Dengue psm
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the key information needed for a comprehensive PSM-oriented dengue answer. Let me compile the complete response:
Dengue - Preventive & Social Medicine (PSM)
Source: Park's Textbook of Preventive and Social Medicine
The Dengue Syndrome
Dengue virus infection can manifest in four ways, as shown in the classification diagram:
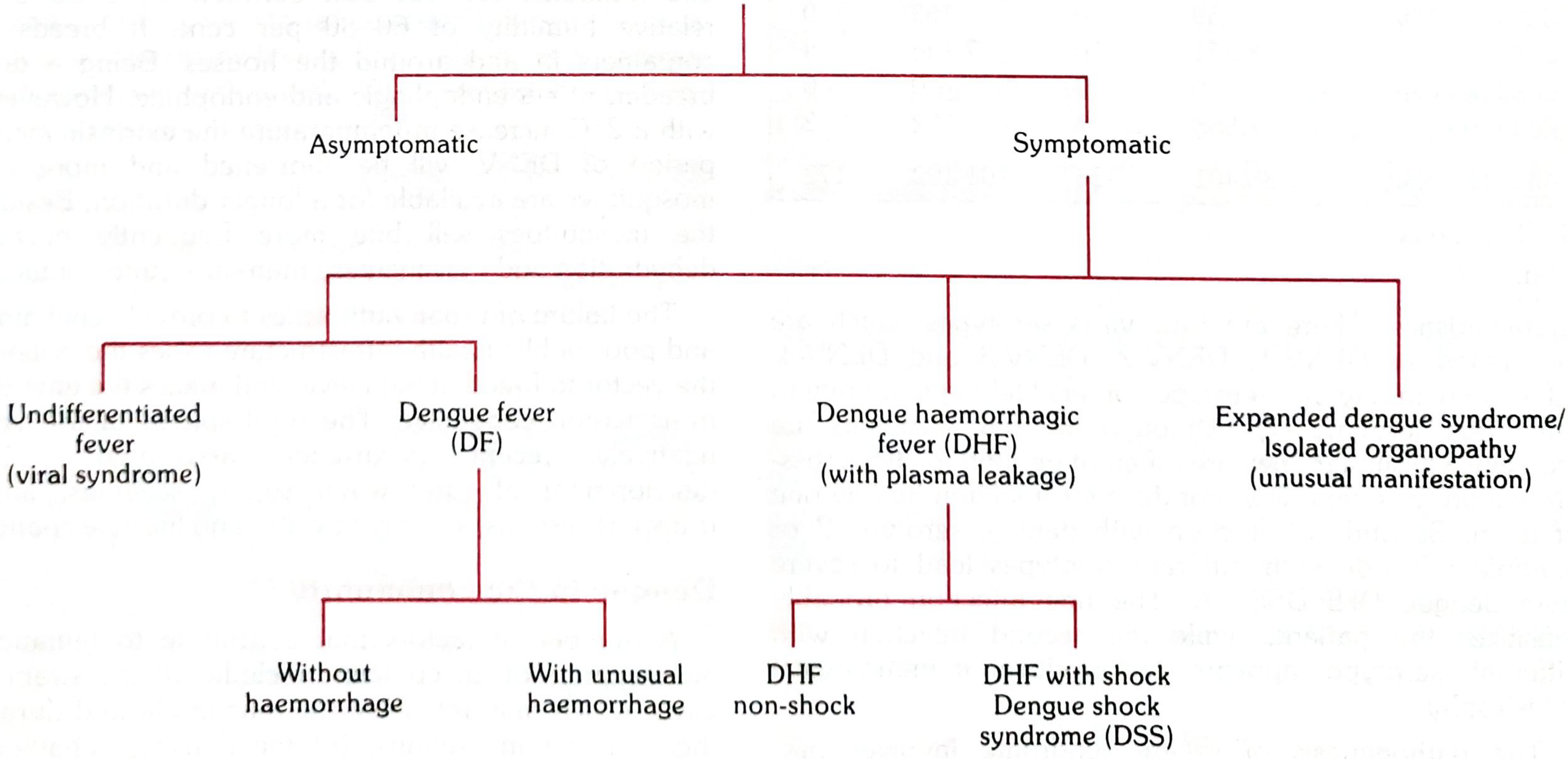
- Asymptomatic (silent infection)
- Undifferentiated fever (viral syndrome)
- Classical Dengue Fever (DF) - with or without unusual haemorrhage
- Dengue Haemorrhagic Fever (DHF) - with plasma leakage; subdivides into DHF non-shock and DHF with shock (Dengue Shock Syndrome - DSS)
- Expanded dengue syndrome / Isolated organopathy (unusual manifestations)
DF/DHF follows an "iceberg/pyramid" phenomenon - most cases at the base are asymptomatic, with DF, DHF, and DSS forming progressively narrower tiers above.
