interior of the short tubular bone is gradually converted into a tuberculous granuloma
- Typical caseating granulomas form: epithelioid macrophages, Langhans giant cells, lymphocytes, plasma cells, and central caseation necrosis
- The nutrient artery becomes occluded by granulomatous inflammation
- Granulomatous destruction expands outward, causing:
- Destruction of internal bone lamellae
- Thinning and expansion of the cortex
- Subperiosteal new bone formation (periosteal reaction lifts the cortex outward)
- The bone takes on a fusiform/spindle-shaped expanded appearance
- Sequestra may form (though less common than in pyogenic osteomyelitis)
- Natural course: healing with shortening of the bone and deformity of the neighbouring joint
- Complications: sinus formation (discharging sinuses through skin), secondary pyogenic infection, pathological fracture
Histopathology
- Caseating epithelioid granulomas with Langhans giant cells
- Acid-fast bacilli (AFB) demonstrable by Ziehl-Neelsen (ZN) stain (though often paucibacillary and difficult to detect)
- Caseation necrosis in the centre of granulomas
- Surrounding fibrous reaction in chronic cases
Clinical Features: Signs and Symptoms
Characteristic Presentation
| Feature | Description |
|---|---|
| Age | Predominantly under 5-6 years |
| Onset | Insidious, over weeks to months |
| Primary symptom | Painless (or mildly painful) swelling of a digit |
| Duration before diagnosis | Typically 2-6 months |
| General features | Usually afebrile; low-grade fever possible |
Local Signs
- Fusiform/spindle-shaped swelling of the affected digit - this is the hallmark
- Swelling is initially small, gradually progressive
- Bony hard consistency on palpation, fixed to underlying bone
- Mildly tender; local temperature may be slightly raised
- No joint involvement initially (joints typically spared in early stages)
- Skin over the swelling is normal in appearance early on
- Sinus formation may occur in advanced cases with discharge of caseous material
Systemic Signs
- Anorexia and weight loss are common
- Low-grade fever (may be absent - unlike pyogenic osteomyelitis where fever is high)
- No acute inflammatory signs (no intense redness, warmth, or severe pain) - this "quiet" presentation is a key differentiating feature from pyogenic infection
- Signs of primary pulmonary tuberculosis (cough, lymphadenopathy) may coexist
- Multiple digits may be affected simultaneously in children
Distribution
- Hand > foot (hands more commonly involved than feet)
- Phalanges > metacarpals > metatarsals
- Index and middle fingers most commonly affected
- Multiple bones may be involved simultaneously in some children
Investigations
1. Blood Investigations
- ESR - elevated (e.g. 72 mm/1st hour in reported cases)
- CRP - elevated
- CBC - mild anaemia, lymphocytosis possible
- Mantoux test (TST) - positive in the majority of cases; note that a positive test only indicates TB infection, not necessarily disease
