Hormones of reproductive system
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks to write a thorough answer. Let me compile it.
Hormones of the Reproductive System
The reproductive system is regulated by a multi-tier hormonal hierarchy: the hypothalamus, the anterior pituitary, the gonads, and (during pregnancy) the placenta. Both sexes share the same central control axis but diverge at the gonadal level.
1. The Hypothalamic-Pituitary-Gonadal (HPG) Axis
The HPG axis is the master regulator of reproduction in both males and females. It controls two core functions: (1) production of gametes, and (2) gonadal sex steroid biosynthesis.
- Medical Physiology, p. 1594
2. Hypothalamic Hormone
Gonadotropin-Releasing Hormone (GnRH)
| Feature | Detail |
|---|---|
| Structure | Decapeptide (10 amino acids); encoded on chromosome 8 |
| Origin | Neurons in the arcuate nucleus and preoptic area of the hypothalamus; embryologically derived from the olfactory placode |
| Route | Secreted at the median eminence → travels via the hypothalamic-pituitary portal system to the anterior pituitary |
| Target | Gonadotroph cells of the anterior pituitary |
| Half-life | 2-4 minutes (rapid proteolytic cleavage) |
Pulsatile secretion is essential. Continuous GnRH exposure causes receptor downregulation and stops gonadotropin release. Pulsatile exposure upregulates GnRH receptors ("autoprime" effect) and drives FSH and LH secretion. GnRH is unique among releasing hormones in that it simultaneously regulates both FSH and LH.
Pulse patterns vary across the menstrual cycle:
- Follicular phase: frequent, small-amplitude pulses
- Late follicular phase: increased frequency and amplitude
- Luteal phase: slower frequency, higher amplitude, progressively declining
Slower pulse frequency preferentially favors FSH over LH - important for FSH availability in the late luteal/early follicular transition.
The precursor protein (92 amino acids) also yields GnRH-Associated Peptide (GAP), which inhibits prolactin secretion and stimulates gonadotropin release.
- Berek & Novak's Gynecology, pp. 270-271
3. Anterior Pituitary Gonadotropins
Follicle-Stimulating Hormone (FSH)
| Feature | Detail |
|---|---|
| Type | Glycoprotein (alpha + beta subunit) |
| Half-life | ~4 hours (fast component), ~3 days (slow component) |
| Female targets | Granulosa cells of ovarian follicles |
| Male targets | Sertoli cells of the testes |
Actions in females:
- Recruits a cohort of ovarian follicles at the start of each cycle
- Drives estradiol synthesis by granulosa cells (via the two-cell, two-gonadotropin model)
- Stimulates inhibin B production
Actions in males:
- Acts on Sertoli cells to produce androgen-binding protein (ABP), aromatase, growth factors, and inhibin
- Supports spermatogenesis
- Increases LH receptor numbers on Leydig cells (via growth factors), amplifying testosterone production
Luteinizing Hormone (LH)
| Feature | Detail |
|---|---|
| Half-life | Fast component ~40 min; slow component ~120 min |
| Female targets | Theca cells and granulosa cells |
| Male targets | Leydig cells |
Actions in females:
- Stimulates androgen (androstenedione) synthesis in theca cells
- Triggers ovulation (the midcycle LH surge, 24-36 hours before ovulation)
- Stimulates progesterone production in luteinized granulosa cells before and after ovulation
- Maintains the corpus luteum
Actions in males:
- Stimulates Leydig cells to produce testosterone
A useful mnemonic: LH → Leydig cells; FSH → Sertoli cells.
- Medical Physiology, p. 1598
4. Gonadal Hormones - Female
Estrogens (principally 17β-Estradiol, E2)
Produced mainly by granulosa cells of developing follicles (follicular phase) and by the corpus luteum (luteal phase). Estrogen is also made from androgens via aromatase in the placenta and peripheral fat tissue.
