Give me clinical related to brest
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"breast cancer"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive clinical information on breast cancer. Let me compile a thorough, well-organized answer.
Breast Cancer - Clinical Overview
1. Epidemiology & Screening
Breast cancer is the most common cancer in females worldwide. Key screening points:
- Mammography reduces breast cancer mortality by 15-30% in large trials
- The USPSTF recommends biennial mammography for women aged 50-74 years; the decision to screen women aged 40-49 should be individualized
- The average size of invasive carcinoma detected by mammography is ~1 cm (smaller than those detected by palpation)
- Approximately 10% of invasive carcinomas are not visible on standard 2D mammography - digital breast tomosynthesis, ultrasound, and MRI serve as adjuncts
- Breast self-examination does not improve outcomes
- BRCA1/BRCA2 screening: Recommended only for women with family history of breast, ovarian, tubal, or peritoneal cancer (by risk-assessment tool first, then genetic counseling if positive)
(Goldman-Cecil Medicine, 9780323930345)
2. Risk Factors
| Risk Factor | Relative Risk |
|---|---|
| Female sex | >4.0 |
| Germline mutations (high penetrance e.g., BRCA1/2) | >4.0 |
| Strong family history (>1 first-degree relative) | >4.0 |
| Personal history of breast cancer | >4.0 |
| High breast density | >4.0 |
| Germline mutations (moderate penetrance) | 2.1-4.0 |
| High-dose chest radiation at young age | 2.1-4.0 |
| Early menarche (<12 yrs), late menopause (>55 yrs) | 1.1-2.0 |
| Late first pregnancy (>35 yrs), nulliparity | 1.1-2.0 |
| Exogenous hormone therapy | 1.1-2.0 |
| Postmenopausal obesity, alcohol consumption | 1.1-2.0 |
~20% of breast cancers are attributable to modifiable risk factors.
(Robbins & Cotran Pathologic Basis of Disease, 9780443264528)
3. Classification
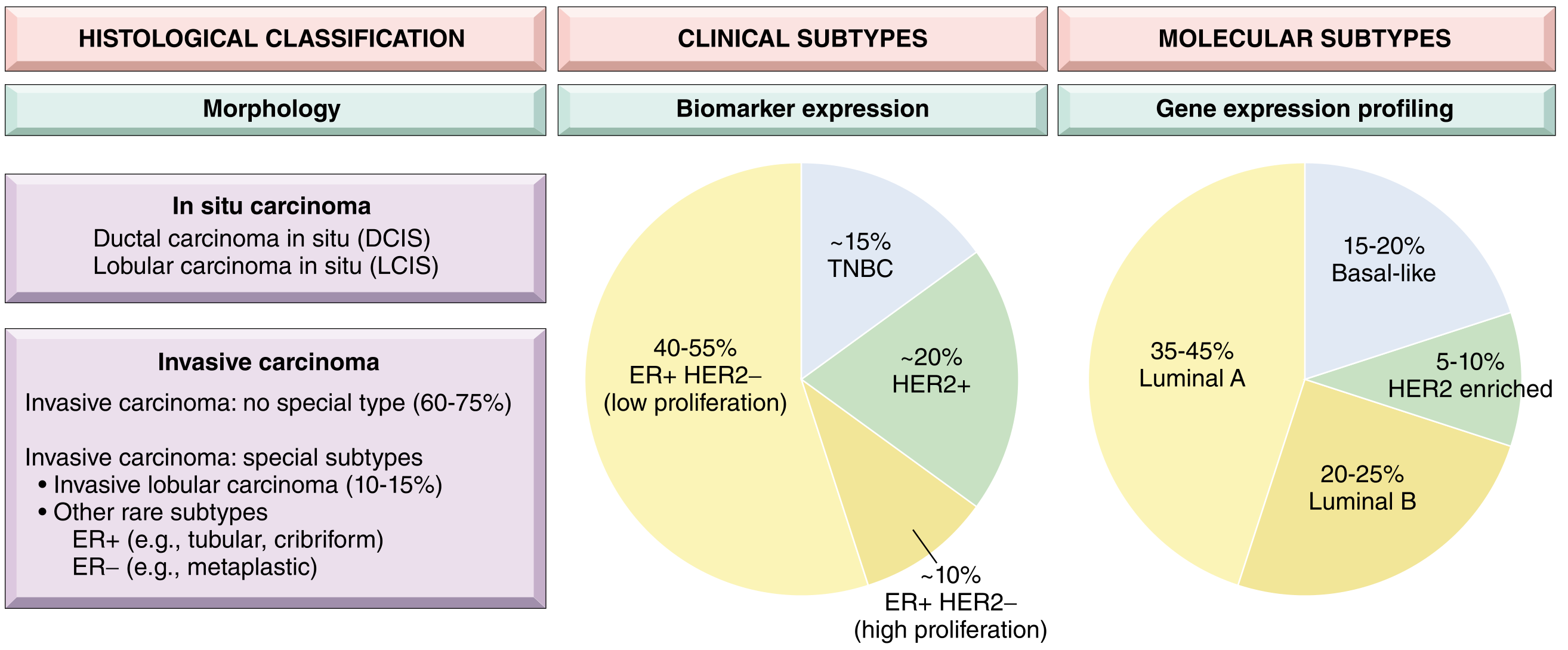
Fig. 23.15 - Robbins & Cotran Pathologic Basis of Disease
Histological Classification
In situ carcinoma:
- DCIS (Ductal Carcinoma In Situ)
- LCIS (Lobular Carcinoma In Situ)
Invasive carcinoma:
- Invasive carcinoma of no special type (NST) - 60-75%
- Invasive lobular carcinoma - 10-15%
- Special subtypes: tubular, cribriform, metaplastic, mucinous
Molecular/Intrinsic Subtypes (by IHC)
| Intrinsic Subtype | IHC Profile | Clinical Classification | Prevalence |
