Describe the role of respiratory centers in neural regulation of respiration. physiology topic answer in ditel
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from both Guyton & Hall and Costanzo Physiology. Let me compile a thorough, detailed answer.
Neural Regulation of Respiration: Role of Respiratory Centers
Breathing is controlled by a hierarchically organized neural system in the brainstem that generates a rhythmic motor pattern, integrates sensory feedback, and modulates output to match metabolic demands - all largely without conscious effort.
1. Overview of the Respiratory Center
The respiratory center is not a single discrete nucleus but a collection of neuron groups distributed bilaterally throughout the medulla oblongata and pons of the brainstem. It is divided into three major functional components:
| Component | Location | Primary Function |
|---|---|---|
| Dorsal Respiratory Group (DRG) | Dorsal medulla (nucleus tractus solitarius) | Inspiration & basic rhythm |
| Ventral Respiratory Group (VRG) | Ventrolateral medulla | Inspiration + active expiration |
| Pneumotaxic Center | Upper pons (nucleus parabrachialis) | Rate and depth control (switches off inspiration) |
| Apneustic Center | Lower pons | Prolongs inspiration (excites DRG) |
"The respiratory center is composed of several groups of neurons located bilaterally in the medulla oblongata and pons of the brain stem... It is divided into three major collections of neurons: (1) a dorsal respiratory group... which mainly causes inspiration; (2) a ventral respiratory group... which contains inspiratory and expiratory neurons; and (3) the pneumotaxic center... which mainly controls rate and depth of breathing."
- Guyton and Hall Textbook of Medical Physiology
2. Medullary Respiratory Centers
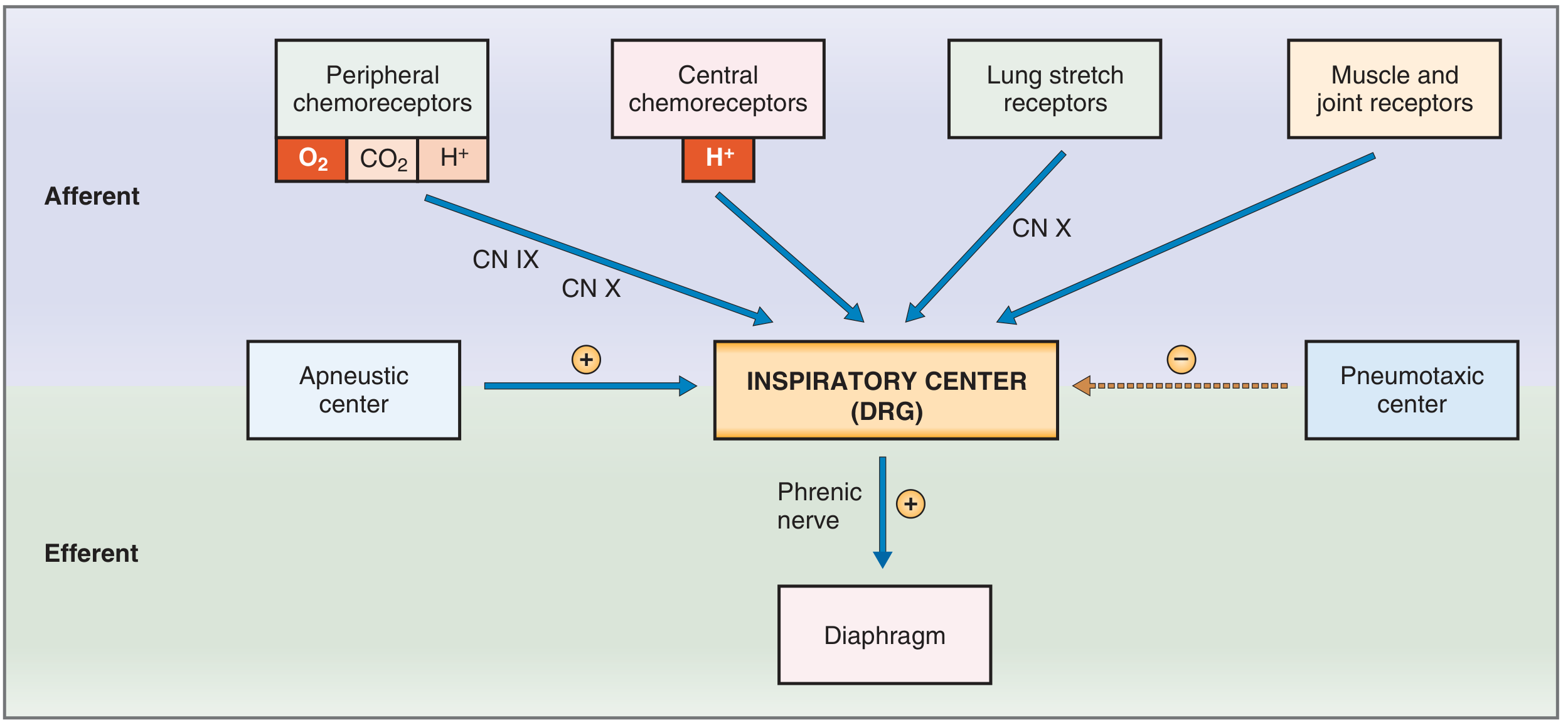
A. Dorsal Respiratory Group (DRG) - The "Inspiratory Center"
- Location: Nucleus tractus solitarius (NTS) in the dorsal medulla
- Primary role: Generates the basic rhythm of breathing (inspiratory drive) and sets the frequency of inspiration
- Motor output: Sends signals via the phrenic nerve to the diaphragm
- Sensory inputs it receives:
- Peripheral chemoreceptors (O₂, CO₂, H⁺) via CN IX (glossopharyngeal) and CN X (vagus)
- Baroreceptors, gastrointestinal and hepatic receptors via the vagus
- Lung mechanoreceptors (stretch receptors) via the vagus
Inspiratory ramp signal: The DRG does not send a simple ON/OFF signal. Instead it generates a characteristic ramp pattern of neural activity:
- A period of quiescence (expiratory pause)
- A gradually increasing burst of action potentials over ~2 seconds (inspiratory ramp) - this progressively increases diaphragm contraction until tidal volume is reached
- Sudden cessation of the ramp (abrupt switch-off), allowing passive expiration to begin
This ramp pattern produces the smooth, progressive lung filling seen in normal breathing rather than a sudden gasping contraction.