Actions on target tissues:
| Target | Effect |
|---|---|
| Uterus | Proliferation of endometrium; increases contractility |
| Fallopian tubes | Stimulates ciliary activity and motility |
| Vagina | Proliferation of epithelial cells |
| Breasts | Development of duct tissue |
| Granulosa cells | Promotes proliferation |
| Receptors | Up-regulates estrogen, progesterone, and LH receptors |
| Pituitary | Negative feedback (most of cycle) → positive feedback (late follicular, triggering LH surge) |
| Bone | Anti-osteoporosis; contributes to epiphyseal closure at puberty |
| Lipids | Decreases LDL cholesterol |
| Secondary sex characteristics | Pubic/axillary hair, breast development, female fat distribution |
| Prolactin | Stimulates secretion but blocks its action at the breast (until parturition) |
Estrogen also prepares target tissues for progesterone by up-regulating progesterone receptors. Without prior estrogenic stimulation, progesterone has little biological activity.
Progesterone
Produced by luteinized granulosa cells/corpus luteum in the luteal phase; main source in pregnancy shifts to the placenta after 5-6 weeks.
Actions:
| Target | Effect |
|---|---|
| Endometrium | Converts proliferative to secretory (prepares for implantation) |
| Cervical mucus | Makes it thick and impenetrable to sperm |
| Uterus | Raises threshold to contractions (anti-contractile during pregnancy) |
| Breasts | Development of alveoli and lobular tissue |
| Hypothalamus | Raises thermoregulatory set point → increases basal body temperature in luteal phase (basis of the temperature rhythm method of contraception) |
| Pituitary | Negative feedback on FSH and LH |
Progesterone also down-regulates estrogen receptors in some tissues, reducing their responsiveness to estrogen.
- Costanzo Physiology, pp. 1380-1396
Inhibin and Activin (Ovarian Peptides)
| Hormone | Source | Primary Action |
|---|---|---|
| Inhibin B | Granulosa cells (follicular phase) | Selectively suppresses FSH from pituitary |
| Inhibin A | Corpus luteum (luteal phase) | Suppresses FSH |
| Activin | Granulosa cells | Stimulates FSH release; potentiates FSH action in the ovary |
These peptides fine-tune FSH levels independently of estrogen feedback.
5. Gonadal Hormones - Male
Testosterone
Produced by Leydig cells of the testes under LH stimulation.
Effects by organ system:
| Target | Effect |
|---|---|
| Male sex organs | Growth, development, secondary sex characteristics, erections, prostatic growth |
| Spermatogenesis | Supports spermatogenesis within seminiferous tubules |
| Bone | Linear growth, closure of epiphyses, increased bone mineral density |
| Muscle | Anabolic; increases mass and possibly strength |
| Fat | Reduces body and visceral fat |
| Brain | Modulates libido, mood, memory, aggression |
| Kidney | Stimulates erythropoietin production |
| Bone marrow | Stimulates stem cell production |
| Hair | Facial/body hair patterns, temporal balding |
| Liver | Stimulates serum protein synthesis |
| Heart | Coronary vasodilation |
Testosterone can be converted to dihydrotestosterone (DHT) by 5-alpha reductase (more potent at androgen receptors) or to estradiol by aromatase (Sertoli cells and peripheral tissues).
