See this topic and teach me retinal vasculitis from very basic to advanced level
Reading File
Reading File
Running Command
python -m markitdown /home/daytona/workspace/attachments/0a5451af-22c2-4a75-826d…
Finding Sources
Finding Sources
Running Command
cd /home/daytona/workspace/attachments/0a5451af-22c2-4a75-826d-89d6c4db7585/ && …
Reading File
Reading File
Running Command
python3 -c " import zipfile, re pptx_path = '/home/daytona/workspace/attachments…
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
retinal vasculitis treatment immunosuppression
I now have all the material I need from the PPTX, the medical library (Kanski, Rheumatology textbook, Robbins, Harrison's), and PubMed. Let me compile the complete teaching session.
Retinal Vasculitis: Basic to Advanced
Based on your Fellowship PPTX (Dr. Seema Bhandari) + Kanski's Clinical Ophthalmology 10th Ed., Firestein & Kelley's Textbook of Rheumatology, Robbins Pathologic Basis of Disease, Harrison's 22nd Ed., and the 2026 IUSG ReViSe Systematic Review [PMID: 40983164]
1. DEFINITION
Retinal vasculitis is inflammation of the retinal blood vessels characterized by perivascular cuffing, vascular leakage, vascular occlusion, or a combination, identified on fundoscopy or fluorescein angiography. It may be primary (isolated to the eye) or secondary to systemic disease.
Key point from Firestein & Kelley: Retinal vasculitis is diagnosed clinically and angiographically - not histologically - because retinal biopsy carries prohibitive morbidity. The term is somewhat imprecise because it does not always indicate true vessel wall destruction.
- Firestein & Kelley's Textbook of Rheumatology, p. 4462
2. EPIDEMIOLOGY
| Parameter | Figure |
|---|---|
| Proportion of uveitis cases with retinal vasculitis | ~30% |
| Bilateral involvement at presentation | 15-40% |
| Male-to-female ratio (Eales disease) | 2-3:1 |
| Peak incidence age | 15-45 years (varies by etiology) |
3. CLASSIFICATION
By vessel affected:
- Arteritis - arteries involved; typically severe, ischemic, sight-threatening
- Phlebitis / Periphlebitis - veins involved; more common, predominantly inflammatory
- Capillaritis - capillaries; macular edema dominant
- Panvasculitis - both arteries and veins (classic in Behçet disease, SLE)
By etiology:
| Category | Examples |
|---|---|
| Infectious | TB, syphilis, CMV, HSV/VZV (ARN), toxoplasmosis, Lyme |
| Autoimmune / Systemic | Behçet disease, SLE, sarcoidosis, MS, ANCA vasculitis, RA |
| Idiopathic (primary ocular) | Eales disease, IRVAN, Frosted branch angiitis |
| Masquerade | Lymphoma, leukemia, retinitis pigmentosa |
The SUN (Standardization of Uveitis Nomenclature) Working Group classification is the internationally accepted reference standard.
4. PATHOPHYSIOLOGY & IMMUNOLOGY
This is the mechanistic backbone. Understand this and the rest falls into place.
TRIGGER ANTIGEN
(microbial, autoantigen, immune complex)
↓
TLR signaling + Complement activation
↓
CD4+ Th1 → IFN-γ
CD4+ Th17 → IL-17 ← Innate/Adaptive immune bridge
TNF-α, IL-6, IL-10
↓
Breakdown of BLOOD-RETINAL BARRIER (BRB)
↓
Leukocyte adhesion (ICAM-1, VCAM-1)
Neutrophil/Monocyte transmigration
↓
PERIVASCULAR CUFFING (histology hallmark)
↓
Vascular occlusion → Ischemia → VEGF upregulation
↓
Neovascularization → Vitreous hemorrhage / TRD
Key immunologic mediators: TNF-α, IFN-γ, IL-6, IL-17, IL-10 drive inflammation. This explains why anti-TNF agents (infliximab, adalimumab) are so effective. - Nussenblatt RB, Foster CS & Vitale AT
5. CLINICAL FEATURES
Symptoms (what the patient complains of):
| Symptom | Mechanism |
|---|---|
| Floaters (most common) | Vitreous cells/debris from periphlebitis |
| Decreased vision | Macular edema, vitreous hemorrhage, or ischemia |
| Photopsia | Traction or severe vitreous inflammation |
| Redness/Pain | Anterior uveitis component |
| Scotoma | Branch or central RVO/RAO |
| Asymptomatic | Peripheral phlebitis - incidental finding on FFA |
Signs (what you see on examination):
| Sign | Significance |
|---|---|
| Perivascular sheathing | White/gray cuffing - perivenous or periarterial; the hallmark |
| Vitreous cells | Activity marker |
| Macular edema (CME) | Most common cause of VA loss (40-60% of patients) |
| Cotton wool spots | Ischemia; associated with arteritis |
| Vascular occlusion | BRVO, BRAO, CRVO, or combined |
| Neovascularization | NVD or NVE → risk of vitreous hemorrhage |
| Retinal hemorrhages | Variable pattern by etiology |
6. CHARACTERISTIC FUNDUS PATTERNS BY ETIOLOGY
This is where pattern recognition becomes your clinical tool.
Eales Disease
- Classic "young Indian male" peripheral periphlebitis
- Peripheral venous disease → ischemia → NVE → recurrent vitreous hemorrhage
- Diagnosis of exclusion; associated with hypersensitivity to tubercular protein
- Staging: Stage I = Periphlebitis | Stage II = Ischemia | Stage III = NVE | Stage IV = Regression
Behçet Disease
- Occlusive vasculitis affecting both arteries AND veins - the most severe form
- Explosive, recurrent attacks with dense vitritis, retinal hemorrhage, disc swelling
- Associated with oral/genital aphthae, skin pathergy; HLA-B51 positive
- Cumulative ischemic damage over repeated episodes → optic atrophy
- Without treatment: 74% of eyes have VA worse than 20/200 within 5 years - Firestein & Kelley, p. 364
Sarcoidosis
- "Candle-wax drippings" (taches de bougie) - perivenous nodular exudates, the pathognomonic sign
- Also: vitreous "string of pearls," choroidal granulomas, disc granuloma (Lauber's spot), sea fan NVE
- Granulomatous periphlebitis; often bilateral
- Look for bilateral hilar lymphadenopathy, elevated ACE/serum lysozyme
TB-associated Vasculitis
- Peripheral perivenous sheathing ± choroidal tubercles or tuberculoma
- Can mimic Eales disease exactly - many "Eales" cases show TB serology evidence
- Confirm with Mantoux/IGRA, chest CT, aqueous PCR where feasible
- QuantiFERON-TB Gold: specificity 97%, sensitivity 78% (preferred in BCG-vaccinated)
MS-Associated Vasculitis
- Peripheral retinal periphlebitis (venous sheathing) in a subset of MS patients
- Overlaps with pars planitis; inferior peripheral "snowbanking" and vitreous "snowballs"
- Sheathing may be subclinical, detectable only on FFA
IRVAN Syndrome (Idiopathic Retinal Vasculitis, Aneurysms, Neuroretinitis)
- Rare; affects healthy young women - Kanski's, p. 516
- Multiple fusiform arteriolar aneurysms clustered near major bifurcations and disc
- Neuroretinitis with macular star exudate
- Progressive peripheral capillary non-perfusion → NVE
- Steroids have little effect on retinal ischemia; responds to infliximab
Frosted Branch Angiitis (FBA)
- Severe diffuse perivascular sheathing of BOTH arteries and veins - the "frosted branch" appearance
- Primary (idiopathic, children/young adults, often self-limited) or secondary (CMV, HSV, sarcoidosis, lymphoma)
- Treatment: systemic corticosteroids + treat the underlying cause
7. IMAGING - FFA, ICGA, OCT, OCT-A
Fundus Fluorescein Angiography (FFA) - the Gold Standard Investigation
| Phase | What to Look For |
|---|---|
| Arterial | Arterial wall staining/filling defects → arteritis; arterial non-perfusion → BRAO |
| Venous | Perivenous leakage/staining → active phlebitis; venous beading/dilation |
| Late | Disc hyperfluorescence (optic nerve involvement); macular CME (petaloid pattern) |
| Peripheral | Capillary non-perfusion zones (NPA); NVE leakage; AV communications |
Key teaching point: FFA is mandatory because fundoscopy underestimates activity. Widefield FFA (Optos/Heidelberg 200° field) detects 30-50% more peripheral non-perfusion than 7-field photography.