- IGRA (Interferon-Gamma Release Assay) - more specific than TST; useful in BCG-vaccinated children
2. Imaging Studies
Plain X-Ray (First-Line, Most Important)
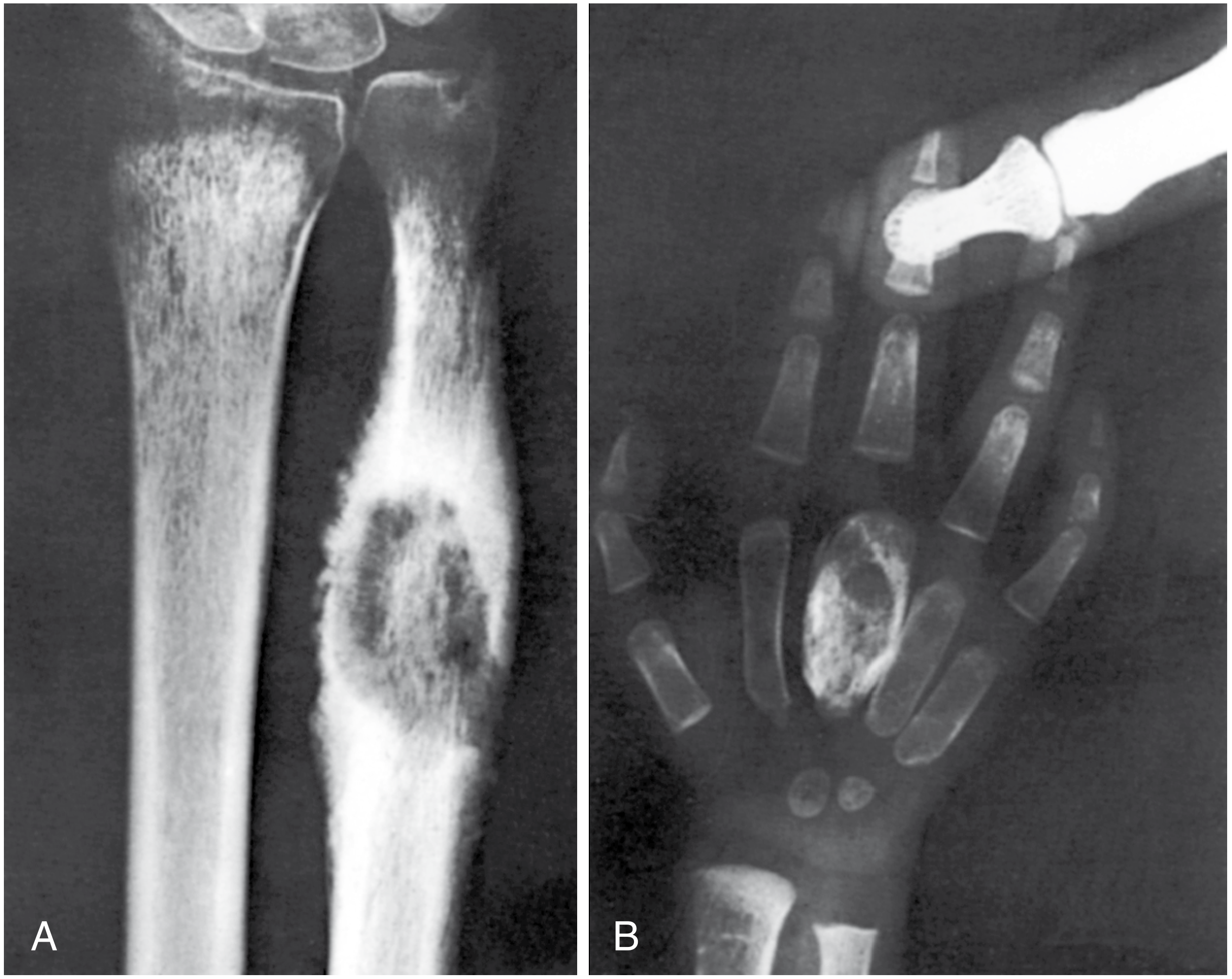
- Cyst-like lytic cavities within the expanded bone
- Diaphyseal expansion - fusiform/balloon-like widening of the bone shaft
- Cortical thinning with periosteal new bone
- Soft tissue swelling around the affected digit
- Absence of sequestra (or small sequestra) - distinguishes from pyogenic osteomyelitis
- Diffuse osteopenia of the involved bone - distinguishes from pyogenic infection
- Internal septations may be visible
- Sclerotic margins in long-standing cases
"Tuberculous dactylitis is rare but classically appears as cyst-like cavities associated with diaphyseal expansion more commonly affecting the bones of the hands than the feet - known as spina ventosa." - Grainger & Allison's Diagnostic Radiology
Ultrasound (US)
- Simple, non-invasive, no radiation
- Identifies soft tissue swelling, periosteal reaction, fluid collections
- Guides fine needle aspiration (FNAC)
CT Scan
- Defines extent of cortical destruction more precisely
- Identifies sequestra if present
- Shows bony sclerosis and destruction
- Not always required but useful in atypical cases
MRI (Gold Standard for Soft Tissue and Early Marrow Involvement)
- Highest sensitivity and specificity
- T1: low signal in medullary cavity (granuloma/pus)
- T2: high signal (oedema, caseous material)
- Gadolinium-enhanced: avid enhancement of granulation tissue
- Shows early marrow involvement before X-ray changes appear
- Identifies soft tissue abscess and sinus tracks
- Best for evaluating extent of disease and surgical planning
3. Microbiological Investigations
- Fine Needle Aspiration Cytology (FNAC) - first-line diagnostic procedure; shows caseating granulomas with epithelioid cells and Langhans giant cells
- AFB smear (ZN staining) of aspirated material - often negative due to paucibacillary nature
- Culture (Lowenstein-Jensen medium / MGIT BACTEC) - gold standard but slow (4-8 weeks)
- GeneXpert MTB/RIF - rapid molecular diagnosis; detects MTB DNA and rifampicin resistance within 2 hours; increasingly used as first-line
- Histopathology (biopsy) - confirmatory; shows typical caseating granulomas
4. Chest X-Ray
- Mandatory in all cases to identify primary pulmonary focus or miliary TB
- Pulmonary TB found in approximately 75% of cases
5. Sputum / Nasopharyngeal Swabs
- In children: induced sputum or gastric lavage for AFB smear and culture
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Enchondroma | No soft tissue swelling; no systemic features; lobulated calcifications on X-ray |
| Pyogenic osteomyelitis | Acute onset; high fever; severe pain; sequestra common; elevated WBC |
| Brodie's abscess | Well-defined lytic lesion with sclerotic rim; usually metaphyseal in long bones |