- Smith and Tanagho's General Urology, p. 752
6. Hormonal Pattern of the Menstrual Cycle
The diagram below shows the coordinated hormonal fluctuations across a 28-day cycle:
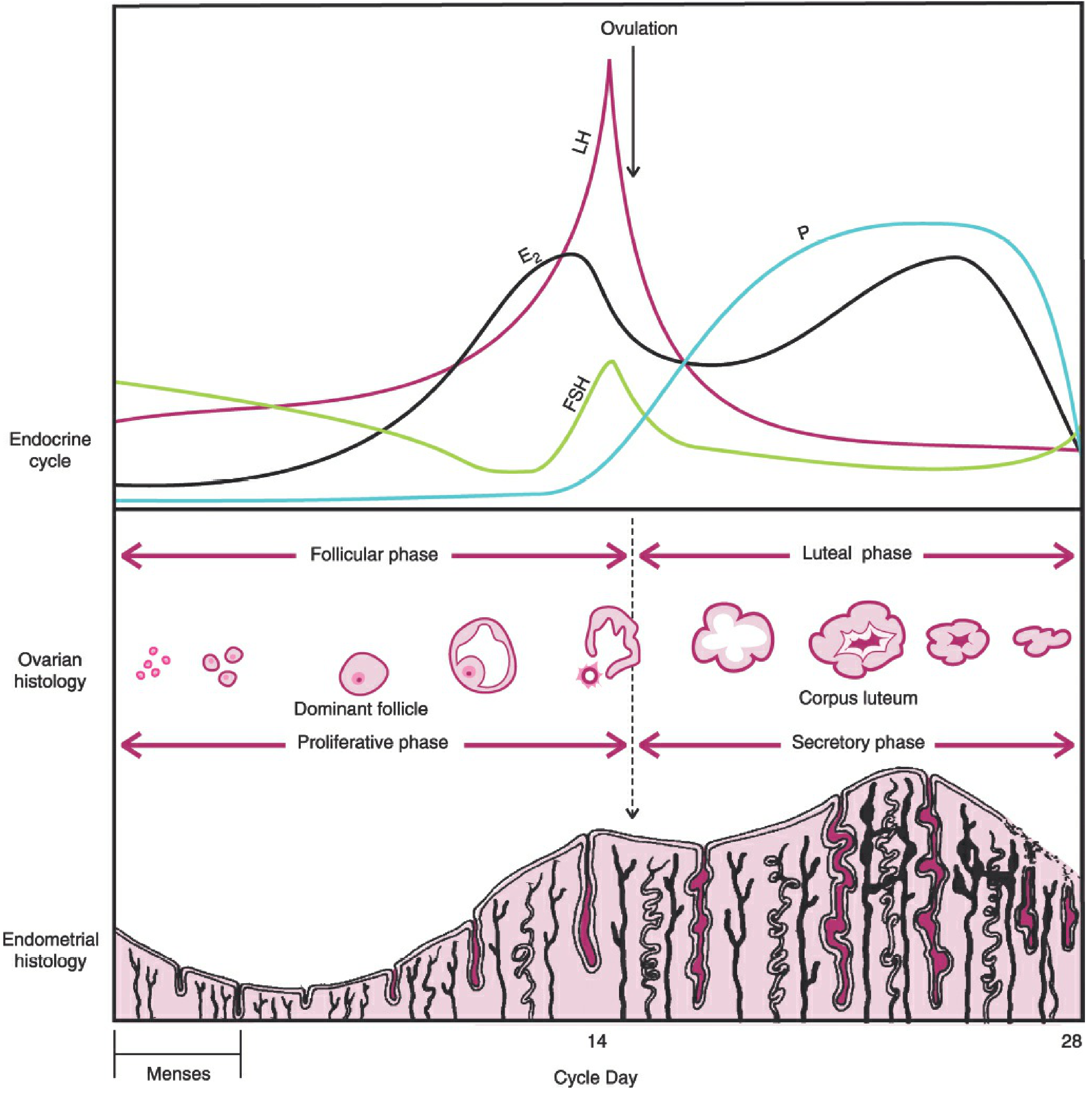
Phase-by-phase summary:
Follicular phase (Days 1-14):
- FSH rises (corpus luteum demise removes inhibin A/progesterone feedback)
- Follicles recruited; estradiol rises progressively
- Rising estradiol causes negative feedback on FSH (FSH begins to fall)
- Late follicular: estradiol burst switches to positive feedback → LH surge (and smaller FSH surge)
- Ovulation triggered 24-36 hours after LH surge
Luteal phase (Days 14-28):
-
Corpus luteum forms; secretes estradiol, progesterone, and inhibin A
-
Progesterone converts endometrium from proliferative → secretory
-
High progesterone + estrogen + inhibin A suppress FSH and LH
-
If no fertilization: corpus luteum degenerates → hormone levels fall → menstruation
-
Berek & Novak's Gynecology, pp. 359-374
7. Hormones of the Posterior Pituitary (Relevant to Reproduction)
Oxytocin
- Released by the posterior pituitary
- Stimulates uterine contractions during labor
- Drives milk ejection (let-down reflex) during breastfeeding
- Levels increase progressively near term and are amplified by estrogen (which upregulates oxytocin receptors in the myometrium)
8. Placental Hormones (Pregnancy)
Human Chorionic Gonadotropin (hCG)
| Feature | Detail |
|---|---|
| Source | Syncytiotrophoblast of placenta |
| Structure | Similar to LH (shares alpha subunit); unique beta subunit |
| Role | Rescues the corpus luteum from luteolysis; stimulates corpus luteum to continue producing progesterone to maintain the endometrium until the placenta takes over (~5-6 weeks) |
| Clinical use | Basis of pregnancy tests (detectable in urine from ~8-10 days post-implantation) |
| Fetal effect | Stimulates testosterone in fetal Leydig cells (male sexual differentiation) |
Human Placental Lactogen (hPL / Chorionic Somatomammotropin)
- Promotes mammary gland preparation for lactation