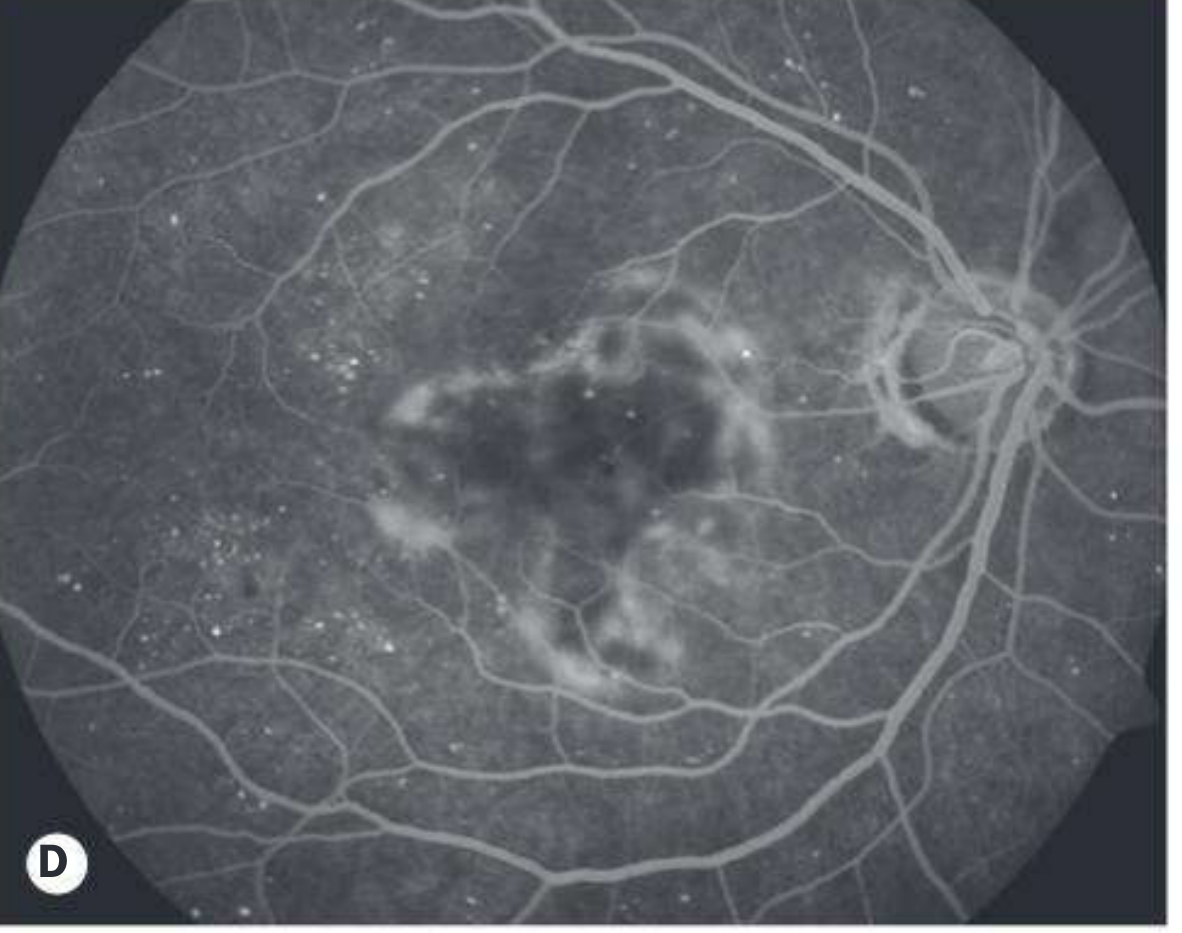
The two most sensitive angiographic activity markers are disc hyperfluorescence + vascular leakage.
Color fundus photo showing IRVAN-associated retinal vasculitis:

FFA showing hyperfluorescence from retinal leakage in IRVAN:
ICG Angiography (ICGA)
- Detects choroidal involvement - hypofluorescent spots (granulomas in sarcoid, Behçet)
- Better visualization of choriocapillaris ischemia and deep vessel detail
- In Birdshot chorioretinopathy: multiple hypofluorescent spots beyond visible fundus lesions
OCT Findings
| OCT Feature | Clinical Significance |
|---|---|
| CME (intraretinal cysts) | Active inflammation, leading cause of VA loss |
| Subretinal fluid | Active exudation |
| Ellipsoid zone disruption | Photoreceptor damage - predicts final VA |
| Epiretinal membrane | Fibrovascular proliferation complication |
| Vitreous hyperreflective dots | Active vitritis on OCT |
OCT-Angiography (OCT-A)
- Maps the superficial and deep capillary plexus without dye injection
- Detects capillary dropout / foveal avascular zone (FAZ) enlargement
- Identifies subclinical NVE flow
- Limitation: cannot detect leakage (only structural flow mapping)
8. SYSTEMIC WORKUP ALGORITHM
Tier 1 - ALL Patients
- CBC, ESR, CRP
- Serum ACE (sarcoidosis)
- VDRL/TPHA (syphilis)
- Chest X-ray / CT chest
- Mantoux / IGRA (TB)
- Toxoplasma IgG/IgM
- RA factor, ANA, dsDNA (SLE)
- ANCA (systemic vasculitis)
- HLA-B51 (Behçet, especially in endemic populations)
Tier 2 - Selected Cases
- MRI brain (MS, CNS sarcoidosis)
- Fluorescein / ICGA angiography
- Anterior chamber tap for PCR/cytology (viral, lymphoma)
- PET-CT (occult malignancy, systemic sarcoid)
- Vitreous biopsy (masquerade syndromes)
Clinical Pearl #1: Always exclude infection before starting immunosuppression. TB and syphilis are the great mimickers.
