Discuss various modalities of enteral nutritional support. [5]
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple surgical textbooks. Here is the complete answer:
Modalities of Enteral Nutritional Support
Enteral nutrition (EN) refers to the delivery of nutrients directly into the gastrointestinal tract. It is always the preferred route over parenteral nutrition when the gut is functional, because it preserves mucosal barrier integrity, maintains immunity, prevents gut atrophy, reduces infection rates, improves wound healing, and shortens hospital stay.
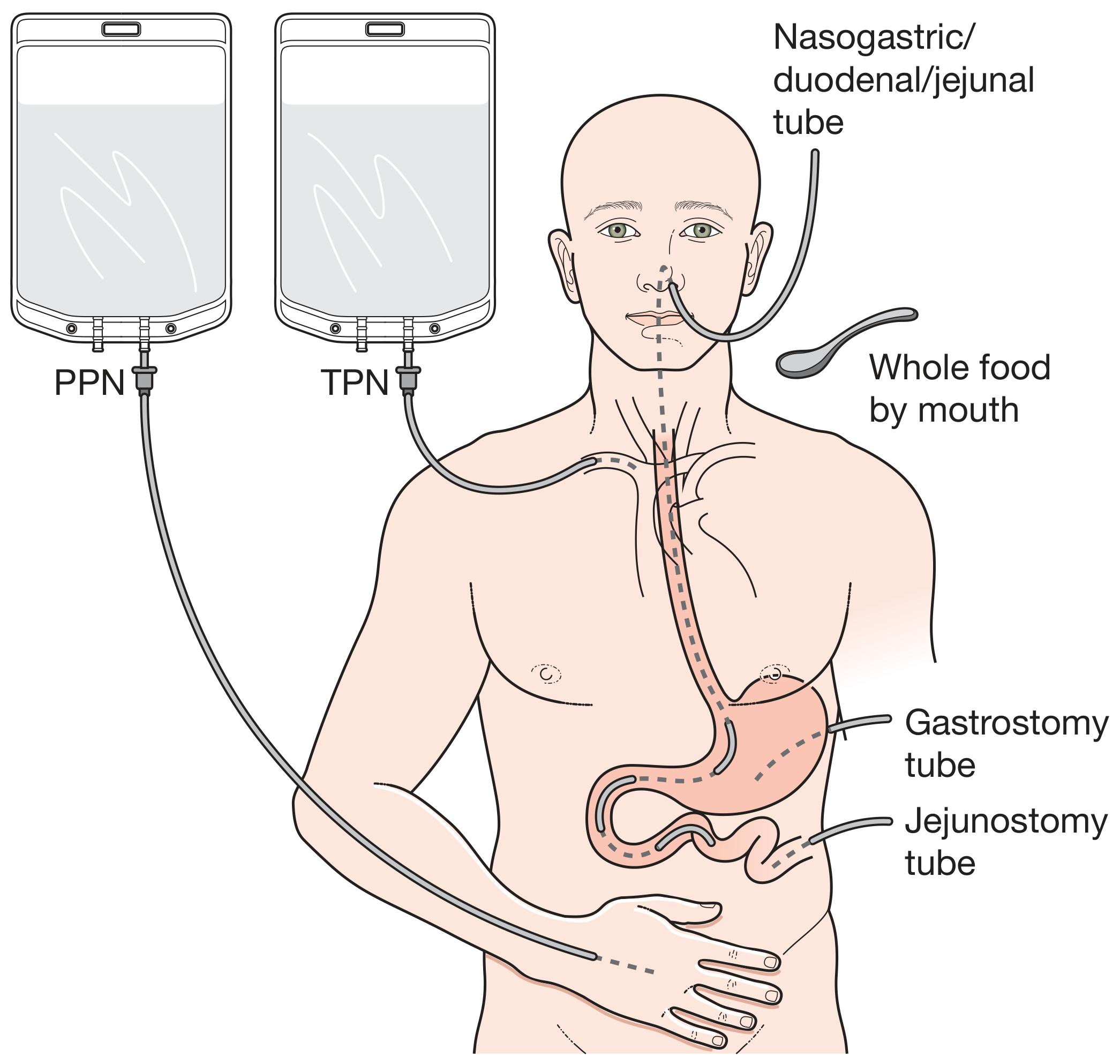
1. Oral Nutritional Supplements (ONS)
This is the simplest and most physiological form of enteral support. Commercially available liquid supplements typically supply around 200 kcal and 2 g of nitrogen per 200 mL carton. They are used to augment caloric intake beyond what diet alone provides and are particularly useful when weaning patients off tube-feeding regimens. This modality requires a patient who is conscious, cooperative, and able to swallow.
- Bailey & Love's Short Practice of Surgery, 28th Edition
2. Nasogastric Tube (NGT) Feeding
A fine-bore silicone rubber or polyurethane tube is passed through the nose into the stomach (prepyloric route).
- Conventional Ryle's tube - larger bore, used for short-term decompression and feeding
- Fine-bore nasogastric feeding tube (e.g. No. 7 French gauge, mercury-weighted tip) - more comfortable for prolonged therapy
Technique:
- Tube position must be confirmed by X-ray before commencing feeding
- Best delivered via an infusion pump (minimises blockage, ensures smoother delivery vs. bolus feeding)
- Start at half or quarter strength to minimize cramps and diarrhoea
- If the patient is severely hypoalbuminaemic, gastric emptying and absorption may be impaired - parenteral albumin replacement (100-200 mL of 25% albumin) may be needed first
- Gastric residuals ≥200 mL over 4-6 hours or abdominal distension require cessation and rate adjustment
Indications: Head injury, oropharyngeal dysfunction, neurological impairment, short-term postoperative support.
- Pye's Surgical Handicraft, 22nd Edition; Schwartz's Principles of Surgery, 11th Edition
3. Nasojejunal (NJ) Tube Feeding
A fine-bore tube is advanced beyond the pylorus into the jejunum, either endoscopically or fluoroscopically.
-
Used when gastroparesis is present (e.g. closed-head injury, critical illness) - feeding distal to the pylorus bypasses the problem of delayed gastric emptying
-
In acute pancreatitis, the nasojejunal and nasogastric routes are considered equivalent with no significant difference in adverse effects
-
Reduces risk of aspiration compared to gastric feeding in some patients
-
Schwartz's Principles of Surgery, 11th Edition; Mulholland & Greenfield's Surgery, 7th Edition
4. Percutaneous Endoscopic Gastrostomy (PEG)
A feeding tube is placed directly into the stomach through the anterior abdominal wall using a combined endoscopic/percutaneous technique, avoiding the need for general anaesthesia.
-
Indications: Patients requiring long-term (>4 weeks) enteral feeding - stroke, motor neuron disease, head and neck cancer, oesophageal obstruction, permanent neurological impairment
-
Avoids the discomfort of prolonged nasogastric intubation
-
Can be converted to a PEG-J (PEG with jejunal extension) tube to deliver feed beyond the pylorus when gastric emptying is compromised
-
Pye's Surgical Handicraft, 22nd Edition; Bailey & Love's, 28th Edition
5. Surgical Gastrostomy
Placed operatively (open or laparoscopic) when endoscopic access is not feasible (e.g. obstructing oropharyngeal or oesophageal tumours, after failed PEG). Provides long-term gastric access for feeding.
6. Needle Catheter Jejunostomy (NCJ)
A fine catheter (typically 30 cm from the duodenojejunal flexure) is inserted at the time of a laparotomy via a 10 cm submucosal tunnel, secured with a purse-string suture.
-
A contrast study on the operating table confirms catheter tip position
-
Indications: Proximal GI obstruction, high-output fistula, fragile anastomosis, major upper GI surgery
-
Particularly useful for post-operative early enteral feeding following oesophagogastric or pancreatic resections
-
Pye's Surgical Handicraft, 22nd Edition
7. Surgical / Endoscopic Feeding Jejunostomy
A larger-bore tube is placed surgically into the jejunum as a formal stoma, or via endoscopy (direct percutaneous endoscopic jejunostomy - DPEJ).