- Antagonizes insulin → raises maternal blood glucose (ensures fetal glucose supply)
Placental Progesterone
- After 5-6 weeks, the placenta takes over progesterone synthesis independently
- Inhibits uterine contractions, maintains decidua, promotes mammary differentiation
Placental Estrogens
-
The predominant form at term is estriol (E3), synthesized from fetal DHEAS via the fetoplacental unit
-
Promotes growth of the uterus and mammary glands
-
Color Atlas of Human Anatomy - Internal Organs, pp. 610-611
Quick Reference Summary Table
| Hormone | Source | Key Actions |
|---|---|---|
| GnRH | Hypothalamus (arcuate nucleus) | Pulsatile stimulation of FSH and LH from pituitary |
| FSH | Anterior pituitary | Follicle growth (female); spermatogenesis/Sertoli cells (male) |
| LH | Anterior pituitary | Ovulation/corpus luteum (female); testosterone via Leydig cells (male) |
| Estradiol (E2) | Granulosa cells/corpus luteum/placenta | Endometrial proliferation, secondary sex characteristics, feedback on HPG |
| Progesterone | Corpus luteum/placenta | Endometrial secretory change, anti-contractile, thermogenic |
| Testosterone | Leydig cells (testes) | Spermatogenesis, secondary male sex characteristics, anabolic effects |
| Inhibin | Granulosa cells/Sertoli cells | Selective FSH suppression |
| Activin | Granulosa cells | FSH stimulation |
| hCG | Syncytiotrophoblast | Corpus luteum rescue in early pregnancy |
| Oxytocin | Posterior pituitary | Uterine contractions, milk ejection |
| hPL | Placenta | Lactation preparation, insulin antagonism |
Neuromuscular junction
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Excellent - I now have comprehensive material and two excellent diagrams. Let me compile the full answer.
Neuromuscular Junction (NMJ)
The neuromuscular junction is the specialized synapse where a motor neuron terminal meets and communicates with a skeletal muscle fiber. It is the site where an electrical signal in the nervous system is converted into a mechanical contraction in muscle.