9. DIFFERENTIAL DIAGNOSIS
Infectious Mimics
- CMV retinitis: perivascular "frosting" + hemorrhagic necrosis; immunocompromised patients
- ARN (Acute Retinal Necrosis, HSV/VZV): peripheral full-thickness necrosis with occlusive arteritis
- Syphilitic uveitis: multifocal, FTA-ABS positive; the "great imitator"
- Toxoplasmosis: focal retinochoroiditis + adjacent vasculitis - "headlight in fog" appearance
Non-Inflammatory Vascular Masquerades
- CRVO/BRVO: disc edema, flame hemorrhages, venous dilation (no leukocytic cuffs on FFA)
- Diabetic retinopathy: NVE/NVD + microaneurysms (no inflammatory cells)
- Hypertensive retinopathy: AV nipping, hard exudates, copper/silver wiring
- Radiation retinopathy: history of orbital/ocular radiation
10. TREATMENT PROTOCOLS
Step 1 - Treat the Underlying Cause (if infectious)
| Pathogen | Treatment |
|---|---|
| TB | ATT: 2HRZE + 4HR (consider extending to 9-12 months for posterior uveitis) |
| Syphilis | IV/IM penicillin G |
| CMV | IV ganciclovir / oral valganciclovir |
| HSV/VZV (ARN) | IV acyclovir → oral valacyclovir |
| Toxoplasmosis | Sulfamethoxazole-trimethoprim or pyrimethamine + sulfadiazine |
For TB: Never start steroids before ATT in confirmed TB. In probable ocular TB, simultaneous start is acceptable. Expect a paradoxical reaction (10-40% worsen initially) - add oral prednisolone 0.5 mg/kg/day after 4 weeks of ATT.
Step 2 - Control Inflammation (Non-infectious)
| Route | Agent | Note |
|---|---|---|
| Systemic (1st line) | Prednisone 1 mg/kg/day | Taper over 3-6 months |
| Periocular | Posterior sub-Tenon's triamcinolone | Unilateral disease |
| Intravitreal | Triamcinolone or dexamethasone implant | CME |
Corticosteroids delay progression but do NOT alter the ultimate outcome in Behçet - hence immunosuppression is essential.
Step 3 - Steroid-Sparing Immunosuppression
| Line | Drug | Dose |
|---|---|---|
| 2nd line | Methotrexate, Mycophenolate mofetil, Azathioprine | As per protocols |
| 3rd line | Cyclosporine (4-5 mg/kg/day), Tacrolimus | Avoid cyclosporine monotherapy in Behçet (neurological risk) |
| Behçet 1st line | Azathioprine 2-3 mg/kg/day | Yazici 1990 RCT - reduces attack frequency; EULAR 2018 guideline |
Step 4 - Biologic Agents
| Agent | Indication | Key Evidence |
|---|---|---|
| Infliximab (anti-TNF) | Behçet, severe refractory vasculitis, IRVAN | Effective at ≥5 mg/kg/infusion |
| Adalimumab (anti-TNF) | Non-infectious uveitis (FDA approved) | VISUAL I (active uveitis: HR 0.50, p<0.001) and VISUAL II (inactive: HR 0.57, p=0.004) - first FDA-approved biologic for non-infectious uveitis |
| Interferons | Behçet refractory to above | |
| Rituximab (anti-CD20) | ANCA-associated |
The MUST Trial (2014): Fluocinolone acetonide implant vs systemic therapy - non-inferior VA outcomes; but implant group had 80% cataract surgery rate and 37% IOP-lowering procedure rate. Systemic therapy preferred for bilateral disease.
Step 5 - Laser and Surgery
| Modality | Indication |
|---|---|
| PRP (Panretinal photocoagulation) | Eales Stage III-IV NVE; NPA >4 disc areas; reduces NVE regression rate ~80% |
| Anti-VEGF + PRP | Combination superior to PRP alone for active NVE (RCT evidence, 2018) |
| Intravitreal anti-VEGF | CME (bevacizumab, ranibizumab); NVE (as adjunct) |
| PPV (Pars plana vitrectomy) | Non-clearing VH >3 months, TRD threatening macula, ERM |
11. DISEASE-SPECIFIC PROTOCOLS
Behçet Disease
EULAR 2018 Recommendations (Hatemi et al.):
- Posterior uveitis/vasculitis → Azathioprine + systemic corticosteroids (1st line)
- Severe/vision-threatening → Anti-TNF (infliximab or adalimumab)
- Acute attack → Systemic CS + cyclosporine 4-5 mg/kg/day
- Avoid cyclosporine monotherapy due to neurological toxicity risk
Behçet Diagnostic Criteria (International Study Group):
- Recurrent oral ulceration (mandatory) + 2 of: genital ulceration, ocular lesions (uveitis/vasculitis), skin lesions (erythema nodosum, pseudofolliculitis), positive pathergy test
Sarcoidosis
- Systemic and/or periocular corticosteroids first
- Steroid-sparing agents for chronic disease (methotrexate, mycophenolate)
- Always confirm with tissue biopsy when possible; chest CT for hilar adenopathy
12. COMPLICATIONS & PROGNOSIS
| Complication | Frequency | Management |
|---|---|---|
| Cystoid Macular Edema | 40-60% of patients; leading cause of VA loss | Intravitreal steroids, anti-VEGF, systemic immunosuppression |
| Vitreous Hemorrhage | 30-50% in Eales; 60-70% clear spontaneously in 3 months | PPV if persistent >3 months |
| Neovascularization (NVD/NVE) | Correlates with NPA extent | PRP + anti-VEGF |
| Tractional RD | Fibrovascular proliferation over NVE | Complex PPV + silicone oil; guarded prognosis |
| Optic Atrophy | End-stage from ischemia/inflammation | Prevention via early treatment |
| Rubeosis iridis | Anterior neovascularization from ischemia | Anti-VEGF + PRP |
Prognosis by Disease
| Disease | Prognosis |
|---|---|
| Eales disease (uncomplicated) | Good if treated early; recurrent VH is main risk |
| Behçet (untreated) | Poor - 74% <20/200 in 5 years |
| Behçet (with anti-TNF) | Substantially improved; attacks reduced |
| Sarcoidosis | Generally favorable; chronic relapsing course |
| IRVAN | Variable; PRP reduces NVE risk |
| FBA (idiopathic) | Usually good prognosis; often self-limited |
13. KEY CLINICAL PEARLS (Fellowship Level)
-
Always exclude infection before immunosuppression. TB and syphilis mimic every form of non-infectious vasculitis.
-
FFA is mandatory - fundoscopy consistently underestimates disease activity. Widefield FFA detects 30-50% more peripheral NPA.
-
CME is the leading cause of VA loss (40-60% of patients). OCT-guided therapy is the standard of care.
-
Behçet retinal vasculitis - anti-TNF biologics (infliximab/adalimumab) are disease-modifying. Start early, do not wait for conventional therapy failure.
-
Adalimumab is the only FDA-approved biologic for non-infectious uveitis (VISUAL I & II Trials, 2016).
-
PRP + anti-VEGF combination is superior to PRP alone for NVE in Eales - RCT evidence (2018).
-
OCT-A reveals subclinical capillary dropout and FAZ enlargement even in clinically quiet eyes - prognostically important.
-
TB paradoxical reaction: 10-40% worsen initially on ATT. Do not abandon treatment - add steroids after 4 weeks of ATT.
-
Cyclosporine monotherapy in Behçet is contraindicated due to neurotoxicity risk.
-
IGRA (QuantiFERON-TB Gold) is preferred over Mantoux in BCG-vaccinated populations (specificity 97%, sensitivity 78%).
14. LATEST EVIDENCE (2026)
A 2026 systematic review from the International Uveitis Study Group (IUSG) ReViSe Study (PMID: 40983164) systematically reviewed clinical trials in non-infectious retinal vasculitis treatment, confirming the evidence base for immunosuppressive strategies covered in this overview. This represents the most current evidence synthesis available.