- Used for long-term feeding when gastric access is not possible (e.g. post-total gastrectomy)
- Avoids aspiration risk entirely
Continuous vs. Intermittent (Bolus) Feeding
| Feature | Continuous Enteral Feeding (CEF) | Intermittent/Bolus Feeding |
|---|---|---|
| Preferred in | Critically ill adults | Ambulatory/home patients |
| Complication rate | Lower | Higher (diarrhoea, aspiration) |
| Protein anabolism | May promote it by inhibiting breakdown | Variable |
| Practical use | ICU, post-op | Community/rehabilitation |
The standard choice in critically injured adults is continuous enteral feeding due to lower complication rates.
- Schwartz's Principles of Surgery, 11th Edition
Enteral Formulae
Feed formulations contain 1-2 kcal/mL and up to 0.6 g/mL protein. Choice depends on GI functional status:
| GI Status | Formula |
|---|---|
| Intact GI tract | Standard polymeric (complex carbohydrate + whole protein) |
| Malabsorption / IBD / short bowel | Elemental or semi-elemental (hydrolysed protein + MCT) |
| Diarrhoea | Soluble fibre-supplemented formula |
| Organ dysfunction | Disease-specific (renal, hepatic, pulmonary formulas) |
| Critical illness | Immune-modulating (glutamine, arginine, omega-3 FA) |
Practical Points
-
Enteral feeding does not require the presence of bowel sounds or passage of flatus as a prerequisite
-
Early EN (within 24-48 hours) is recommended in critically ill patients; early "full nutrition" is harmful - target >80% of estimated energy goals by day 3-4
-
Low-output enterocutaneous fistulas (<500 mL/day) are not a contraindication to enteral feeding
-
A trained dietician should plan and manage the feeding regime
-
Monitor weight daily; electrolytes and albumin twice weekly
-
Schwartz's Principles of Surgery, 11th Edition; Bailey & Love's Short Practice of Surgery, 28th Edition
Malrotation of gut. [5]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed. Here is the comprehensive answer:
Malrotation of the Gut
Definition and Embryology
Malrotation refers to failure of the normal developmental process of intestinal growth and fixation during embryonic life. Normally, the midgut herniates through the umbilical ring at ~4 weeks, undergoes counterclockwise rotation of 270° around the axis of the superior mesenteric artery (SMA) between weeks 4-10, then returns into the abdominal cavity by week 12 with the duodenum and cecum becoming fixed in their normal positions. In malrotation, this process is incomplete, resulting in:
- The duodenojejunal (DJ) junction and ileocecal junction lying abnormally close together
- A narrow mesenteric base (instead of the broad diagonal attachment from the DJ junction in the left upper quadrant to the ileocecal valve in the right lower quadrant)
- Abnormal peritoneal bands (Ladd's bands) from the cecum across the duodenum to the right peritoneum
Incidence: 1 in 200 (all anomalies); clinically apparent symptomatic malrotation ~1 in 6000 live births.
- Sabiston Textbook of Surgery, 21st Edition; Current Surgical Therapy, 14th Edition
Types / Spectrum of Rotational Anomalies
| Type | Description |
|---|---|
| Non-rotation | No rotation occurs; small bowel on right, colon on left |
| Malrotation (incomplete rotation) | Most common; DJ junction fails to reach left of midline |
| Reverse rotation | Colon lies posterior to duodenum and SMA |
| Paraduodenal hernia | Internal herniation into mesocolic fossae (left or right) |
Clinical Features
Age of presentation:
- 70% present in the first year of life; of those, ~70% in the first month
- ~90% present before 12 months; up to 1% present in adults
1. Midgut Volvulus (surgical emergency)
The narrow mesenteric base allows the entire midgut to twist around the SMA axis. This is life-threatening.
- Bilious emesis - the cardinal symptom; must always be treated as an emergency until proven otherwise
- Initially: feeding intolerance, irritability, colicky abdominal pain
- Guaiac-positive stool (early mucosal ischaemia)
- Late: progressive abdominal distension, haematemesis, hypotension
- Severe: metabolic acidosis, coagulopathy, shock, transmural midgut necrosis
A somnolent/lethargic newborn with acute onset bilious emesis is an ominous sign mandating immediate investigation.
2. Duodenal Obstruction by Ladd's Bands
Ladd's bands stretch from the malpositioned cecum across the duodenum to the right posterior abdominal wall, causing extrinsic duodenal compression:
- Bilious emesis with gastric/proximal duodenal distension
- Without the acute haemodynamic compromise of volvulus
3. Incidental / Asymptomatic
Found on contrast studies performed for other reasons; estimated ~1% of the population have rotational anomalies without symptoms.
- Mulholland & Greenfield's Surgery, 7th Edition; Sabiston Textbook of Surgery
Associated Anomalies
- Diaphragmatic hernia
- Gastroschisis / omphalocele
- Duodenal atresia
- Biliary atresia, congenital heart disease
- Intestinal atresia and stenosis
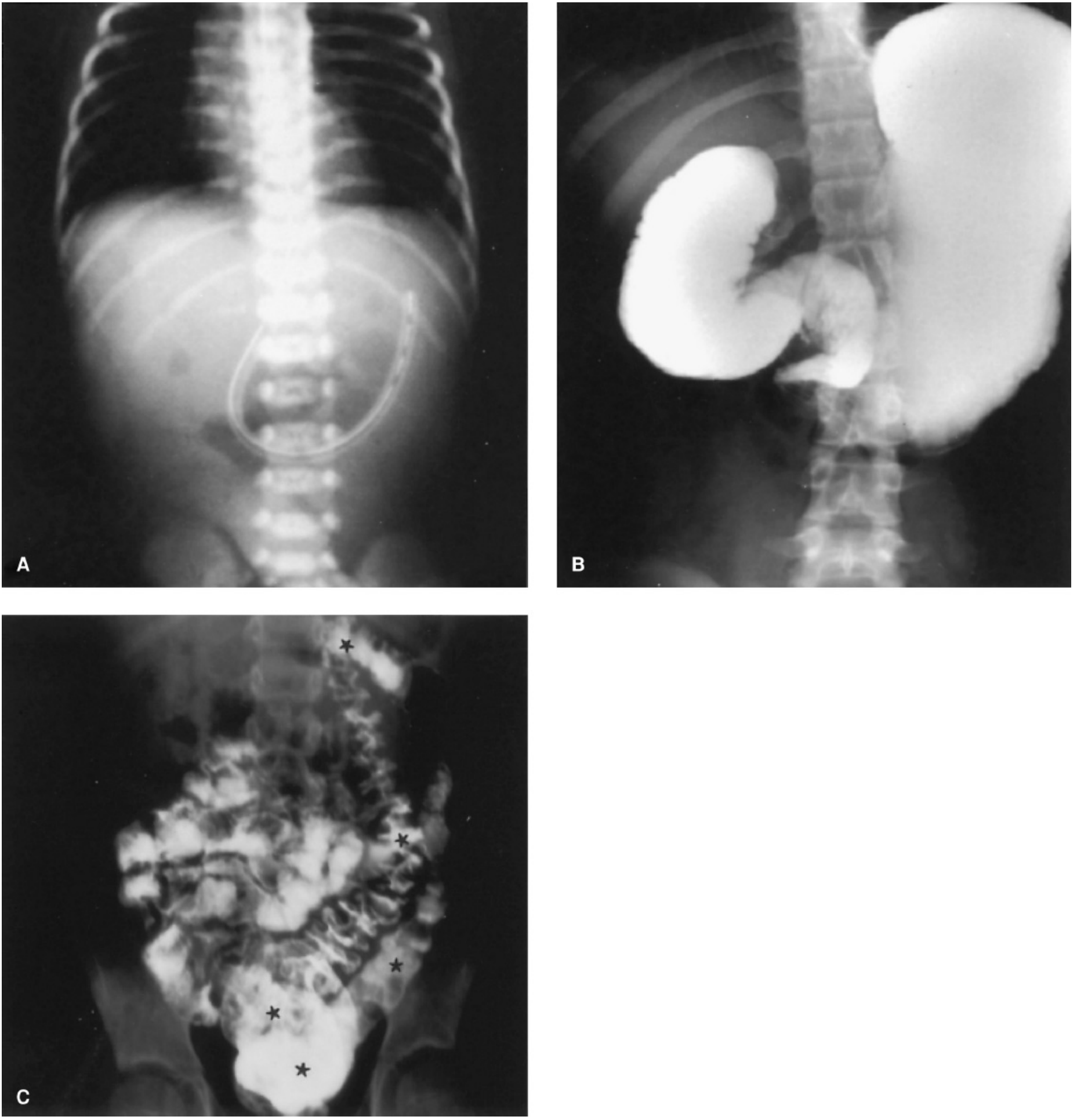
Diagnosis
Plain Abdominal Radiograph:
- Gastric and proximal duodenal distension
- Paucity or absence of distal small bowel gas (classic sign)
- Cannot exclude malrotation - a "normal bowel gas pattern" never rules it out
Upper GI Contrast Series (UGI) - investigation of choice:
Three key features used to exclude malrotation on UGI:
- Duodenum crosses to the left of the midline (using spine as landmark)
- C-loop shape - 4th part of duodenum rises to the level of the pylorus
- Retroperitoneal course toward the spine (on lateral views)
Absence of any one = abnormal UGI = warrants exploration in a symptomatic child.