1. Structure of the NMJ
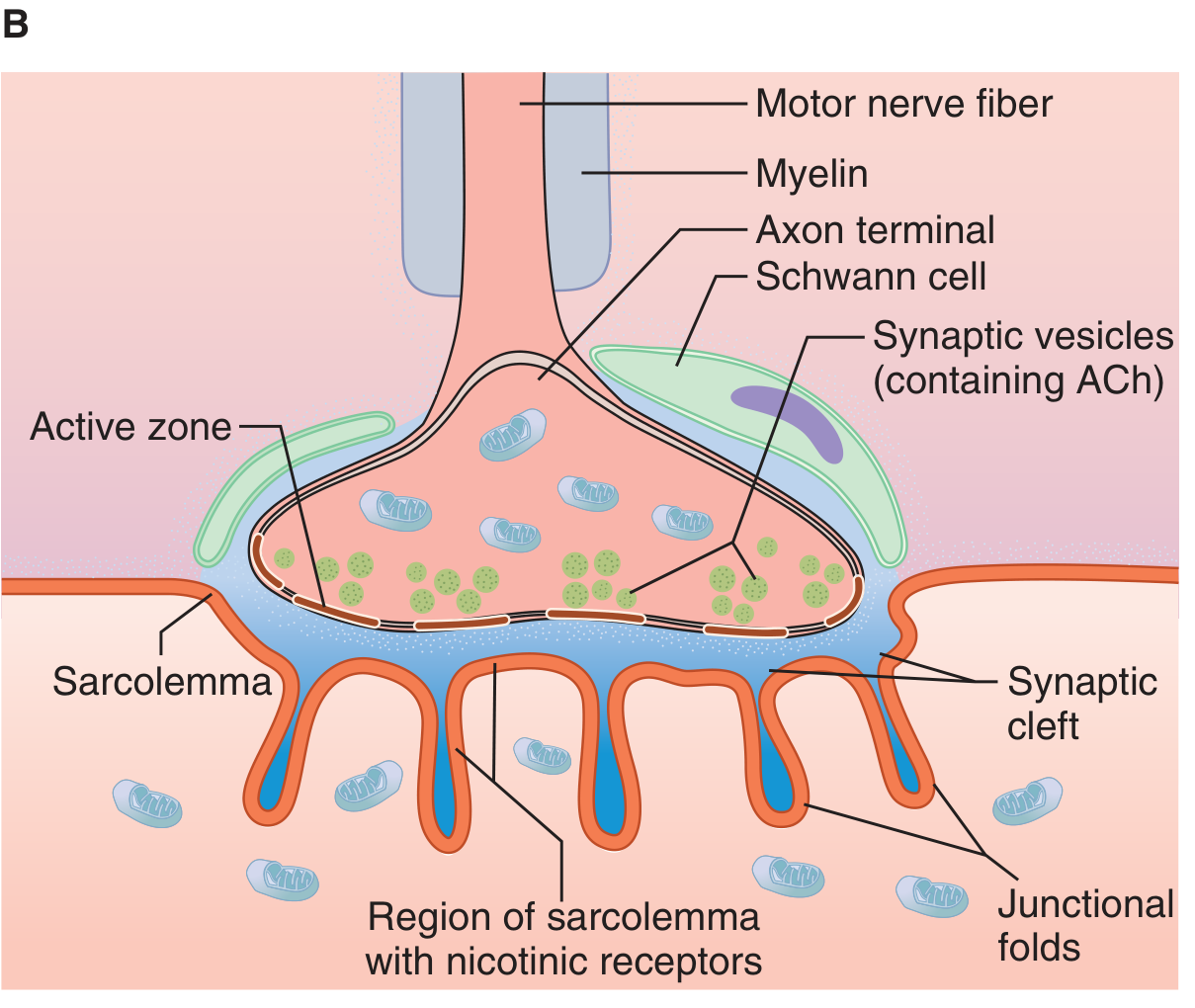
The NMJ has three main components:
Presynaptic Terminal (Motor Nerve Ending)
- As the myelinated motor axon approaches the muscle, it loses its myelin sheath and divides into several terminal boutons
- Each bouton sits in a depression on the muscle surface
- The terminal is rich in:
- Mitochondria (energy supply for ACh synthesis)
- Synaptic vesicles (each containing ~5,000 molecules of acetylcholine)
- Active zones - specialized docking sites where vesicles align for release
- Voltage-gated Ca²⁺ channels adjacent to the active zones
- SNARE proteins: synaptobrevin (VAMP), synaptophysin, synaptotagmin (Ca²⁺ sensor), synapsin
Synaptic Cleft
- The gap (~20-50 nm wide) between the nerve terminal and the motor endplate
- Filled with a proteoglycan matrix
- Contains acetylcholinesterase (AChE), anchored to the basement membrane - the enzyme that rapidly degrades ACh
Postsynaptic Membrane (Motor Endplate)
- The thickened region of the muscle sarcolemma opposite the nerve terminal
- Forms deep junctional folds that greatly increase surface area
- Concentrated at the tops of the junctional folds: nicotinic cholinergic receptors (N_M type)
- At the bottoms of the folds: voltage-gated Na⁺ channels (important for action potential propagation)
- The AChR is anchored to the membrane by rapsyn (43 kDa protein, 1:1 ratio with AChR)
Each endplate receives input from only one motor nerve fiber.