Summary Mind Map
RETINAL VASCULITIS
│
├── DEFINITION: Inflammation of retinal vessels + intraocular inflammation
│ ± vascular occlusion
│
├── TYPES: Arteritis (severe/ischemic) | Phlebitis (common) | Capillaritis | Panvasculitis
│
├── PATHOPHYSIOLOGY
│ TLR → Th1/Th17 → TNF-α/IL-17/IFN-γ → BRB breakdown → cuffing → occlusion
│
├── ETIOLOGY MNEMONICS
│ BEST-BITE: Behçet, Eales, Sarcoid, TB | Syphilis, Infectious (CMV/ARN), TB, others
│
├── INVESTIGATION HIERARCHY
│ Fundoscopy → FFA (mandatory) → OCT/OCT-A → ICGA → Blood workup (Tier 1 & 2)
│
├── TREATMENT LADDER
│ Treat infection → Corticosteroids → Immunosuppressants → Biologics → Laser/Surgery
│
└── LEADING CAUSE OF VA LOSS: CME (40-60%) → OCT-guided prompt treatment
Sources: Kanski's Clinical Ophthalmology 10th Ed. (p. 516); Firestein & Kelley's Textbook of Rheumatology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Harrison's Principles of Internal Medicine 22nd Ed.; Rheumatology 2-Volume Set (Elsevier 2022); IUSG ReViSe Systematic Review, Surv Ophthalmol 2026 [PMID 40983164]; Fellowship PPTX by Dr. Seema Bhandari
Teach me from basics, anatomy and physiology and applied aspect to it in detail
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
I now have comprehensive material from Guyton & Hall Medical Physiology, Kanski's Clinical Ophthalmology 10th Ed., Costanzo Physiology, and neuroscience textbooks. Let me compile the complete, detailed teaching session.
Retinal Anatomy, Physiology & Applied Aspects to Vasculitis
A Complete Teaching Session - Basics to Advanced
Sources: Guyton & Hall Medical Physiology, Kanski's Clinical Ophthalmology 10th Ed., Costanzo Physiology 7th Ed., Junqueira's Basic Histology 17th Ed., Firestein & Kelley's Rheumatology, Robbins Pathologic Basis of Disease
PART 1 - RETINAL ANATOMY
1.1 What Is the Retina?
The retina is a specialized sensory epithelium lining the inner surface of the posterior two-thirds of the globe. It is approximately 0.1-0.5 mm thick (thicker at the macula and disc margin, thinnest at the fovea center and ora serrata) and is derived embryologically from the diencephalon - it is, in essence, a displaced piece of brain tissue. This has massive implications for how it responds to inflammation and injury.
The retina extends from the optic disc posteriorly to the ora serrata anteriorly, where it merges with the pars plana of the ciliary body. It is held against the underlying retinal pigment epithelium (RPE) not by a true anatomical adhesion but by:
- Active fluid transport by the RPE (out of the subretinal space)
- Interdigitation of RPE microvilli with photoreceptor outer segments
- Intraocular pressure
This is why the retina detaches so easily - there is a potential space (subretinal space) with no true adhesion.
1.2 The Ten Layers of the Retina
Light travels from vitreous inward (inside to outside), passing through inner layers before reaching photoreceptors. This "inverted" organization is a quirk of vertebrate eye evolution.
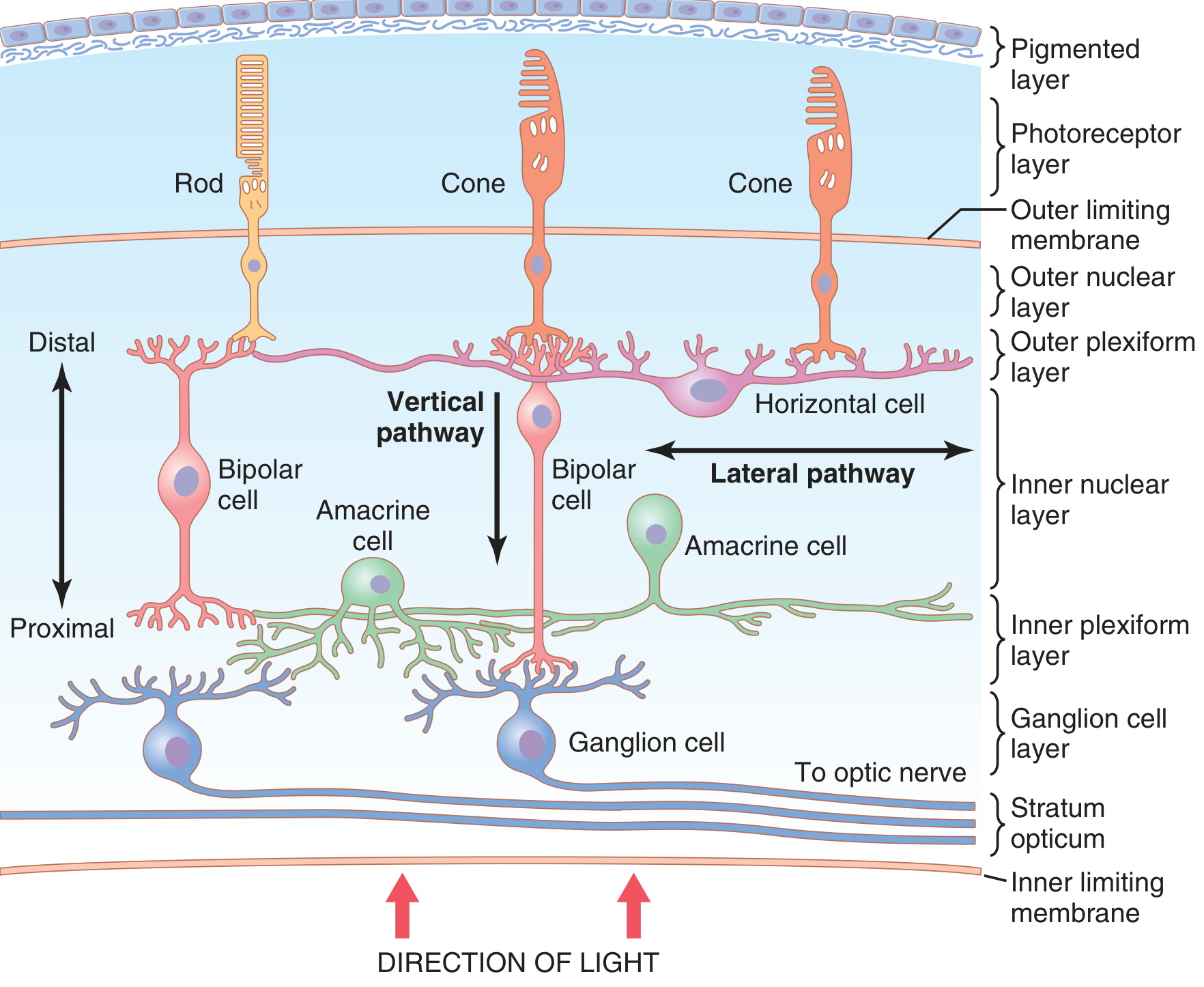
Going from vitreous surface → choroid (i.e., from inside to outside, the direction light travels):
| # | Layer | What It Contains | Applied Point |
|---|---|---|---|
| 1 | Internal Limiting Membrane (ILM) | Basement membrane of Müller cell footplates; separates retina from vitreous | Site of vitreoretinal traction; targeted in ERM peeling surgery |
| 2 | Nerve Fiber Layer (NFL) | Axons of ganglion cells converging to optic disc | Lost in glaucoma & ischemia; OCT-NFL thinning = irreversible damage |
| 3 | Ganglion Cell Layer (GCL) | Cell bodies of RGCs (~1.2 million cells) | Optic atrophy occurs here in end-stage vasculitis ischemia |
| 4 | Inner Plexiform Layer (IPL) | Synapses between bipolar cells, amacrine cells, and ganglion cells | Site of lateral signal integration |
| 5 | Inner Nuclear Layer (INL) | Cell bodies of bipolar, horizontal, amacrine, and Müller cells | Outer capillary plexus lies here |
| 6 | Outer Plexiform Layer (OPL) | Synapses between photoreceptor axons and bipolar/horizontal cells | Hard exudates preferentially deposit here |
| 7 | Outer Nuclear Layer (ONL) | Nuclei/cell bodies of rods and cones | Preserved until very late in vascular disease |
| 8 | Outer Limiting Membrane (OLM) | Zonula adherens between photoreceptors and Müller cells | On OCT: the "ellipsoid zone" line |
| 9 | Photoreceptor Layer | Outer and inner segments of rods and cones | Avascular; nourished entirely by choroid |
| 10 | Retinal Pigment Epithelium (RPE) | Hexagonal pigmented cells; forms outer BRB | The metabolic workhorse of the retina |
Memory trick: I Never Give Idiots Any Of Our Precious Retinas (ILM, NFL, GCL, IPL, INL, OPL, ONL, OLM, Photoreceptors, RPE) - from vitreous to choroid.