- Malrotation with volvulus: corkscrew or coiled appearance in the distal duodenum
- Extrinsic duodenal compression by Ladd's bands may be visible
Contrast Enema: Shows cecal malposition (typically in left abdomen or near midline)
Ultrasound: Abnormal position of SMV - normally to the right of SMA; in malrotation it may be ventral or to the left of the SMA (inverted relationship)
Note: CT scan may identify malrotation incidentally in older children and adults, but has no role as the initial imaging study in symptomatic infants with bilious emesis.
Treatment - Ladd's Procedure
Indications: All symptomatic patients require emergency laparotomy. Asymptomatic incidentally discovered malrotation generally also warrants elective repair given the unpredictable risk of volvulus.
Steps of the Ladd Procedure (via supraumbilical transverse laparotomy):
- Detorse the volvulus - deliver the midgut and rotate counterclockwise ("turning back the hands of time") - usually 180°-360°
- Lyse Ladd's bands - divide peritoneal bands from the cecum across the duodenum to the right lower quadrant peritoneum
- Straighten the duodenum - modified Kocher maneuver with complete mobilisation, dividing all anterior, lateral, and posterior duodenal attachments
- Broaden the mesenteric base - divide peritoneal bands tethering the cecum, small bowel mesentery, mesocolon, and duodenum around the SMA base to widen the pedicle and prevent re-volvulus
- Place bowel in position of non-rotation - small bowel on the right, colon on the left
- Appendicectomy - because the appendix will lie in an atypical position after the procedure, potentially causing diagnostic confusion in future
Assess bowel viability: Any non-viable bowel must be resected. Complete midgut infarction is survivable only with total enterectomy and long-term TPN support.
Laparoscopic approach is feasible in elective/stable cases in experienced hands.
- Current Surgical Therapy, 14th Edition; Mulholland & Greenfield's Surgery, 7th Edition; Sabiston Textbook of Surgery
Outcome
- Overall survival for operated malrotation is good in the absence of midgut necrosis
- Midgut volvulus with complete infarction carries very high mortality
- Short bowel syndrome is the main long-term morbidity following extensive resection
- In adults, mortality from midgut volvulus complicating malrotation may be as high as 3% even with treatment
. Discuss the embryological principles, clinical presentation and management of small bowel malrotation. [4+3+3]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a complete, detailed, marks-specific answer. Compiling now:
Small Bowel Malrotation
Part 1: Embryological Principles [4 marks]
Normal Midgut Development
The midgut gives rise to:
- Small intestine from the duodenum (distal to the bile duct opening) through to the mid-transverse colon
- Cecum, appendix, ascending colon, and right two-thirds of transverse colon
- All supplied by the superior mesenteric artery (SMA)
Normal midgut fixation occurs in three sequential stages between weeks 5-12 of gestation, with the SMA as the axis of rotation throughout:
Stage 1 - Physiological Herniation and Initial 90° Rotation (Weeks 5-10)
At week 5, as the midgut elongates rapidly, it forms a ventral U-shaped loop that herniates into the proximal part of the umbilical cord (physiological umbilical herniation). The apex communicates with the yolk sac via the omphalomesenteric (vitello-intestinal) duct.
The midgut loop has two limbs:
- Prearterial (cranial) limb - gives rise to distal duodenum, jejunum, and proximal ileum
- Postarterial (caudal) limb - gives rise to distal ileum, cecum, appendix, and right colon
While in the hernial sac, the midgut loop undergoes the first 90° counterclockwise rotation around the SMA axis, carrying the cranial limb to the right and the caudal limb to the left.
Stage 2 - Reduction and Further 180° Rotation (Weeks 10-12)
By week 10, liver growth slows and the abdominal cavity enlarges, allowing the herniated gut to return. As the intestine re-enters the abdomen, it undergoes a further 180° counterclockwise rotation (total = 270°):
- The prearterial (cranial) segment passes posterior to the SMA; the distal duodenum ends up fixed to the left of the aorta at the ligament of Treitz
- The postarterial (caudal) segment (cecum) passes anteriorly then to the right of the SMA
- The jejuno-ileal loops undergo dramatic elongation forming ~6 primary intestinal loops, filling the right side of the abdomen
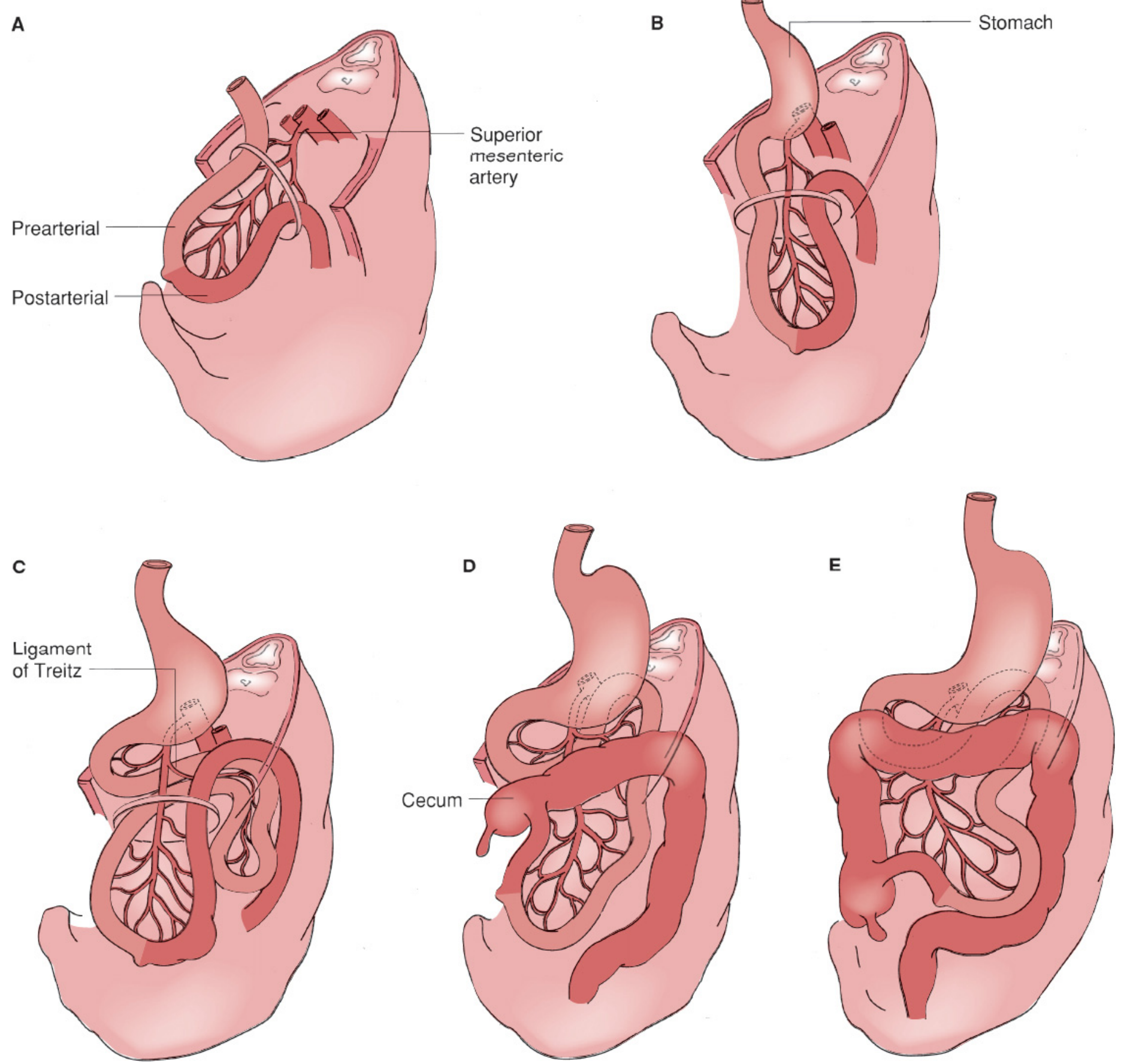
Stage 3 - Fixation (After Week 12)
The intestine becomes fixed to the posterior abdominal wall:
- Cecum descends to the right iliac fossa
- Duodenojejunal (DJ) junction is fixed at the ligament of Treitz - to the left of the aorta, anterior to the left renal vein, at the level of L1/L2
- The mesentery acquires a broad oblique base running from the DJ junction (left upper quadrant) diagonally to the ileocecal valve (right lower quadrant)
- This wide mesenteric attachment is what prevents volvulus
Pathogenesis of Malrotation
Failure of this 270° rotation and fixation results in:
| Abnormality | Consequence |
|---|---|
| Nonrotation | Rotation arrested before 90°; small bowel on right, colon on left; cecum near midline |
| Incomplete/mixed rotation | Arrest at ~180°; DJ junction stays right of midline; cecum in upper abdomen |
| Reverse rotation | Colon trapped posterior to SMA and duodenum |
In all variants, the mesenteric base remains narrow - instead of a broad diagonal fixation, both the DJ junction and ileocecal junction lie close together near the midline. This predisposes the entire midgut to twist around the SMA pedicle. Additionally, Ladd's bands - abnormal peritoneal attachments from the malpositioned cecum across the duodenum to the right posterior abdominal wall - cause extrinsic duodenal compression.