|---|---|---|---|
| Luminal A | ER+, PR+, HER2-, Ki-67 low | HR-positive | 35-45% |
| Luminal B | ER+, PR+/-, HER2+/-, Ki-67 high | HR-positive (±HER2+) | 20-25% |
| HER2-enriched | ER-, PR-, HER2+ | HER2-positive | 5-10% |
| Basal-like | ER-, PR-, HER2- | Triple-negative (TNBC) | 15-20% |
| Normal-like | ER+, PR+, HER2- | HR-positive | ~5% |
HR-positive tumors (ER and/or PR ≥1%) comprise ~70% of all breast cancers.
(Current Surgical Therapy 14e, 9780323796835)
4. TNM Staging (AJCC/UICC 8th Edition)
T - Primary Tumor
| Stage | Size |
|---|---|
| Tis | Carcinoma in situ |
| T1 | ≤20 mm (T1mi <1mm, T1a 1-5mm, T1b 5-10mm, T1c 10-20mm) |
| T2 | >20-50 mm |
| T3 | >50 mm |
| T4 | Any size with extension to chest wall/skin; T4d = inflammatory carcinoma |
N - Regional Nodes
| Stage | Nodes |
|---|---|
| N0 | No regional nodes positive |
| N1 | 1-3 axillary or internal mammary nodes (N1mi >0.2-2mm) |
| N2 | 4-9 axillary nodes OR internal mammary nodes without axillary |
| N3 | ≥10 axillary nodes, or infra/supraclavicular, or combined axillary + internal mammary |
M - Distant Metastasis
| Stage | Status |
|---|---|
| M0 | No distant metastasis |
| M1 | Distant metastasis present |
(Fischer's Mastery of Surgery 8th ed., 9781975176433)
5. Pathogenesis
- 25-35% of breast cancers occur due to inherited susceptibility genes
- BRCA1 and BRCA2 mutations account for 80-90% of single-gene familial breast cancers and 3-6% of all breast cancers
- Most female BRCA carriers develop breast cancer by age 70
- BRCA1/2 mutations also increase risk for ovarian, prostate, and pancreatic cancer
- Two major pathways of breast cancer evolution:
- Low-grade pathway: ER+/HER2- tumors, via flat epithelial atypia → atypical hyperplasia → low-grade DCIS → invasive cancer
- High-grade pathway: More complex, includes TNBC and HER2+ tumors
(Robbins & Cotran Pathologic Basis of Disease, 9780443264528)
6. Treatment by Subtype
HR-Positive (ER/PR+) - ~70% of cases
Endocrine therapy is the backbone:
- Tamoxifen (SERM) - competitive ER antagonist; used in pre- and post-menopausal women; 5 years of adjuvant therapy reduces 15-year recurrence and mortality; watch for endometrial cancer and thromboembolic events
- Aromatase inhibitors (AIs) - anastrozole, letrozole, exemestane; preferred for postmenopausal women; risk of osteoporosis/arthralgias; no endometrial cancer risk