1.3 Key Cell Types and Their Roles
Photoreceptors - The Transducers
| Feature | Rods | Cones |
|---|---|---|
| Number | ~120 million | ~6 million |
| Distribution | Peripheral retina, absent at fovea | Concentrated at fovea (6 million in macula) |
| Function | Scotopic (dim light) vision | Photopic (colour, detail) vision |
| Pigment | Rhodopsin | 3 colour opsins (S/M/L, i.e., blue/green/red) |
| Diameter | 2-5 µm (peripheral), narrower centrally | 5-8 µm (peripheral), 1.5 µm at fovea |
| Energy demand | Very high (mitochondria-rich inner segments) | Even higher at fovea |
Both rod and cone outer segments are composed of stacked membrane discs - up to 1000 discs per cell - packed with photopigment. These discs represent ~40% of the outer segment mass. - Guyton & Hall, p. 632
Bipolar Cells
- Midget bipolar: 1:1 connection with foveal cones → high acuity
- Diffuse bipolar: converge multiple rods → high sensitivity (but less acuity)
- ON-center bipolar: depolarize to light
- OFF-center bipolar: hyperpolarize to light
Horizontal Cells
- Lateral inhibition between adjacent photoreceptors
- Responsible for contrast enhancement at edges
Amacrine Cells
- ~30 subtypes; modulate ganglion cell responses
- Play a role in motion detection and directional selectivity
Ganglion Cells (RGCs)
- The only output neuron of the retina
- Their axons form the optic nerve
- Magnocellular (M-cells): motion and low contrast
- Parvocellular (P-cells): fine detail and colour
Müller Cells - The Retinal Glia
- Span the ENTIRE retina from ILM to OLM
- Act as structural scaffolding, metabolic support, potassium buffering (spatial K⁺ buffering)
- Release VEGF under hypoxia → drive neovascularization
- In vasculitis: Müller cell dysfunction → macular edema amplification
Retinal Pigment Epithelium (RPE)
- A single layer of hexagonal cells
- 10 critical functions:
- Absorbs stray light (melanin granules)
- Phagocytoses shed photoreceptor outer segment discs (~30,000 discs/cell/day)
- Re-isomerizes all-trans retinal → 11-cis retinal (visual cycle)
- Maintains ionic environment of subretinal space
- Active fluid transport (keeps subretinal space dry)
- Forms the outer blood-retinal barrier (tight junctions)
- Secretes trophic factors for photoreceptors
- Secretes VEGF toward choroid (maintains choriocapillaris)
- Secretes anti-VEGF PEDF apically
- Immune modulation: secretes immunosuppressive factors (TGF-β, CXCL16, IL-10) - critical for immune privilege
1.4 The Fovea and Macula
| Region | Size | Contents | Clinical Importance |
|---|---|---|---|
| Macula | ~5.5 mm diameter | Xanthophyll pigment, cones > rods | All fine central vision |
| Fovea | ~1.5 mm diameter | Cone-rich, no large vessels | CME = most common cause of VA loss in vasculitis |
| Foveola | 0.35 mm diameter | Pure cones, avascular | Maximum visual acuity (20/20) |
| Foveal Avascular Zone (FAZ) | ~0.35 mm | No capillaries | FAZ enlargement = capillary dropout on OCT-A in vasculitis |
The foveal pit is created by lateral displacement of inner nuclear and ganglion cell layers during fetal development, allowing unimpeded light access to cones. This displacement is what we see as the characteristic foveal contour on OCT.
PART 2 - RETINAL BLOOD SUPPLY (VASCULAR ANATOMY)
2.1 The Dual Blood Supply - The Most Important Concept in Retinal Disease
The retina has two entirely separate circulations that supply different layers:
RETINA
┌──────────────────────────┐
│ INNER 2/3 of retina │ ← RETINAL CIRCULATION
│ (NFL to INL) │ (Central retinal artery branches)
│──────────────────────────│
│ OUTER 1/3 of retina │ ← CHOROIDAL CIRCULATION
│ (ONL, photoreceptors, │ (Short posterior ciliary arteries
│ RPE) │ → choriocapillaris)
└──────────────────────────┘
This duality is why:
- Retinal artery occlusion kills inner retina but spares photoreceptors (initially)
- Choroidal ischemia kills photoreceptors and RPE but spares inner retina
- Retinal vasculitis primarily affects the inner retinal circulation
2.2 The Retinal Circulation in Detail
Origin: The central retinal artery (CRA) is a branch of the ophthalmic artery (first branch of the internal carotid artery). It enters the optic nerve ~12 mm behind the globe and travels within the nerve substance, emerging at the optic disc.