Associated anomalies arising from the same developmental window (weeks 4-12): omphalocele, gastroschisis, congenital diaphragmatic hernia, duodenal atresia, biliary atresia.
- The Developing Human: Clinically Oriented Embryology; Mulholland & Greenfield's Surgery, 7th Edition; Sabiston Textbook of Surgery, 21st Edition
Part 2: Clinical Presentation [3 marks]
Incidence: ~1 in 200 (all rotational anomalies); ~1 in 6000 with clinically symptomatic malrotation.
- 70% present in the first year of life, of which 70% in the first month
- Up to 1% present in adults
A. Midgut Volvulus (Surgical Emergency)
The narrow mesenteric pedicle allows the entire midgut to twist, obstructing the SMA and causing ischaemia:
Early:
- Bilious (green) vomiting - the cardinal sign; must be treated as an emergency until malrotation is excluded
- Colicky abdominal pain, feeding intolerance, irritability
- Guaiac-positive stool (early mucosal ischaemia)
- Relatively soft, non-distended abdomen early on
Late (bowel ischaemia/necrosis):
- Progressive abdominal distension
- Haematemesis, bloody stools (PR bleeding)
- Shock, hypotension
- Metabolic acidosis, coagulopathy
- Peritonitis, sepsis
- If untreated: transmural necrosis of the entire midgut supplied by the SMA
An acutely ill, lethargic/somnolent neonate with bilious emesis is an ominous presentation mandating immediate surgical evaluation.
B. Duodenal Obstruction by Ladd's Bands
- Bilious vomiting with gastric distension
- Less haemodynamically compromised than volvulus
- May present as partial or intermittent obstruction
C. Chronic / Intermittent Presentation
- Recurrent episodes of colicky abdominal pain ("recurrent abdominal pain")
- Intermittent vomiting, failure to thrive, malabsorption
- In adults: chronic abdominal pain, episodic obstruction (can mimic IBS or functional disorders for years)
D. Asymptomatic / Incidental
-
Discovered on contrast studies or CT performed for other indications
-
Estimated in ~1% of population
-
Current Surgical Therapy, 14th Edition; Mulholland & Greenfield's Surgery, 7th Edition
Part 3: Management [3 marks]
Initial Resuscitation
- IV access, fluid resuscitation, correction of electrolyte imbalances
- Nasogastric decompression
- In volvulus with shock: aggressive resuscitation must occur simultaneously with preparation for theatre - not sequentially
Investigations
- Plain AXR: Paucity of distal small bowel gas; gastric and proximal duodenal distension. A normal gas pattern NEVER excludes malrotation.
- Upper GI contrast series (UGI) - investigation of choice: Three features must be present to exclude malrotation:
- Duodenum crosses to the left of the midline (using spine as landmark)
- C-loop shape - 4th part of duodenum rises to level of pylorus
- Retroperitoneal course (confirmed on lateral view)
- Malrotation + volvulus shows corkscrew/coiled appearance in distal duodenum
- Ultrasound: Inverted SMA/SMV relationship (SMV to the left or anterior to SMA) suggests malrotation
- Contrast enema: Cecal malposition (in left abdomen or near midline)
If the infant is critically ill with bilious emesis, emergent laparotomy may be indicated without waiting for imaging.
Surgical Management - Ladd's Procedure
Approach: Emergency supraumbilical transverse laparotomy. Laparoscopic approach is feasible in stable elective cases.
Steps:
- Detorsion of volvulus - deliver the midgut out of the abdomen; rotate counterclockwise ("turning back the hands of time") - usually 180°-360° until fully unwound
- Assess bowel viability - frankly necrotic bowel is resected; borderline bowel can be reassessed after 15-20 minutes of warm packs ("second look" laparotomy at 24-48 hours for extensive ischaemia)
- Divide Ladd's bands - lyse peritoneal bands crossing from the cecum over the duodenum to the right posterior abdominal wall
- Straighten the duodenum - extended Kocher maneuver; divide all anterior, lateral, and posterior duodenal attachments
- Broaden the mesenteric base - divide peritoneal bands around the SMA pedicle widely to place the DJ junction and ileocecal valve far apart, preventing re-volvulus
- Final position - bowel placed in position of non-rotation: small bowel on the right, colon on the left
- Appendicectomy - incidental appendicectomy is performed as the appendix will be in an atypical position post-procedure (could cause diagnostic confusion in future appendicitis)
Special Situations
- Complete midgut infarction: Requires total enterectomy; carries very high mortality; survivors require permanent TPN or intestinal transplantation
- Asymptomatic incidental malrotation: Elective Ladd's procedure is generally recommended given the unpredictable and potentially catastrophic risk of volvulus at any age
- Adults with malrotation: Same principles apply; mortality from volvulus in adults may approach 3% even with treatment
Postoperative
-
Gradual reintroduction of feeds
-
Long-term monitoring for adhesive obstruction (rare)
-
Excellent outcomes when operated before bowel necrosis occurs; survival >90% in uncomplicated cases
-
Sabiston Textbook of Surgery, 21st Edition; Current Surgical Therapy, 14th Edition; Mulholland & Greenfield's Surgery, 7th Edition
Discuss the presentation, diagnosis and management of infantile hypertrophic pyloric stenosis. [2+3+5]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, mark-specific content. Composing the full structured answer:
Infantile Hypertrophic Pyloric Stenosis (IHPS)
Definition and Epidemiology
IHPS is a form of gastric outlet obstruction caused by progressive hypertrophy of the circular smooth muscle of the pyloric channel, causing narrowing and functional obstruction. It is the most common abdominal surgical condition in the first 6 months of life and the commonest cause of vomiting requiring surgery in infants.