Rhythm generation - the pre-Bötzinger complex: Within the rostral portion of the VRG lies the pre-Bötzinger complex, a group of neurons with intrinsic pacemaker-like (voltage-dependent) properties. These neurons fire spontaneously and project to both the DRG and VRG, contributing to the basic respiratory rhythm. Experimental ablation of this region eliminates respiratory rhythm entirely, making it a core component of the central pattern generator (CPG) for breathing.
B. Ventral Respiratory Group (VRG) - Expiratory and Accessory Inspiratory Center
- Location: Ventrolateral medulla (nucleus ambiguus rostrally and nucleus retroambiguus caudally)
- Role: Contains both inspiratory and expiratory neurons; largely silent during quiet breathing (eupnea) since normal expiration is passive
- Activated during: Exercise, forceful breathing, high ventilation demands
Three functional subregions:
- Pre-Bötzinger complex (rostral VRG): Rhythm generator, projects to DRG and drives the inspiratory ramp
- Bötzinger complex (rostral to pre-Bötzinger): Contains inhibitory neurons that switch off inspiration and contribute to the transition from inspiration to expiration
- Caudal VRG: Sends powerful expiratory signals to intercostal and abdominal muscles during active (forced) expiration - acts as an "overdrive" mechanism during heavy exercise
The retrotrapezoid nucleus (adjacent to VRG in the rostral medulla) is a key nodal point for CO₂/H⁺ chemosensory integration, responding vigorously to local increases in PCO₂ and receiving input from the carotid bodies.
3. Pontine Respiratory Centers
A. Pneumotaxic Center (Pontine Respiratory Group)
- Location: Nucleus parabrachialis in the upper pons
- Role: Turns off (inhibits) inspiration by cutting off the inspiratory ramp signal
- Limits tidal volume (prevents over-inflation)
- Secondarily regulates respiratory rate: more frequent switch-off = faster rate
- A strong pneumotaxic signal produces rapid, shallow breathing
- A weak pneumotaxic signal allows slower, deeper breaths
When the pneumotaxic center is lesioned or absent, breathing rhythm is still present but becomes slower and deeper, with occasional apneustic breathing - confirming its role in fine-tuning the rhythm rather than generating it.
B. Apneustic Center
- Location: Lower pons
- Role: Excites the inspiratory center - prolongs the inspiratory ramp by stimulating the DRG, delaying switch-off
- When the apneustic center is stimulated experimentally, the result is apneusis: prolonged inspiratory gasps interrupted by brief expirations
- Under normal conditions, the pneumotaxic center overrides the apneustic center, preventing apneusis
Hierarchy summary:
- Apneustic center tries to keep inspiration ON
- Pneumotaxic center turns inspiration OFF
- The balance between them determines respiratory rhythm depth and rate
4. The Inspiratory-Expiratory Switching Mechanism
Normal breathing follows a cyclical pattern generated by interactions among the medullary and pontine centers:
Quiescence (expiration)
↓
DRG fires → Inspiratory ramp begins → Diaphragm contracts → Lungs inflate
↓
Pneumotaxic center fires → DRG inhibited → Ramp terminates
↓
Expiration (passive elastic recoil) → quiescence restores DRG
↓
Cycle repeats (~12-20 times/min at rest)
Additionally, as the lungs inflate, pulmonary stretch receptors in bronchial/bronchiolar walls send signals via the vagus to the DRG to stop inspiration - this is the Hering-Breuer inflation reflex. In humans, this reflex is mainly a protective mechanism activated when tidal volume exceeds ~1.5 L, preventing overdistension rather than participating in normal quiet breathing.