Structure of retinal vessels:
| Vessel | Wall Structure | Applied Point |
|---|---|---|
| Retinal arteries | Tunica intima (endothelium + IEL), media (smooth muscle, internal elastic lamina), adventitia (loose CT) | No external elastic lamina (unlike systemic arteries) |
| Retinal arterioles | Smooth muscle + discontinuous IEL | Autoregulate; site of cotton wool spots |
| Capillaries | Endothelium + basement membrane + pericytes | Forms inner BRB; first to be affected in vasculitis |
| Venules/Veins | Small amount of smooth muscle + elastic tissue | Distensible; enlarge proximally toward central retinal vein |
Key vascular anatomy facts:
- CRA is an end artery - no collateral anastomoses with other retinal arteries
- Cilioretinal artery (present in ~20% of eyes) arises from posterior ciliary circulation → spares a strip of retina in CRA occlusion
- The retinal circulation lacks autonomic innervation (unlike choroidal) - autoregulation is entirely myogenic and metabolic
- A-V ratio normally 2:3 (artery:vein diameter) - reversal suggests hypertension or vascular disease
2.3 The Retinal Capillaries - The Site of Vasculitis
This is where retinal vasculitis plays out at the microscopic level. - Kanski's, p. 7476
Two capillary plexuses exist:
- Superficial/inner plexus: in the ganglion cell layer
- Deep/outer plexus: in the inner nuclear layer
- Both connect at the macula to form a complex ring
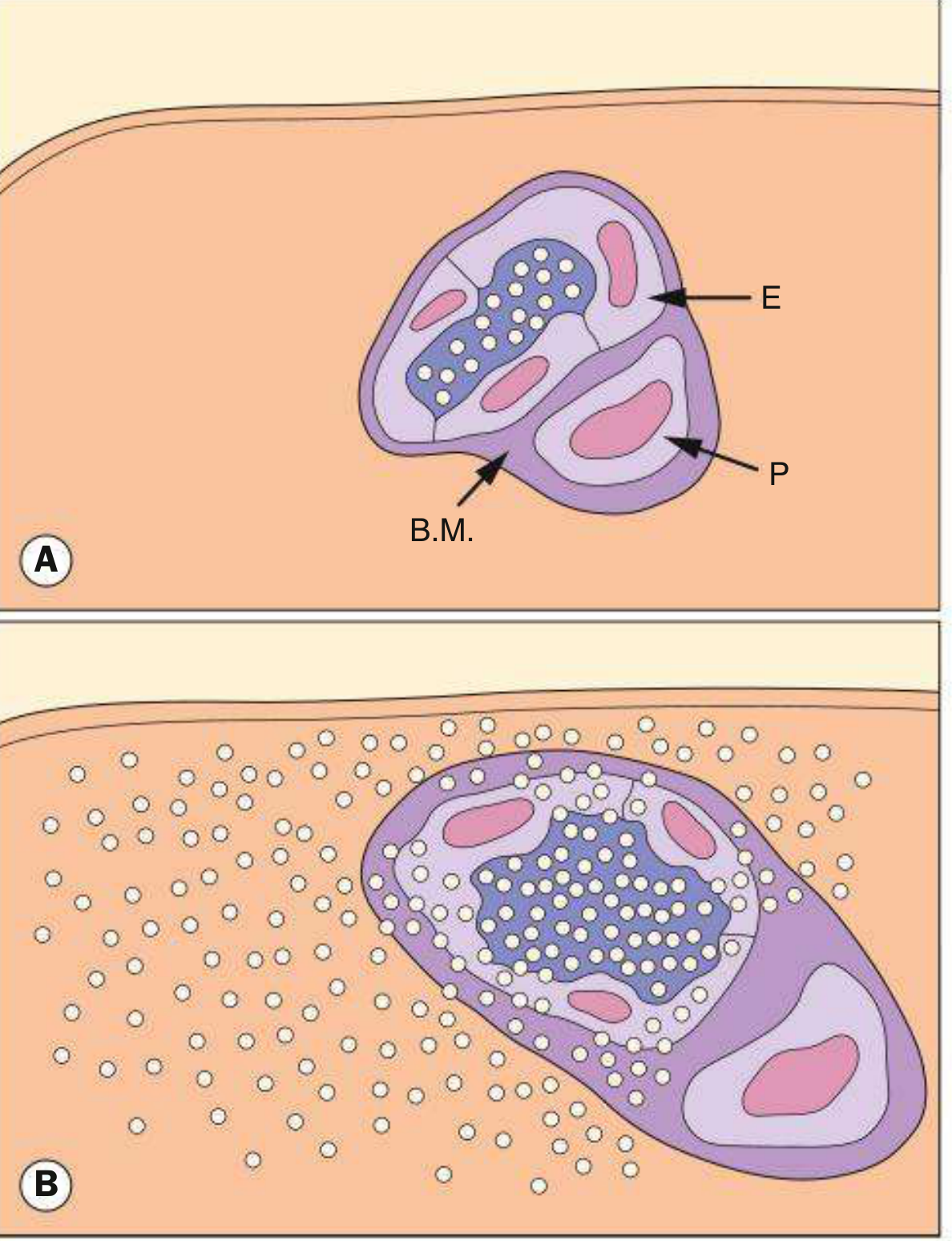
Capillary wall structure (from lumen outward):
- Endothelial cells - single layer; linked by tight junctions = the inner blood-retinal barrier
- Basement membrane - lies beneath endothelial cells
- Pericytes - external to endothelium; enclosed by outer basal lamina; have pseudopodal processes enveloping the capillary
The pericyte-to-endothelial cell ratio in the retina is 1:1 - the highest in the body. This is unique to the retina (compared to 1:3-4 in most other tissues) and reflects the extreme metabolic demands and need for autoregulation.
Capillary-free zones:
- Around arterioles (arteriolar capillary-free zone)
- At the fovea (FAZ - foveal avascular zone, ~0.35 mm)
2.4 The Choroidal Circulation
- Supplied by short and long posterior ciliary arteries (from the ophthalmic artery)
- The choriocapillaris is a fenestrated capillary bed (unlike retinal capillaries)
- Blood flow: ~70 ml/min/100g tissue - the highest perfusion rate in the body
- Functions as the metabolic supply to the outer retina (no autoregulation - entirely pressure-dependent)
- Fenestrated walls allow fluorescein leakage into the extravascular space → blocked by RPE tight junctions = outer BRB
PART 3 - THE BLOOD-RETINAL BARRIER (BRB)
This is THE central concept in retinal vasculitis pathophysiology.
3.1 Inner BRB (iBRB)
- Location: Tight junctions (zonula occludentes) between retinal capillary endothelial cells
- Also known as: the retinal vascular barrier
- Prevents passage of both bound and free fluorescein, proteins, and inflammatory cells
- Pericytes and basement membrane play only a minor supportive role in barrier function - the endothelial tight junctions are the key element - Kanski's, p. 2508
- Integrity maintained by: VEGF antagonism (PEDF), angiopoietin-1 from pericytes, occludin/claudin tight junction proteins
What breaks the iBRB?
- Inflammatory cytokines: VEGF, TNF-α, IL-1β, IL-6 → downregulate occludin, claudin-5
- Leukocyte transmigration → mechanical disruption
- Complement activation → membrane attack complex (MAC)
- Pericyte loss (early event in diabetic retinopathy and vasculitis)
Clinical consequence of iBRB breakdown = MACULAR EDEMA (CME) → the leading cause of visual loss in retinal vasculitis (40-60% of cases)
3.2 Outer BRB (oBRB)
- Location: Tight junctions between RPE cells (zonula occludentes)
- The choriocapillaris is fenestrated (leaky) → fluorescein freely leaks into the extravascular space
- RPE cells physically block this fluorescein from entering the subretinal space
- Disruption of oBRB → subretinal fluid accumulation, RPE detachments, exudative retinal detachment
In retinal vasculitis, the iBRB is primarily affected. The oBRB becomes secondarily affected in severe uveitis or when choroiditis coexists.
PART 4 - RETINAL PHYSIOLOGY
4.1 Visual Transduction (Phototransduction)
The conversion of light into an electrical signal happens in the photoreceptor outer segment.