- Incidence: ~1 in 300-500 live births (UK: 1:300; USA: 3 in 1000); varies by ethnicity - highest in white northern Europeans, lowest in Asians
- Sex: Males outnumber females 4:1 to 5:1; first-born males particularly affected
- Genetics: Autosomal dominant forms reported; 5 genetic loci identified including NOS1 (12q24), IHPS2/5 (chromosome 16); MBNL1 and NKX2-5 identified on GWAS
- Risk factors: Family history (maternal relatives carry higher risk), macrolide antibiotic exposure in early infancy (including via breast milk), Turner syndrome, trisomy 18, oesophageal atresia
Aetiology: The exact cause is unknown but proposed mechanisms include:
- Localised deficiency of nitric oxide synthase (NOS1) - an enzyme critical for smooth muscle relaxation
- Abnormal neuronal innervation - reduced neurofilaments, nerve terminals, synaptic vesicle protein
- Misplaced interstitial cells of Cajal (pacemaker cells) confined near submucosa rather than throughout pylorus
- Elevated EGF and heparin-binding EGF-like growth factor in smooth muscle cells
Part 1: Presentation [2 marks]
Age of Onset
Infants are typically asymptomatic at birth. Symptoms begin at 2-6 weeks of age (most commonly 3-4 weeks), as the muscular hypertrophy is an evolving postnatal process. This is why IHPS is not considered a true congenital defect.
Symptoms
- Non-bilious projectile vomiting - the hallmark symptom. Vomiting is so forceful it may exit through both mouth and nostrils; can project 1-2 metres. The obstruction is pre-pyloric (above the ampulla of Vater), hence vomiting is never bilious (green)
- Initially mild regurgitation, progressing in frequency and forcefulness daily - distinguishing it from gastro-oesophageal reflux (GOR), which waxes and wanes from birth
- Vomitus may be "coffee ground" coloured or contain small amounts of frank blood (from gastric mucosal irritation) but is never bile-stained
- Hunger after vomiting - infant remains hungry and demands re-feeding immediately after vomiting; this distinguishes it from infective/septic causes of vomiting (e.g. meningitis, UTI) where the infant is unwell and not hungry
- Over time: loss of interest in feeding, weight loss, failure to thrive
Signs
-
Visible gastric peristalsis - waves seen passing from left to right across the upper abdomen (left hypochondrium to right), best observed during a test feed
-
Palpable pyloric "olive" - a firm, smooth, ovoid mass ~2 cm long palpable in the right upper quadrant/epigastrium, best felt in a relaxed/feeding infant, or after the stomach has been emptied by NGT aspiration, or with the infant prone. Palpable in 70-90% of cases (though now less commonly found as infants are diagnosed earlier)
-
Dehydration - sunken fontanelle, dry mucous membranes, reduced skin turgor, reduced urine output
-
Wasting/cachexia - in late presentation
-
Jaundice - indirect hyperbilirubinaemia in ~2-5% (related to volume depletion and poor caloric intake)
-
Bailey & Love's Short Practice of Surgery, 28th Edition; Sleisenger & Fordtran's Gastrointestinal and Liver Disease
Part 2: Diagnosis [3 marks]
Metabolic/Biochemical Findings
Repeated vomiting of gastric acid (HCl) leads to characteristic metabolic derangements:
| Electrolyte / Acid-Base | Finding | Mechanism |
|---|---|---|
| Serum chloride | ↓ Hypochloraemia | Loss of Cl⁻ in HCl vomitus |
| Serum potassium | ↓ Hypokalaemia | Renal K⁺ loss in exchange for H⁺ retention; aldosterone-driven |
| Blood pH | ↑ Metabolic alkalosis | Loss of H⁺ ions in vomitus |
| Serum sodium | May be ↓ (hyponatraemia) | Dilutional; ADH response to volume depletion |
| Urine | Paradoxical aciduria | Despite systemic alkalosis, kidneys preferentially conserve Na⁺ by excreting H⁺ when K⁺ stores are depleted |
Classic biochemical picture: Hypochloraemic, hypokalaemic metabolic alkalosis with paradoxical aciduria.
Investigations
1. Test Feed (clinical diagnosis)
- Feed the undressed infant cradled in the mother's arm under good light
- Observe for visible left-to-right gastric peristaltic waves
- Palpate for the pyloric "olive" in the RUQ/epigastrium
- When the "olive" is palpated confidently, no imaging is required
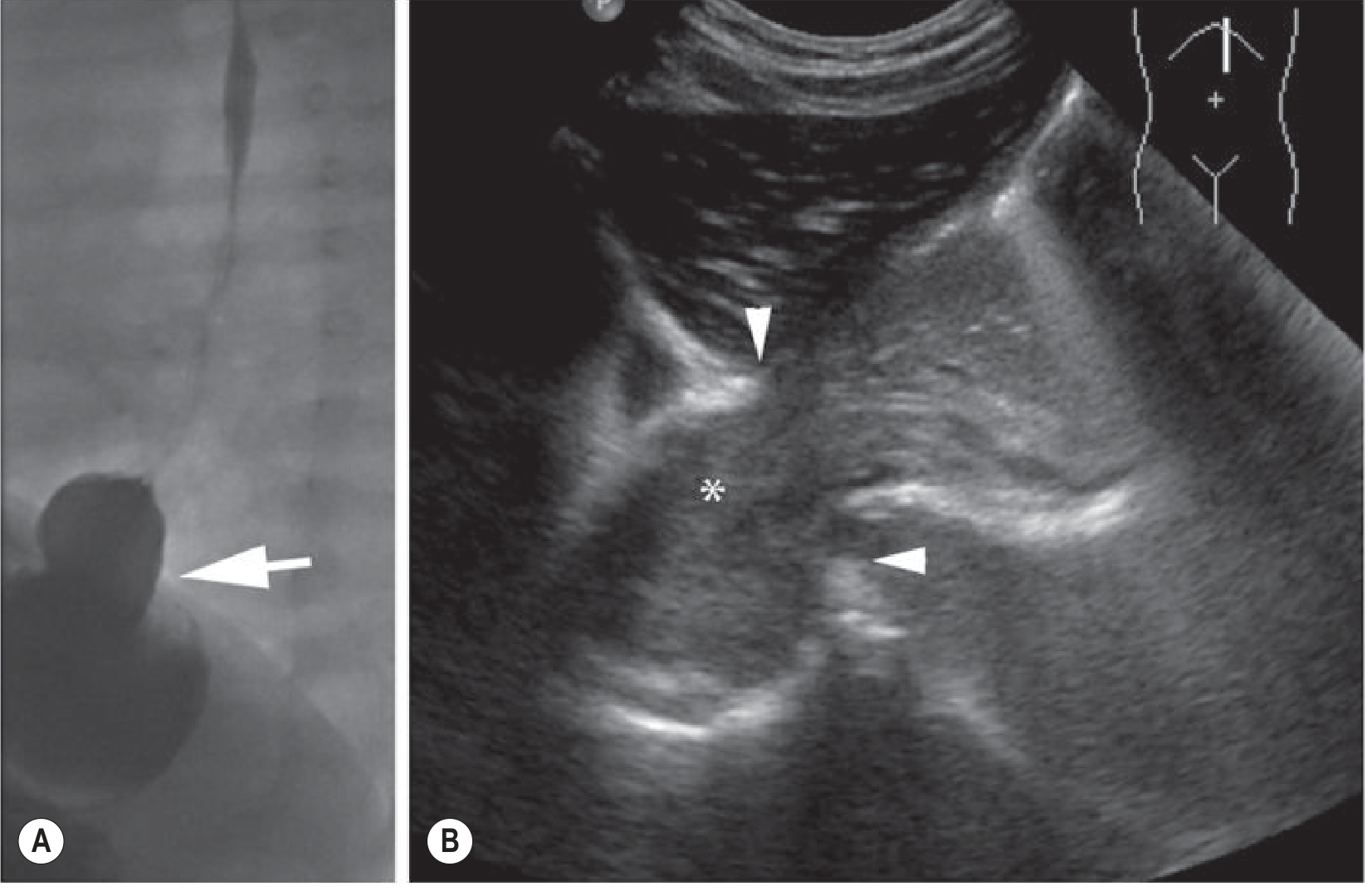
2. Abdominal Ultrasound - investigation of choice
- Has replaced barium studies; sensitivity up to 98%, specificity up to 100%
- Performed with a high-frequency linear transducer after emptying the stomach
Diagnostic USS criteria:
| Measurement | Normal | IHPS |
|---|---|---|
| Pyloric muscle wall thickness | <3 mm | ≥3-4 mm (most reliable) |
| Pyloric canal length | <15 mm | ≥17-20 mm |
| Pyloric diameter | <13 mm | ≥13-15 mm |
USS signs:
- "Donut/target sign" on transverse view - hypoechoic thickened muscle ring surrounding hyperechoic mucosa
- "Cervix sign" - hypertrophied pylorus resembles the uterine cervix on longitudinal view
- "Shoulder sign" - hypertrophic muscle bulges into the gastric antrum
- "Nipple sign" - redundant hyperechoic mucosa protrudes into the stomach
- Exaggerated, non-propulsive peristaltic waves seen in real time
3. Plain AXR
- Distended stomach ("single bubble" appearance)
- Paucity of gas beyond the stomach
4. Barium/Contrast Upper GI Series (now rarely needed; used when USS equivocal or GOR is also in differential)
-
"String sign" - elongated, narrow pyloric canal
-
"Double channel/rail track sign" - two parallel streaks of contrast in compressed canal
-
"Shoulder/beak sign" - indentation of the antrum by the hypertrophied pyloric muscle
-
"Mushroom/umbrella sign" - bulging of pyloric mass into gastric antrum
-
Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Grainger & Allison's Diagnostic Radiology
Part 3: Management [5 marks]
IHPS is NOT a surgical emergency. It is a medical emergency first - the electrolyte and fluid deficit must be corrected before any anaesthetic or surgery, as severe hypochloraemic alkalosis can precipitate life-threatening anaesthetic complications (apnoea, laryngospasm).