| Syphilitic dactylitis | Positive Wassermann/VDRL; responds to antisyphilitic therapy (historically confused - as in the Campbell's case) |
| Sarcoidosis | "Lace-like" trabecular pattern; bilateral; elevated ACE; systemic features |
| Giant cell tumour | Epiphyseal location; different age group |
| Actinomycosis | Multiple sinuses; sulfur granules; causative organism identifiable |
Treatment
1. Anti-Tubercular Therapy (ATT) - Mainstay of Treatment
Intensive Phase (2 months) - 4 drugs (2HRZE)
| Drug | Dose |
|---|---|
| Isoniazid (H) | 10 mg/kg/day (max 300 mg) |
| Rifampicin (R) | 10-15 mg/kg/day (max 600 mg) |
| Pyrazinamide (Z) | 35 mg/kg/day |
| Ethambutol (E) | 20 mg/kg/day |
Continuation Phase (7-10 months) - 2 drugs (HR)
| Drug | Dose |
|---|---|
| Isoniazid (H) | 10 mg/kg/day |
| Rifampicin (R) | 10-15 mg/kg/day |
2. Supportive Measures
- Splinting/immobilisation of the affected digit in the early phase to reduce pain
- Analgesics (NSAIDs)
- Nutritional support, iron supplementation
- Pyridoxine (Vitamin B6) supplementation with isoniazid to prevent peripheral neuropathy
3. Surgical Treatment (Secondary - Limited Role)
| Indication | Procedure |
|---|---|
| Failure of conservative ATT | Curettage of the lesion |
| Diagnostic uncertainty (biopsy needed) | Excisional biopsy or FNAC |
| Extensive destruction with shortening | Bone grafting after curettage |
| Pathological fracture | Stabilisation |
| Secondary pyogenic infection | Drainage |
| Sinus tracts not healing | Excision |
4. Monitoring Response
- Clinical: reduction in swelling, pain resolution, weight gain, improved appetite
- ESR and CRP normalisation
- Serial plain X-rays: progressive healing, sclerosis, reconstitution of bone
Prognosis
- Excellent with early diagnosis and complete ATT
- Natural (untreated) course leads to shortening of the affected bone and joint deformity
- Early treatment prevents bone shortening and deformity
- Recurrence is rare with complete treatment
- Drug resistance (MDR-TB) should be suspected and tested for in non-responders
Key Points Summary
| Feature | Detail |
|---|---|
| Cause | Mycobacterium tuberculosis |
| Age group | < 5-6 years |
| Bones involved | Metacarpals, metatarsals, phalanges (hands > feet) |
| Pathology | Caseating tuberculous granuloma, spindle-shaped bone expansion |
| Key symptom | Painless progressive fusiform swelling of a digit |
| Gold standard imaging | MRI; plain X-ray for classic appearance |
| Confirmatory test | Biopsy/FNAC + histopathology / GeneXpert |
| Treatment | 9-12 months ATT (2HRZE / 7HR) |
| Prognosis | Excellent with treatment |
- Campbell's Operative Orthopaedics 15th Ed 2026, p.1068 - Figure 25.17 and spina ventosa description
- Grainger & Allison's Diagnostic Radiology - Osteomyelitis section
- Gupta S et al., Am J Transl Res 2024 - Paediatric Spina Ventosa case report (PMID 39262713)
- Abebe W, PMC 2016 - Tuberculous Dactylitis: An Uncommon Presentation