In the DARK (without light):
- cGMP levels are HIGH
- cGMP-gated Na⁺ channels are OPEN → Na⁺ flows in continuously (the "dark current")
- Rod membrane potential: -40 mV (relatively depolarized)
- Glutamate is continuously released at the synaptic terminal
- This continuously INHIBITS ON-bipolar cells
In the LIGHT:
LIGHT
↓
Photon absorbed by rhodopsin (outer segment disc)
↓
11-cis retinal → all-trans retinal (photoactivation)
↓
Activated rhodopsin (metarhodopsin II)
↓
Activates TRANSDUCIN (G-protein, Gα)
↓
Transducin activates cGMP PHOSPHODIESTERASE (PDE)
↓
cGMP hydrolyzed to 5'-GMP → cGMP levels FALL
↓
cGMP-gated Na⁺ channels CLOSE
↓
Dark current stops; K⁺ continues to exit
↓
HYPERPOLARIZATION (membrane potential → -70 to -80 mV)
↓
Glutamate release STOPS
↓
ON-bipolar cells DEPOLARIZE → ganglion cells fire
This signal amplification is extraordinary: one photon of light → activation of ~500 transducin molecules → activation of ~500 PDE molecules → hydrolysis of ~250,000 cGMP molecules - Guyton & Hall, p. 638
Recovery (dark adaptation):
- Activated rhodopsin phosphorylated by rhodopsin kinase → arrestin binding → inactivation
- Transducin-GTP → Transducin-GDP (intrinsic GTPase activity)
- PDE deactivated
- Guanylyl cyclase restores cGMP
- Na⁺/Ca²⁺-K⁺ exchanger restores Ca²⁺ levels
- All-trans retinal transported to RPE → re-isomerized to 11-cis retinal (the visual cycle, requiring vitamin A)
Applied: Vitamin A deficiency impairs 11-cis retinal regeneration → night blindness (nyctalopia). This can occur with severe uveitis/vasculitis disrupting RPE function.
4.2 Retinal Oxygen Metabolism
The retina is one of the most metabolically active tissues in the body:
- Oxygen consumption: ~5 mL O₂/100g/min (among the highest of any tissue)
- The photoreceptor inner segments are packed with mitochondria to sustain the enormous ATP demand of the dark current (Na⁺/K⁺-ATPase)
Oxygen gradient across the retina:
Vitreous (PO₂ ~10 mmHg)
↑
Inner retina ← supplied by CRA branches (PO₂ ~30-40 mmHg at NFL)
↑
Outer retina ← almost no oxygen (PO₂ approaches 0 mmHg at ONL)
↑
Choriocapillaris (PO₂ ~60-70 mmHg) ← outer retina's sole oxygen source
The outer nuclear layer is the most hypoxic region of the entire retina - this is why photoreceptors are the first to die in choroidal vascular insufficiency and why the ONL is exquisitely sensitive to the effects of subretinal fluid.
Applied to vasculitis: When retinal capillaries are occluded by vasculitis, the inner retina becomes ischemic. The inner nuclear layer neurons die, leaving characteristic cotton wool spots (swollen nerve fiber layer axons - cytoid bodies from axoplasmic flow disruption). With extensive capillary non-perfusion, ischemic drive increases VEGF → neovascularization.
4.3 Retinal Autoregulation
Unlike the choroid, the retinal vasculature has no autonomic innervation and must self-regulate blood flow entirely by:
- Myogenic autoregulation (Bayliss effect): Smooth muscle in arterioles contracts when transmural pressure rises → maintains constant flow over an IOP/BP range of 30-80 mmHg ocular perfusion pressure
- Metabolic autoregulation: Tissue hypoxia → local adenosine/NO release → vasodilation
- Pericyte-mediated regulation: Pericytes contract/relax at the capillary level (the retinal-specific mechanism)
Pericyte loss is the earliest structural change in retinal vascular disease (including vasculitis and diabetic retinopathy). Loss of pericyte contractile tone → capillary dilation, microaneurysm formation, and loss of autoregulation → fluctuating perfusion → accelerated endothelial injury.
PART 5 - OCULAR IMMUNE PRIVILEGE (The Foundation of Why Vasculitis Is Unique in the Eye)
5.1 What Is Immune Privilege?
The eye is an immune-privileged site - meaning it can tolerate foreign antigens without mounting a destructive inflammatory response. This privilege evolved to protect the irreplaceable visual neurons from collateral damage during inflammation. The other immune-privileged sites are the brain, testis, and placenta.
The mechanisms of ocular immune privilege:
| Mechanism | How It Works | Applied Implication |
|---|---|---|
| Blood-retinal barrier (iBRB + oBRB) | Prevents immune cell trafficking into retina | When BRB breaks down (vasculitis), immune cells flood in |
| Anterior chamber-associated immune deviation (ACAID) | Antigens draining via aqueous into blood induce systemic tolerance (Treg expansion) rather than effector immunity | Breakdown → autoimmune retinal disease |
| Constitutive immunosuppressive microenvironment | RPE and iris/CB secrete TGF-β, α-MSH, CXCL16, IL-10, VEGF, sFasL | Suppresses T-cell activation locally |
| Low MHC I expression | Retinal neurons express low MHC class I → less recognition by CD8+ T-cells | Loss of MHC I suppression in inflammation → cytotoxic damage |
| Complement regulatory proteins | CD55/CD59 on retinal cells inhibit complement MAC | Complement activation in vasculitis bypasses these inhibitors |
| Vitreous | Contains TGF-β, CXCL16 → immunosuppressive milieu | Disrupted vitreous in VH exposes retina to systemic immune attack |
5.2 How Immune Privilege Breaks Down in Retinal Vasculitis
TRIGGER (microbial antigen, autoantigen, immune complex)
↓
Pattern recognition by TOLL-LIKE RECEPTORS (TLR2, TLR4, TLR9)
on retinal endothelial cells and RPE
↓
NF-κB activation
↓
Upregulation of:
- ICAM-1 (intercellular adhesion molecule-1)
- VCAM-1 (vascular cell adhesion molecule-1)
- P-selectin, E-selectin
on retinal vessel endothelium
↓
Leukocyte ROLLING, ADHESION, TRANSMIGRATION
(leukostasis in retinal capillaries)
↓
CD4+ T-cells: Th1 (IFN-γ) + Th17 (IL-17) infiltrate perivascular space
↓
PERIVASCULAR CUFFING (white sheathing visible on fundoscopy)
↓
Inflammatory cytokines (TNF-α, IL-6, VEGF) released:
→ Disrupt tight junction proteins (occludin, claudin-5)
→ BRB BREAKDOWN → CME (macular edema)
→ Endothelial apoptosis → vascular wall necrosis → OCCLUSION
↓
ISCHEMIA → HIF-1α upregulation → VEGF surge
↓
NEOVASCULARIZATION (NVE, NVD)
↓
Vitreous hemorrhage, TRD, optic atrophy
PART 6 - CLINICAL ANATOMY-PHYSIOLOGY CORRELATION
Connecting each anatomical/physiological fact to what you see clinically
6.1 Why Periphlebitis Is More Common Than Periarteritis
Retinal veins are more commonly affected (periphlebitis >> periarteritis) because:
- Venous blood flow is slower → longer leukocyte contact time with endothelium
- Venous endothelium expresses higher baseline ICAM-1
- Venous walls are thinner and less able to resist inflammatory cell infiltration
- At arteriovenous crossings, artery and vein share a common adventitial sheath → arterial inflammation can spread to adjacent vein
Exception: Behçet disease affects both arteries and veins simultaneously (panvasculitis) because the underlying defect is a neutrophil-mediated vascular injury driven by complement, not primarily T-cell-mediated.
6.2 Why the FAZ Is Clinically Critical
The foveal avascular zone (FAZ) is normally 0.35 mm in diameter. It is a capillary-free zone supplied entirely by diffusion from the surrounding capillary ring and from the choriocapillaris below.