Step 1 - Resuscitation and Correction of Metabolic Derangement
- Stop oral feeds immediately
- Nasogastric tube (8-10 Fr) insertion - decompress and empty the stomach
- IV fluid resuscitation:
- 0.9% normal saline with 0.15% KCl in 5% dextrose at 6-7.5 mL/kg/h
- This provides maintenance fluids and corrects the chloride and potassium deficit simultaneously
- As the chloride deficit is replaced, the kidneys correct the alkalosis and urine becomes alkaline
- Monitoring: Serial U&E/electrolytes until normalised; urine output >1 mL/kg/h
- Correction typically takes 24-48 hours
- Surgery should NOT proceed until: Cl⁻ >95 mmol/L, K⁺ >3.0 mmol/L, pH <7.45, bicarb <30 mmol/L
Step 2 - Ramstedt's Pyloromyotomy (Definitive Treatment)
Approach:
- Laparoscopic pyloromyotomy - now the preferred approach in most centres (3 ports: umbilical camera, two 3mm working ports); equivalent outcomes, better cosmesis, faster recovery
- Open pyloromyotomy - via supraumbilical curved incision or right upper quadrant transverse (Ramstedt's) incision; remains the approach when laparoscopy is not available or feasible
Technique (Ramstedt, 1912):
- Deliver the pyloric "tumour" into the wound
- Make a longitudinal serosal incision along the avascular plane of the anterior pylorus, from the gastric antrum proximally to the duodenal fornix distally
- Split the hypertrophied circular muscle fibres with a pyloric spreader (Ramstedt's dilator), leaving the underlying submucosa and mucosa intact and bulging
- The incision must extend onto the stomach (gastric side) - a short incision stopping at the pyloric-gastric junction causes early recurrence
- The duodenal end requires care - the muscle fibres here are thinner and mucosal perforation is most likely at the duodenal fornix
- Test for mucosal integrity: Air or saline injected via NGT confirms no perforation (bubbles or bile leak)
- If perforation occurs intraoperatively: close with absorbable suture, rotate the myotomy 90° and repeat
Result: The divided muscle springs apart, the submucosal bulge indicates success - the pyloric channel opens, and the obstruction is relieved.
Step 3 - Postoperative Care
- Continue IV fluids until feeds are re-established
- Oral feeding commenced within 24 hours postoperatively - gradual reintroduction of feeds (small volumes initially, progressing to full feeds)
- Early postoperative vomiting is common and expected (due to oedema at the myotomy site and pre-existing GOR); it usually resolves within 24-48 hours
- Persistent vomiting beyond 5-7 days: consider incomplete myotomy or co-existing GOR (more likely than incomplete myotomy)
Complications
| Complication | Details |
|---|---|
| Mucosal perforation | Most common intraoperative complication (~1-3%), especially at duodenal end |
| Incomplete myotomy | Persistent vomiting; may need re-operation |
| Wound infection | More common in open approach |
| Recurrence | Rare; usually due to inadequate gastric extension of myotomy |
| GOR | Common postoperatively, usually self-limiting |
Outcomes
-
Excellent - mortality essentially nil in well-resourced settings when metabolic correction is completed before surgery
-
Full recovery expected; pyloric muscle eventually returns to normal calibre over months
-
No long-term sequelae
-
Bailey & Love's Short Practice of Surgery, 28th Edition; Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Grainger & Allison's Diagnostic Radiology
Vitellointestinal duct and abnormalities associated with it
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive content from embryology and surgery textbooks. Composing the full answer:
Vitello-intestinal Duct (VID) and Its Abnormalities
Embryology and Normal Fate
The vitello-intestinal duct (also called the omphalomesenteric duct or vitelline duct) is a normal embryological structure that connects the primitive midgut to the yolk sac (extra-embryonic) during early fetal development.
Timeline:
- At week 5, the following structures pass through the umbilical ring: the connecting stalk (with allantois and umbilical vessels), the yolk stalk (vitelline duct) with its vessels, and intestinal loops during physiological umbilical herniation
- The midgut loop herniates into the proximal umbilical cord at week 5-6 and remains there until week 10, with the VID at the apex communicating with the yolk sac
- As the midgut returns to the abdominal cavity by week 10-12, the VID and yolk sac normally obliterate completely
- By the end of the third month, only the umbilical vessels surrounded by Wharton's jelly remain in the cord
When the VID fails to obliterate completely, various remnants and anomalies result, depending on which segment persists and the degree of obliteration.
- Langman's Medical Embryology; The Developing Human
Spectrum of VID Remnant Abnormalities
There are five main types of abnormalities depending on which part of the duct persists:
1. Meckel's Diverticulum (Most Common)
The most common VID remnant (~67% of all omphalomesenteric duct remnants) and the most common congenital anomaly of the GI tract.
Pathology:
- The ileal (bowel) end of the VID persists as a blind-ending outpouching
- A true diverticulum - contains all three layers of the bowel wall (mucosa, muscularis propria, serosa)
- Arises from the antimesenteric border of the ileum

The Rule of 2s:
| Feature | Value |
|---|---|
| Prevalence | 2% of population |
| Distance from ileocaecal valve | 2 feet (60 cm) |
| Length | 2 inches (5 cm) |
| Male:Female ratio | 2:1 |
| Symptomatic in | ~2% of cases |
| Most symptomatic by age | 2 years |
| Ectopic tissue types | 2 (gastric or pancreatic) |
Ectopic mucosa: Present in ~50% of diverticula:
- Gastric mucosa - 80-85% of ectopic tissue (secretes acid)
- Pancreatic, duodenal, biliary, or colonic tissue - less common
Clinical Complications:
| Complication | Features |
|---|---|
| Painless rectal bleeding (most common) | Ectopic gastric mucosa secretes acid → peptic ulceration at gastric-ileal mucosal junction; blood usually maroon-coloured or melaena; commonest in children |
| Intestinal obstruction | Either by: (a) intussusception with the diverticulum as the lead point, or (b) volvulus around a persistent fibrous cord remnant of VID between diverticulum and umbilicus |
| Meckel's diverticulitis | Acute inflammation mimicking appendicitis; perforation in ~1/3 of cases may resemble perforated duodenal ulcer |
| Chronic ulceration | Periumbilical pain (midgut origin); can cause chronic blood loss |
| Littre's hernia | Meckel's diverticulum in an inguinal or femoral hernia sac |
| Intestinal obstruction (band) | Fibrous cord between diverticulum apex and umbilicus causes direct obstruction or volvulus |
Diagnosis:
- Tc-99m (Technetium) pertechnetate scan ("Meckel's scan") - investigation of choice for bleeding; detects ectopic gastric mucosa; sensitivity ~85% in children
- CT scan: blind-ending tubular structure from antimesenteric border of terminal ileum
- CT enterography: improved detection
- Plain X-ray, barium studies, USS: rarely diagnostic
Management:
- Symptomatic Meckel's: Always requires surgical excision
- Surgical approach: Diverticulectomy with transverse closure of the defect, or segmental ileal resection with end-to-end anastomosis (preferred if base is wide, indurated, or if ectopic tissue extends to base); can use linear stapler-cutter
- A broad-based diverticulum should not be amputated and invaginated (risk of stricture and leaving ectopic tissue behind)
- Incidental Meckel's in adults: Generally left alone if wide-mouthed and not thickened; prophylactic resection considered in children, or in adults with palpable ectopic tissue, mesodiverticular band, prior bleeding/diverticulitis
- Laparoscopic approach feasible
2. Umbilical Fistula (Patent Vitello-intestinal Duct / Entero-umbilical Fistula)
The entire duct remains patent throughout its length, creating a direct communication between the ileal lumen and the umbilicus.