5. Higher Center Influences
Cerebral Cortex (Voluntary Control)
- The cerebral cortex can temporarily override the automatic brainstem centers
- Allows voluntary hyperventilation (raising RR and TV, reducing PaCO₂, raising pH) - self-limiting because the resulting hypocapnia causes unconsciousness, reverting to automatic control
- Allows voluntary breath-holding (hypoventilation) - limited by rising PaCO₂ and falling PaO₂ creating irresistible drive to breathe
Hypothalamus and Limbic System
- The hypothalamus and limbic system modify breathing in response to emotional states, fever, and thermoregulatory demands
- Anxiety or fear can trigger hyperventilation; deep sleep reduces respiratory drive
6. Chemoreceptor Integration with Respiratory Centers
Neural respiratory centers do not work in isolation - they receive critical chemical feedback:
Central Chemoreceptors
- Located on the ventral surface of the medulla, near CN IX/X exit points, close to the DRG
- Stimulus: Decreased pH of cerebrospinal fluid (CSF)
- Mechanism: CO₂ crosses the blood-brain barrier (BBB) freely; H⁺ and HCO₃⁻ do not. CO₂ enters CSF and is hydrated to H⁺ + HCO₃⁻. The resulting fall in CSF pH is detected by central chemoreceptors, which signal the DRG to increase respiratory rate (hyperventilation)
- Goal: Maintain PaCO₂ within the normal range (35-45 mmHg)
- CO₂/H⁺ is the dominant minute-to-minute controller of breathing
Peripheral Chemoreceptors
- Carotid bodies: Located at bifurcation of common carotid arteries; afferent signals via Hering's nerve → CN IX → DRG
- Aortic bodies: Along aortic arch; afferents via CN X → DRG
- Stimuli: Primarily low PaO₂ (<70 mmHg); also elevated PCO₂ and H⁺
- Role: Respond when O₂ falls dangerously low - serve as the "backup" system for hypoxic drive to breathe
- O₂ has virtually no direct effect on the medullary respiratory center itself - it acts exclusively through peripheral chemoreceptors
Why CO₂ dominates over O₂ in respiratory control: Due to the hemoglobin-O₂ dissociation curve, tissues receive near-normal O₂ delivery across a wide range of PaO₂ (60-1000 mmHg). Tissue PCO₂, however, changes directly and inversely with ventilation rate, making CO₂ a far more precise and responsive feedback signal.
7. Reflex Inputs to Respiratory Centers
| Receptor | Location | Nerve | Stimulus | Effect on Respiration |
|---|---|---|---|---|
| Pulmonary stretch receptors | Bronchi/bronchioles | Vagus (CN X) | Lung inflation | Stops inspiration (Hering-Breuer reflex) |
| Irritant receptors | Airway epithelium | Vagus | Dust, smoke, chemicals | Cough, bronchoconstriction |
| J (juxtacapillary) receptors | Alveolar walls | Vagus | Pulmonary edema, emboli | Rapid shallow breathing |
| Muscle/joint proprioceptors | Limb muscles & joints | Spinal afferents | Exercise, movement | Immediate increase in ventilation at exercise onset |
| Baroreceptors | Aortic arch/carotid sinus | CN IX/X | High blood pressure | Mild respiratory inhibition |
8. Clinical Significance
- Cheyne-Stokes breathing: Alternating hyperpnea and apnea, seen in heart failure/brain injury; results from instability in the CO₂ feedback loop to medullary centers
- Central apnea: Loss of automatic respiratory drive from medullary dysfunction (stroke, opioids, severe acidosis)
- Ondine's curse (congenital central hypoventilation): Failure of automatic breathing during sleep due to brainstem respiratory center dysfunction
- Apneusis: Sustained inspiratory spasm from pontine lesions (removing pneumotaxic inhibition)
- Opioid-induced respiratory depression: Mu-receptor agonists suppress DRG activity, reducing respiratory rate and tidal volume
Summary Diagram of Regulatory Hierarchy
CEREBRAL CORTEX
↓ (voluntary override)
PONS: Pneumotaxic Center (inhibits DRG) ←→ Apneustic Center (excites DRG)
↓
MEDULLA: DRG (Inspiratory Center / rhythm generator)
↕ pre-Bötzinger complex
VRG (Expiratory center - active during exercise)
↓
Phrenic nerve → Diaphragm
Intercostal nerves → Intercostal muscles
SENSORY INPUTS TO DRG:
- Central chemoreceptors (CO₂/pH via CSF)
- Peripheral chemoreceptors (O₂, CO₂, pH via CN IX/X)
- Lung stretch receptors (Hering-Breuer, via CN X)
- Muscle/joint receptors (exercise drive)
Sources:
- Guyton and Hall Textbook of Medical Physiology - Chapter 42: Regulation of Respiration
- Costanzo Physiology, 7th Edition - Chapter 5: Respiratory Physiology (pp. 239-241)
This is a shared conversation. Sign in to Orris to start your own chat.