- Ganong's Review of Medical Physiology, p. 141
2. Acetylcholine - Synthesis, Storage, and Release
Synthesis:
- ACh is synthesized in the axon terminal cytoplasm from choline + acetyl-CoA via the enzyme choline acetyltransferase (ChAT)
- Acetyl-CoA is produced in mitochondria
- Choline is actively transported into the terminal from the synaptic cleft (recycled after ACh hydrolysis) - this choline reuptake is the rate-limiting step
Storage:
- Newly synthesized ACh is transported into synaptic vesicles
- Each vesicle holds ~5,000 ACh molecules along with ATP
- A single nerve impulse releases approximately 200 quanta (~1,000,000 molecules of ACh total)
Release (Quantal Theory):
-
ACh is released in discrete packets called quanta (one quantum = one vesicle's worth)
-
Even at rest, individual vesicles occasionally fuse spontaneously with the membrane, producing small spontaneous depolarizations called miniature endplate potentials (MEPPs)
-
MEPPs are the physiological signature of quantal release
-
Miller's Anesthesia, p. 1158-1160
3. Step-by-Step Transmission
The diagram below illustrates the full sequence of events:
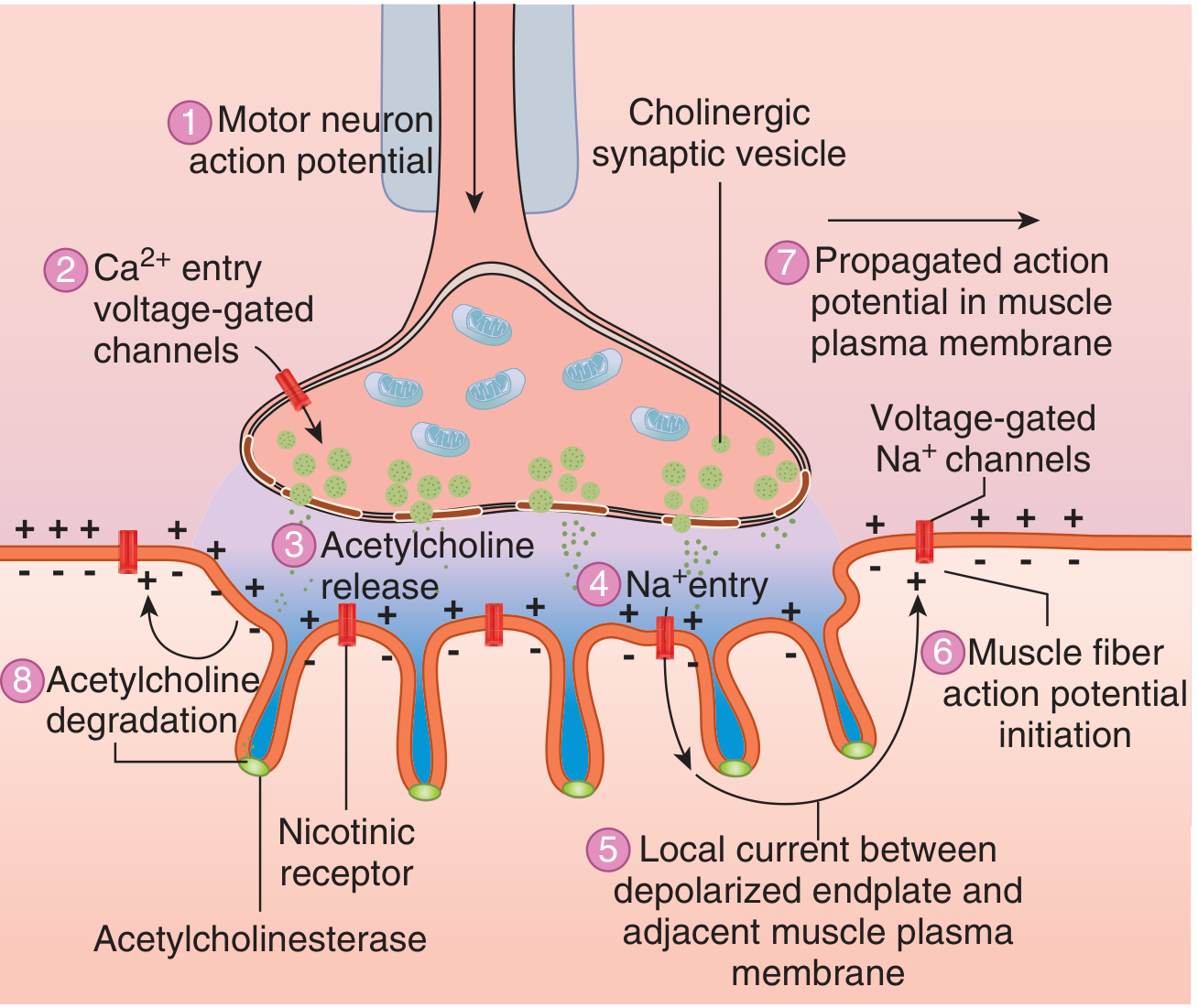
| Step | Event |
|---|---|
| 1 | Action potential arrives at the motor nerve terminal |
| 2 | Depolarization opens voltage-gated Ca²⁺ channels in the presynaptic membrane; Ca²⁺ floods in |
| 3 | Ca²⁺ binds to synaptotagmin (the Ca²⁺ sensor on vesicles), triggering SNARE-mediated vesicle fusion and ACh exocytosis into the cleft |
| 4 | ACh diffuses across the cleft and binds to nicotinic (N_M) receptors on the motor endplate; each receptor requires 2 ACh molecules (one per α-subunit) to open |
| 4 | Receptor opens its ion channel: Na⁺ rushes in, K⁺ leaves (Na⁺ influx dominates) |
| 5 | Net cation influx produces a local depolarization: the endplate potential (EPP) |
| 5 | The local current created by the EPP spreads to adjacent muscle membrane |