- Presentation: Discharge of faecal/intestinal contents from the umbilicus in the neonatal period; the ileum may even prolapse through the umbilicus onto the anterior abdominal wall
- Rare but most serious VID remnant
- Management: Surgical excision and closure of the fistula
3. Umbilical Sinus (Umbilical End Patent)
Only the umbilical (outer) end of the duct remains patent, opening at the umbilicus as a blind-ended sinus.
- Presentation: Chronic mucoid or serous discharge from the umbilicus; may become recurrently infected
- Differentiated from urachal sinus (which also opens at umbilicus but is connected to bladder)
- Management: Surgical excision of the sinus tract
4. Vitello-intestinal Cyst (Enteric Cyst / Enterogenous Cyst)
Both the ileal and umbilical ends obliterate but the middle segment persists as a cystic remnant within the abdominal cavity, connected to the ileum and umbilicus by fibrous cords.
- Presentation: May be asymptomatic (incidental); can cause intestinal obstruction by external compression or volvulus around the cyst; may become infected
- Management: Surgical excision
5. Fibrous Cord (Obliterated VID / Mesodiverticular Band)
The duct is fully obliterated but persists as a solid fibrous band running from the antimesenteric border of the ileum to the umbilicus, with no patent lumen.
- Presentation: The cord acts as a fulcrum around which bowel loops can twist → small bowel volvulus and strangulation; can also cause direct obstruction
- Has been described causing volvulus even in neonatal period
- Management: Division of the fibrous band at laparotomy/laparoscopy; resection of any non-viable bowel
Summary Table
| Abnormality | Portion of VID That Persists | Presentation |
|---|---|---|
| Meckel's diverticulum | Ileal end | Bleeding, obstruction, diverticulitis |
| Umbilical (entero-umbilical) fistula | Entire duct patent | Faecal discharge from umbilicus |
| Umbilical sinus | Umbilical end | Mucopurulent umbilical discharge |
| Vitello-intestinal cyst | Middle segment | Abdominal cyst ± obstruction |
| Fibrous cord | Entire duct obliterated but fibrous | Volvulus, intestinal obstruction |
Diagnostic Investigations (Summary)
| Investigation | Use |
|---|---|
| Tc-99m pertechnetate scan | Bleeding Meckel's (ectopic gastric mucosa) |
| CT abdomen / CT enterography | Obstruction, diverticulitis, incidental finding |
| Ultrasound | Cyst, umbilical sinus |
| Laparoscopy | Diagnostic and therapeutic |
| Sinogram/fistulogram | Umbilical sinus/fistula delineation |
- Bailey & Love's Short Practice of Surgery, 28th Edition; Robbins, Cotran & Kumar Pathologic Basis of Disease; Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Current Surgical Therapy, 14th Edition; Langman's Medical Embryology
a) Clinical features and management of Hirschsprung’s disease.
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I have comprehensive content. Here is the complete structured answer:
Hirschsprung's Disease (Congenital Aganglionic Megacolon)
Definition and Pathogenesis
Hirschsprung's disease (HD) is a neurocristopathy characterised by the congenital absence of ganglion cells in the myenteric (Auerbach's) and submucosal (Meissner's) plexuses of the distal colon and rectum, caused by failure of caudal migration of neural crest-derived neuroblasts during weeks 5-12 of gestation.
Because ganglion cells are responsible for coordinated peristalsis and relaxation, the aganglionic segment is:
- Tonically contracted (functionally obstructed, narrow, normal external calibre)
- Unable to relax the internal anal sphincter
The proximal, normally innervated bowel dilates progressively - hence the term megacolon.
Genetics: Mutations in the RET proto-oncogene (chromosome 10) are identified in familial cases; associated with MEN 2A and 2B.
Incidence: 1 in 5000 live births; M:F = 4:1
Extent of aganglionosis:
| Segment | Proportion |
|---|---|
| Rectosigmoid (short-segment) | ~75-80% of cases |
| Sigmoid to splenic flexure | ~17% |
| Total colonic aganglionosis (TCA) | ~8% (may involve distal ileum) |
| Total intestinal Hirschsprung disease | Very rare |
| Ultra-short segment (internal sphincter only) | Rare |
Associations: Down syndrome (trisomy 21) in 3-10% of patients; anorectal atresias, cleft palate, polydactyly, cardiac septal defects, MEN 2A/2B.
Clinical Features
A. Neonatal Presentation (>90% of cases)
The classic triad:
- Failure to pass meconium within 24-48 hours of birth - the most important early sign; normal neonates pass meconium within 24 hours
- Abdominal distension - progressive, generalised
- Bilious vomiting - secondary to the functional distal obstruction
Additional features:
- Tight, empty rectum on digital rectal examination (DRE) - finger meets resistance ("the aganglionic segment grips the finger")
- Explosive passage of meconium or gas on rectal examination (dramatic decompression) - characteristic and temporarily relieves symptoms
- Symptoms recur without definitive treatment
- Regular enemas provide temporary relief
B. Later/Delayed Presentation (in older children and adults)
When the diagnosis is missed in infancy (more likely with short-segment disease or ultra-short segment):
- Chronic constipation from birth - often lifelong history, intractable to conservative management
- Abdominal distension - persistent, progressive
- Failure to thrive, malnutrition, poor growth
- Ribbon-like, narrow stools (reflecting narrow aganglionic channel)
- In adults: massive megacolon visible on imaging
- Children with longer-segment disease and TCA can paradoxically have milder initial symptoms, causing diagnostic delay
C. Hirschsprung Enterocolitis (Most Serious Complication)
Occurs in 18-50% of patients, in both pre- and postoperative periods. It is the leading cause of death in Hirschsprung disease.
- Bacterial overgrowth in the obstructed, stagnant bowel → mucosal breakdown → bacterial translocation
- Presentation: Explosive, foul-smelling watery or bloody diarrhoea, fever, abdominal distension, lethargy
- Can rapidly progress to: haemorrhagic colitis, peritonitis, septicaemia, shock, death
- Higher frequency in: long-segment disease, diagnosis delayed beyond first week of life
Emergency management of enterocolitis: Rectal washouts (decompression), IV antibiotics, fluid resuscitation; may require urgent colostomy.