In retinal vasculitis:
- Capillary dropout advances toward the FAZ
- FAZ enlargement on OCT-A is the earliest sign of ischemic maculopathy
- FAZ >0.6 mm → high risk of irreversible central vision loss
- Even if clinical inflammation is controlled, enlarged FAZ predicts poor final VA
6.3 Why CME Is the Leading Cause of VA Loss
- The macular capillaries form a dense double-ring perifoveal network (inner and outer plexuses)
- Tight junction disruption from inflammatory cytokines → leakage into Henle's fiber layer (OPL) and inner nuclear layer
- Müller cells cannot adequately reabsorb fluid under sustained inflammatory stress
- Fluid accumulates in petaloid cystic spaces → distorts photoreceptor-bipolar synapses at OPL
- The photoreceptors themselves are pushed away from RPE → outer segment ischemia even without choroidal involvement
OCT appearance of CME:
- Cystoid intraretinal fluid (IR fluid) in OPL and INL
- Petaloid pattern on cross-section
- Subretinal fluid if severe (oBRB secondary failure)
- Ellipsoid zone disruption in chronic CME = photoreceptor death = poor visual prognosis
6.4 Why Cotton Wool Spots = Ischemia (Not Exudates)
Cotton wool spots are swollen nerve fiber layer axons (cytoid bodies) caused by axoplasmic flow stasis at a point of local ischemia. They represent infarcts of the NFL/GCL.
Mechanistically:
- Arteriolar occlusion by vasculitic thrombus or fibrin plug
- Ischemia in capillary-free zone around arteriole (see anatomy above)
- Rapid axoplasmic transport depends on local ATP → halts within hours of ischemia
- Swollen axons appear white on fundoscopy
- Disappear in 4-6 weeks as the axons degenerate
Clinical implication: The presence of cotton wool spots in retinal vasculitis = arterial (arteriolar) component is involved. Isolated periphlebitis does not cause CWS. Seeing CWS in Behçet or SLE = more severe, ischemic disease.
6.5 Why Neovascularization Occurs and Why It Destroys Vision
- Ischemic retina → HIF-1α (hypoxia-inducible factor) → massive VEGF upregulation
- VEGF acts on retinal endothelium → new vessel sprouting (NVE = neovascularization elsewhere, NVD = at disc)
- New vessels are abnormal: no tight junctions → profuse leakage (explains late leakage on FFA)
- New vessels grow into the vitreous space along posterior hyaloid face
- Posterior vitreous detachment → fibrovascular frond traction → vitreous hemorrhage
- Progressive fibrous proliferation → sheets over retina → tractional retinal detachment
Why PRP (laser) works:
- Destroys ischemic peripheral retina → eliminates VEGF source
- Remaining perfused retina receives better oxygen supply
- Neovascular regression occurs in ~80% (Eales Stage III-IV)
6.6 Why Widefield FFA Detects More Disease
- Standard 7-field FFA covers ~60° of fundus
- Widefield (Optos/Heidelberg) covers 200° in one image
- Peripheral retina is where early periphlebitis and NPA begin in Eales, TB, sickle cell, MS
- The peripheral capillary bed is supplied by the most terminal arteriolar branches → first to fail in inflammatory occlusive disease
- 30-50% more non-perfusion area detected with widefield imaging → changes management decisions regarding PRP timing
6.7 Anatomy of Arteriovenous Crossings and BRVO
At AV crossings, the artery and vein share a common adventitial sheath. In inflammatory vasculitis:
- Arterial wall inflammation spreads to the vein through this shared sheath
-
- Venous endothelial turbulence at the crossing
-
- Hypercoagulable state from systemic inflammation → Branch retinal vein occlusion (BRVO)
This is distinct from atherosclerotic BRVO (where the artery compresses the vein mechanically) but the final result - venous occlusion, hemorrhage, edema, ischemia - is identical.
6.8 Why Optic Disc Hyperfluorescence Matters
The optic disc has:
- Capillaries derived from the posterior ciliary arteries (Zinn-Haller ring) + CRA branches
- A fenestrated capillary bed on the disc surface
- No BRB at the disc → fluorescein normally leaks slightly (disc staining normal late)
In active vasculitis:
- Peripapillary capillary inflammation → early disc hyperfluorescence (not late leakage alone)
- Disc edema from axonal ischemia
- In Behçet: disc vasculitis with necrosis → very poor prognosis
On FFA: disc hyperfluorescence + vascular leakage = the two most sensitive markers of active vasculitis
PART 7 - VISUAL PATHWAY ANATOMY (Connecting Retina to Brain)
The reason retinal vasculitis can mimic neurological disease:
Photoreceptors (retina)
↓ (via bipolar cells → ganglion cells)
Optic nerve (CN II) → optic chiasm
↓
Optic tract → Lateral Geniculate Nucleus (LGN)
↓
Optic radiations (Meyer's loop anteriorly,
Baum's loop posteriorly)
↓
Primary Visual Cortex (V1) - striate cortex, occipital pole
Nasal fibres decussate at the chiasm → lesions anterior to chiasm = ipsilateral visual field defect; at chiasm = bitemporal hemianopia; posterior = homonymous hemianopia.
Applied to vasculitis:
- Optic neuritis in MS-related vasculitis = demyelination of optic nerve = RAPD
- Severe disc vasculitis (Behçet) = optic atrophy = permanent field defect
- Sectoral NPA from BRVO = corresponding scotoma mapped on visual field testing
Summary: Anatomy-Physiology-Vasculitis Integration Table
| Anatomical Structure | Normal Function | What Happens in Vasculitis | Clinical Sign |
|---|---|---|---|
| Retinal capillary endothelium (tight junctions) | Inner BRB - barrier function | Tight junction disruption by TNF-α/VEGF | CME, fluorescein leakage on FFA |
| Pericytes | Autoregulation, BRB support | Early loss → dysregulated blood flow, microaneurysms | Aneurysmal dilatations (IRVAN) |
| Retinal arterioles | Autoregulation, end-artery supply | Vasculitic thrombus → occlusion | Cotton wool spots, BRAO |
| Retinal veins | Drainage; AV crossing shared sheath | Perivenous inflammation → periphlebitis, BRVO | Sheathing, hemorrhages, disc edema |
| FAZ (capillary-free zone) | Avascular diffusion to fovea | Capillary dropout advances to FAZ | FAZ enlargement on OCT-A, central VA loss |
| Müller cells (ILM to OLM) | Metabolic support, K⁺ buffering | Overwhelmed by cytokines → fail to reabsorb fluid | Amplified CME |
| Photoreceptors (ONL, outer 1/3) | Light transduction | NOT directly supplied by retinal vessels - Choroid dependent | Preserved until choroidal/RPE involvement |
| RPE (outer BRB, visual cycle) | Recycles retinal, immunosuppression | Secondary disruption in severe disease | Subretinal fluid, RPE window defects on FFA |
| NFL / GCL | Axonal conduit to optic nerve | Ischemic infarction → axoplasmic stasis | Cotton wool spots; later optic atrophy |
| Optic disc vasculature | Disc nutrition via posterior ciliary + CRA | Disc vasculitis → ischemia | Disc hyperfluorescence (earliest FFA sign), optic atrophy |
Sources: Guyton & Hall Medical Physiology (pp. 632-648); Kanski's Clinical Ophthalmology 10th Ed. (pp. 2506-2510, 7474-7494); Costanzo Physiology 7th Ed. (pp. 2715-2725); Junqueira's Basic Histology 17th Ed.; Firestein & Kelley's Textbook of Rheumatology; Robbins, Cotran & Kumar Pathologic Basis of Disease (pp. 1840-1848)
This is a shared conversation. Sign in to Orris to start your own chat.