| 6 | Adjacent muscle membrane is depolarized to threshold → muscle fiber action potential is initiated |
| 7 | Action potential propagates along the sarcolemma and into T-tubules → excitation-contraction coupling → muscle contracts |
| 8 | ACh is rapidly hydrolyzed by acetylcholinesterase (AChE) in the cleft into acetate + choline (half-life of ACh in the cleft: ~200 μsec); choline is recycled back into the terminal |
- Ganong's Review of Medical Physiology, pp. 141-142
4. The Nicotinic ACh Receptor (nAChR)
The postjunctional (mature) nAChR is a ligand-gated ion channel with the following structure:
- Pentameric protein complex (~250 kDa): 2α₁ + β₁ + δ + ε subunits (mature/junctional type)
- Fetal/immature/extrajunctional receptor: 2α₁ + β₁ + δ + γ subunits (γ replaces ε)
- Neuronal α7 receptor: 5 × α7 subunits (found at autonomic ganglia and presynaptically)
- ACh binding sites are on each α-subunit (at cysteine residues 192-193)
- The five subunits form a barrel/cylinder arrangement around a central ion pore
- When both α-sites are occupied by ACh, the channel opens → Na⁺ in, K⁺ out → EPP
The mature and fetal receptors differ importantly:
-
Mature (junctional): clustered at endplate, shorter channel open time
-
Fetal (extrajunctional): present throughout muscle membrane in denervated/immature muscle; longer open time, more sensitive to depolarizing blockers (e.g., succinylcholine)
-
Miller's Anesthesia, pp. 1170-1171
5. Safety Margin of Transmission
The NMJ is designed with a substantial safety margin:
- Far more ACh molecules are released per impulse than needed to trigger an EPP above threshold
- Far more AChRs are available than are actually occupied during normal transmission
- Only a small fraction of vesicles and receptors are used with each nerve impulse
This redundancy means that even significant loss of receptors (as in early myasthenia gravis) may not immediately produce weakness - symptoms appear only when the safety margin is exceeded.