- Sabiston Textbook of Surgery, 21st Edition; Grainger & Allison's Diagnostic Radiology
Diagnosis
1. Plain Abdominal Radiograph
- Dilated loops of bowel consistent with low bowel obstruction
- Absence of gas in the rectum
- Massive megacolon in delayed presentations
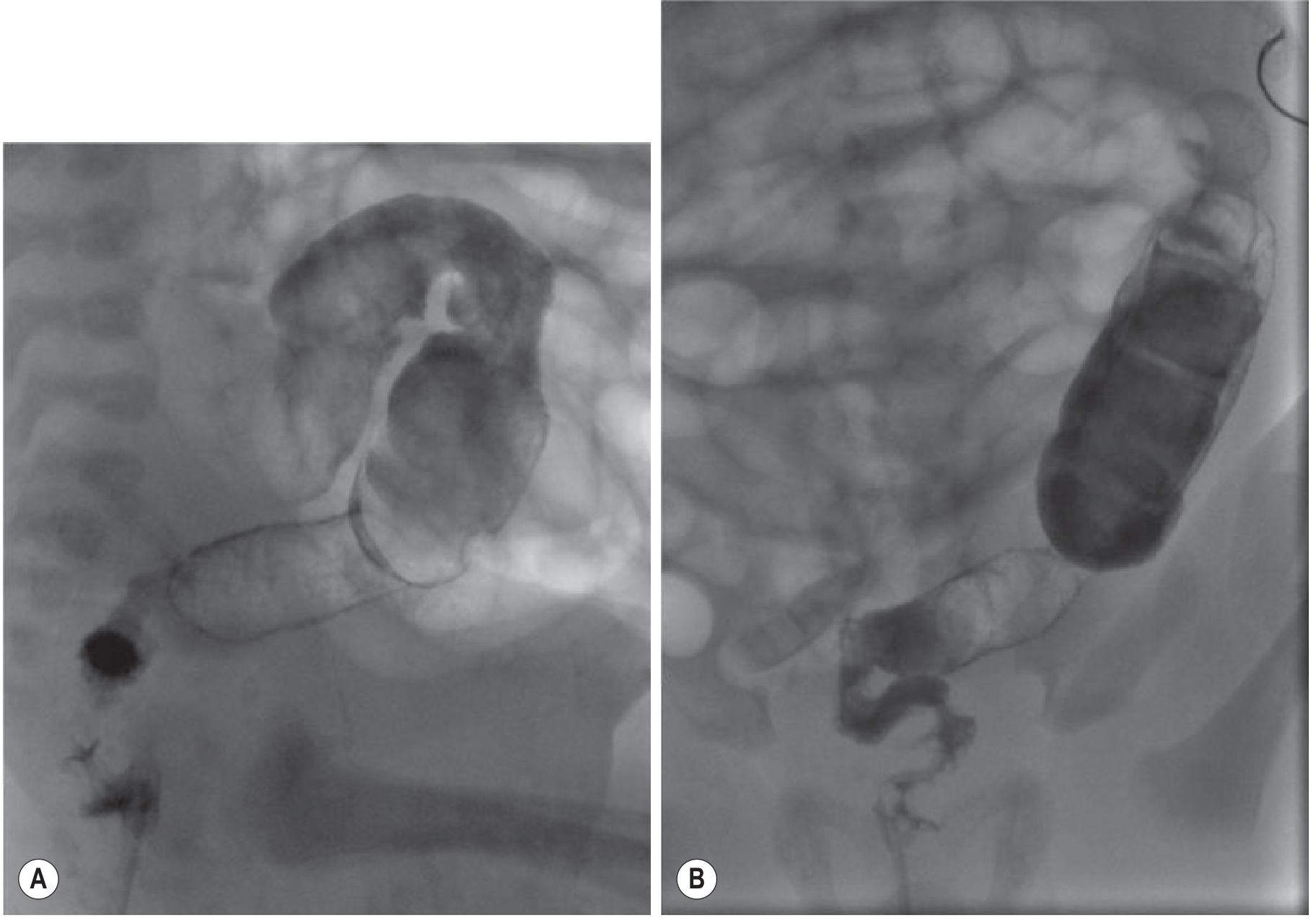
2. Contrast Enema - Investigation of Choice in Newborns
Technique: No bowel preparation; at least 48 hours since last enema/rectal examination; catheter tip placed just inside rectum with balloon uninflated (inflated balloon can obscure the transition zone or perforate the stiff aganglionic bowel).
Findings:
- Narrow aganglionic rectum with abrupt transition to dilated proximal ganglionated bowel (cone-shaped transition zone)
- Reversed rectosigmoid ratio - normally the rectum should be wider than the sigmoid; in HD this ratio is inverted
- Irregular contractions in the aganglionic segment
- Failure to evacuate contrast at 24 hours strongly suggests HD
- Sensitivity ~70%, specificity ~83%; negative predictive value 98% in infants >1 month
In TCA, the contrast enema may appear normal (colonic shortening and loss of normal flexure contours are subtle signs).
Contraindication: Enterocolitis with severe colitis - contrast enema is contraindicated.
3. Anorectal Manometry
- In toddlers and older children
- Failure of the internal anal sphincter to relax after rectal balloon distension (absent rectoanal inhibitory reflex - RAIR) is diagnostic
- Sensitivity ~75-90%
4. Rectal Biopsy - Gold Standard
The definitive diagnostic investigation. Absent ganglion cells + hypertrophied acetylcholinesterase-positive nerve fibres confirm the diagnosis.
Types:
| Type | Indication | Technique |
|---|---|---|
| Suction rectal biopsy | Neonates and infants; bedside | Suction device removes mucosa/submucosa; minimum 2 specimens ≥1 cm apart; taken at least 5 mm-1 cm above the dentate line |
| Full-thickness biopsy | Older children; under GA | Required as thicker rectal wall not amenable to suction technique |
Histological criteria:
- Absent ganglion cells in submucosal and myenteric plexuses
- Hypertrophied nerve trunks (acetylcholinesterase-positive)
- Calretinin immunostaining - an adjunct marker (absent staining in aganglionic segment); now standard
Management
Step 1 - Initial Stabilisation
- Rectal washouts/irrigations - daily with warm normal saline via soft red rubber catheter; decompresses the bowel and prevents enterocolitis
- IV fluid resuscitation and correction of electrolytes
- Nutritional support
- Levelling colostomy - required when:
- Rectal irrigations are ineffective or not feasible
- Family circumstances prevent proper irrigation
- Long-segment or TCA
- Enterocolitis with deterioration
- Colostomy is fashioned at the most distal level of ganglionated bowel (confirmed by intraoperative frozen section biopsies)
Step 2 - Definitive Surgery: Pull-Through Procedure
The principle: resect the aganglionic segment and pull the normal ganglionated bowel through to the anus, anastomosing it close to the dentate line.
Intraoperative frozen section biopsies confirm ganglionated (normal) bowel at the level of pull-through before anastomosis.
Three main techniques are used; functional results are similar when performed by experienced surgeons:
a) Swenson Pull-Through (1949 - the original procedure)
- Full-thickness dissection of the rectum from the surrounding sphincter mechanism
- Dissection from the abdomen extended distally, or starting 5-10 mm proximal to the dentate line extending proximally
- Resection of all aganglionic bowel; coloanal anastomosis performed
- Can be done open, laparoscopic-assisted, or entirely transanal
b) Soave Endorectal Pull-Through (most commonly used)
- Endorectal mucosal dissection within the aganglionic rectum via transanal approach, starting 5 mm proximal to the dentate line
- Leaves the muscular cuff of aganglionic rectum in situ; dissection plane converted to full thickness at the level of the intraabdominal rectum
- Normal ganglionated colon pulled through the muscular cuff after posterior myotomy of the cuff
- Coloanal anastomosis performed at the dentate line
- Can be performed entirely transanally (without abdominal incision) or with laparoscopic assistance
c) Duhamel Retrorectal Pull-Through
- Anterior wall of the aganglionic rectal cuff is left in place
- Normal ganglionated colon is pulled posterior to the cuff (through the retrorectal space)
- Aganglionic cuff anastomosed to the pulled-through ganglionated colon in a side-to-side fashion, creating a common reservoir (neorectum)
- The posterior ganglionated segment drives normal emptying
One-stage vs. Multi-stage:
- One-stage pull-through with rectal irrigations - now the standard for most patients
- Two/three-stage approach (levelling colostomy → pull-through → stoma closure) - reserved for enterocolitis, severely ill neonates, long-segment disease, TCA
Postoperative Care and Complications
| Complication | Details |
|---|---|
| Constipation | Most common long-term problem; managed with stool softeners and laxatives |
| Soiling/incontinence | Frequent initially, often improves with age |
| Postoperative enterocolitis | Occurs in 18-50%; requires rectal decompression and antibiotics |
| Anastomotic stricture/leak/fistula | Requires investigation and surgical revision |
| Residual/recurrent aganglionosis | Residual aganglionic bowel left at anastomosis; confirmed by rebiopsy |
| Permanent colostomy | Eventually required in ~10% |
Long-term follow-up is mandatory. If persistent symptoms occur, histological re-evaluation should confirm normal ganglionated bowel at the anastomosis and exclude transition zone pull-through.
- Sabiston Textbook of Surgery, 21st Edition; Grainger & Allison's Diagnostic Radiology; Schwartz's Principles of Surgery, 11th Edition
This is a shared conversation. Sign in to Orris to start your own chat.