- CDK 4/6 inhibitors (e.g., palbociclib, ribociclib, abemaciclib) - combined with AIs in metastatic/advanced disease
- PI3K inhibitors (in PIK3CA-mutated tumors)
- mTOR inhibitors (e.g., everolimus)
- PARP inhibitors - in patients with germline BRCA1/2 mutations
HER2-Positive - ~20% of cases
- HER2 monoclonal antibodies - trastuzumab, pertuzumab
- Antibody-drug conjugates - trastuzumab emtansine (T-DM1), trastuzumab deruxtecan (T-DXd)
- Tyrosine kinase inhibitors - lapatinib, tucatinib, neratinib
Triple-Negative Breast Cancer (TNBC) - ~15%
- Most aggressive subtype; no hormone or HER2 targets
- Immune checkpoint inhibitors (pembrolizumab + chemotherapy for PD-L1+)
- PARP inhibitors (olaparib, talazoparib) in BRCA1/2 mutation carriers
- Trop2 antibody-drug conjugate (sacituzumab govitecan)
| Subtype | Targeted Therapies |
|---|---|
| HR-positive | SERMs, AIs, SERDs, CDK 4/6 inhibitors, PI3K inhibitors, mTOR inhibitors, PARP inhibitors |
| HER2-positive | HER2 antibodies, ADCs, TKIs |
| TNBC | Immune checkpoint inhibitors, PARP inhibitors, Trop2 ADC |
(Current Surgical Therapy 14e, 9780323796835)
7. Surgical Principles
- Breast conservation (lumpectomy + radiation) is preferred over mastectomy when feasible - shown in landmark 1970s trials to be equivalent or superior to radical mastectomy
- Axillary staging is essential: sentinel lymph node biopsy (SLNB) is the standard for clinically node-negative patients
- Mastectomy options: total/simple, modified radical, skin/nipple-sparing (with reconstruction)
- Post-neoadjuvant therapy: residual disease is staged as ypT/ypN
8. Key Clinical Points to Remember
- Molecular subtype drives treatment - always assess ER, PR, HER2, Ki-67
- BRCA testing is indicated for early-onset, bilateral, or family-history cancers
- Inflammatory breast cancer (T4d) - clinical diagnosis: peau d'orange, erythema, warmth; no discrete lump; treated with neoadjuvant chemotherapy first
- Staging work-up includes CT chest/abdomen/pelvis and bone scan (or PET) for stage II-III disease
- Ovarian function suppression (OFS) combined with AIs may be used in high-risk premenopausal patients
- Extended endocrine therapy (beyond 5 years) reduces late recurrence in high-risk HR+ patients
- HER2-low (IHC 1+ or 2+/FISH-negative) is now a distinct targetable category with T-DXd
This is a shared conversation. Sign in to Orris to start your own chat.