- Miller's Anesthesia, p. 1158
6. Vesicle Recycling
After exocytosis, vesicle membrane is retrieved by endocytosis - it invaginates back into the terminal and is recoated to form a new vesicle. The recycled vesicular membrane retains its enzyme proteins (ChAT, transport proteins) and can be refilled with ACh. This recycling allows sustained high-frequency transmission.
- Guyton & Hall Textbook of Medical Physiology, p. 574
7. Pharmacological Targets at the NMJ
| Drug/Toxin | Site of Action | Mechanism | Effect |
|---|---|---|---|
| Succinylcholine | Postjunctional nAChR | Persistent agonist (depolarizing blocker) | Muscle fasciculation → paralysis (Phase I/II block) |
| Vecuronium, rocuronium, atracurium | Postjunctional nAChR | Competitive antagonist | Non-depolarizing neuromuscular block |
| Neostigmine, pyridostigmine | AChE (synaptic cleft) | Reversible AChE inhibition → ↑ACh in cleft | Reversal of non-depolarizing block; used in myasthenia |
| Organophosphates (nerve agents) | AChE | Irreversible AChE inhibition | Sustained depolarization → paralysis, fasciculations |
| Botulinum toxin | Presynaptic SNARE proteins | Zinc metalloproteinase cleaves VAMP/SNAP-25/syntaxin → prevents vesicle fusion | Blocks ACh release → flaccid paralysis |
| Tetanus toxin | Presynaptic (spinal inhibitory neurons) | Blocks glycine/GABA release | Spastic paralysis (different target than botulinum) |
| α-Bungarotoxin (cobra) | Postjunctional nAChR | Irreversible competitive antagonist | Paralysis; used in research to label AChRs |
| Hemicholinium | Choline transporter | Blocks choline reuptake | Depletes ACh over time |
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 3496
8. Diseases of the Neuromuscular Junction
| Disease | Target | Mechanism | Features |
|---|---|---|---|
| Myasthenia Gravis | Postjunctional nAChR (α-subunit) | Autoantibodies destroy/block AChRs; complement-mediated endplate damage | Fatigable weakness (eyes, face, limbs); improves with rest; AChE inhibitors help; associated with thymoma/thymic hyperplasia |
| Lambert-Eaton Myasthenic Syndrome (LEMS) | Presynaptic voltage-gated Ca²⁺ channels | Autoantibodies reduce Ca²⁺ influx → less ACh released per impulse | Proximal limb weakness; autonomic dysfunction; strength improves with repeated activity (facilitation); associated with small cell lung cancer |
| Botulism | Presynaptic SNARE proteins | Botulinum toxin cleaves SNARE proteins → blocks ACh exocytosis | Descending flaccid paralysis, autonomic dysfunction; from C. botulinum |
| Congenital Myasthenic Syndromes | Various NMJ proteins | Genetic defects in AChR, rapsyn, ChAT, AChE | Present in infancy; no autoantibodies |
Distinguishing feature: in myasthenia gravis, repetitive stimulation causes decremental response (safety margin depleted); in LEMS, repetitive high-frequency stimulation causes incremental response (Ca²⁺ accumulates, releasing more ACh).
- Robbins & Kumar Basic Pathology, p. 755
Quick Summary
Hypothalamus (motor cortex/spinal cord)
↓ Action potential
Motor neuron axon (myelinated)
↓ Arrives at terminal bouton
Ca²⁺ entry via VGCC
↓ SNARE-mediated
ACh exocytosis (quantal, ~200 quanta/impulse)
↓ Diffuses across synaptic cleft (~200 μsec)
Binds N_M nicotinic AChR (tops of junctional folds)
↓ Ion channel opens (Na⁺ in, K⁺ out)
Endplate Potential (EPP)
↓ Local current spreads
Muscle fiber action potential (voltage-gated Na⁺ channels)
↓
Excitation-contraction coupling → Contraction
ACh hydrolyzed by AChE → choline recycled
This is a shared conversation. Sign in to Orris to start your own chat.