Problem Statement / Global Burden
- ~3.9 billion people in 128 countries are at risk of dengue infection
- 390 million infections per year; 96 million manifest clinically
- Reported cases rose from <0.5 million (2010) to 4.2 million (2019)
- ~500,000 DHF hospitalizations per year worldwide; ~90% are children <5 years
- CFR: ~2.5% during epidemics
- Attack rate during outbreaks in non-immune populations: 40-50%, can reach 80-90%
- Regions most affected: South-East Asia and Western Pacific
India
- Endemic in 35 states/UTs
- ~157,996 cases with 253 deaths in 2019; CFR 0.1%
- Seasonal pattern: cases peak after monsoon; southern states and Gujarat have perennial transmission
- All four serotypes isolated; DENV-1 and DENV-2 are currently widespread
- SEAR countries classified into 3 categories:
- Category A (India, Indonesia, Thailand, Myanmar, etc.) - Major public health problem, hyperendemic with all 4 serotypes
- Category B (Bhutan, Nepal) - Endemicity uncertain, first outbreaks 2004
- Category C (DPR Korea) - No evidence of endemicity
Epidemiological Determinants
A. Agent Factors
| Feature | Detail |
|---|---|
| Causative agent | Dengue virus - Flavivirus (RNA virus) |
| Serotypes | 4 serotypes: DENV-1, 2, 3, 4 |
| Cross-immunity | Homologous (same serotype) - lifelong; Heterologous (different serotype) - partial, transient |
| Pathogenesis of DHF | Secondary infection with a different serotype triggers "antibody-dependent enhancement" - leads to plasma leakage |
B. Host Factors
- Age: In hyperendemic areas, DHF primarily affects children; in primary epidemic areas, all age groups affected
- Immunity: No cross-protection between serotypes; secondary infection increases risk of DHF/DSS (only 2-4% develop severe disease in sequential infections)
- Severity: Depends on serotype sequence of secondary infection; DENV-2 secondary infections associated with greater severity
C. Vector Factors
| Feature | Aedes aegypti | Aedes albopictus |
|---|---|---|
| Primary/secondary vector | Primary | Secondary |
| Biting habit | Day-biting (peak activity: 2 hrs after sunrise, late afternoon) | Day-biting |
| Habitat | Domestic/peridomestic | Peridomestic/semi-wild |
| Behaviour | Endophagic, endophilic | Less endophilic |
| Breeding sites | Man-made containers (stored water, flower pots, tyres, coolers) | Natural + artificial containers |
| Extrinsic incubation period | 8-10 days at 30°C | - |
D. Environmental Factors
- Temperature: Optimum 16-30°C; humidity 60-80%
- Aedes population fluctuates with rainfall and water storage
- Even a 2°C rise in temperature shortens the extrinsic incubation period and increases biting frequency
- Rapid urbanization, poor water management, and deficient sanitation amplify transmission
Clinical Features
1. Classical Dengue Fever
- Incubation period: 3-14 days (commonly 4-7 days)
- Sudden onset high fever (39-40°C)
- Severe headache, retro-orbital pain (pain on eye movement and pressure), photophobia
- Myalgia and arthralgia ("break-bone fever")
- Biphasic fever curve - remission for a few hours to 2 days
- Rash in 80% cases - appears during remission or 2nd febrile phase
- Early: diffuse flushing/mottling on face, neck, chest
- Later: maculopapular or scarlatiniform rash on chest/trunk (3rd-4th day), may spread to extremities; may itch and be followed by desquamation
- Fever lasts ~5 days (rarely >7 days); full recovery usual; CFR exceedingly low
2. Dengue Haemorrhagic Fever (DHF) - Three Phases
Phase 1 - Febrile Phase:
- Abrupt onset high fever, facial flushing, headache
- Anorexia, vomiting, epigastric discomfort, right costal tenderness
- Maculopapular (rubelliform) rash less common than in DF
- Positive Tourniquet Test (Rumple-Leede test)
Phase 2 - Critical Phase (day 3-7):
- Fever defervescence
- Plasma leakage - leads to pleural effusion, ascites
- Platelet count drops sharply (≤100,000/mm³)
- Haematocrit rises ≥20% (haemoconcentration) - hallmark of plasma leakage
- Risk of shock if plasma leakage is severe
Phase 3 - Recovery Phase:
- Plasma reabsorption
- Risk of fluid overload (pulmonary oedema) if IV fluids given excessively
DHF Grading (WHO)
| Grade | Features |
|---|---|
| I | Fever + constitutional symptoms + positive tourniquet test |
| II | Grade I + spontaneous bleeding (skin, mucosa, or GI) |
| III | Circulatory failure - rapid/weak pulse, narrowing pulse pressure (≤20 mmHg), hypotension, cold/clammy skin, restlessness |
| IV | Profound shock - undetectable pulse and BP (DSS) |
Diagnostic Criteria (WHO)
Classical Dengue Fever (Probable Case)
Acute febrile illness (2-7 days) with two or more of:
- Headache
- Retro-orbital pain
- Myalgia/arthralgia
- Rash
- Haemorrhagic manifestation
- Low WBC
- Confirmed by serology/virus isolation
DHF Criteria (All 4 must be present):
- Acute fever of 2-7 days
- Haemorrhagic manifestations (positive tourniquet test, petechiae/ecchymoses, or bleeding from mucosa/GI/injection sites)
- Platelet count ≤ 100,000/mm³
- Evidence of plasma leakage: rising haematocrit ≥20%, pleural effusion, ascites, or hypoproteinaemia
Dengue Shock Syndrome (DSS)
DHF criteria + signs of shock:
- Tachycardia, cool extremities, delayed capillary refill, weak pulse, lethargy/restlessness
- Pulse pressure ≤ 20 mmHg (e.g., 100/80 mmHg)
- Hypotension: systolic <80 mmHg (age <5 yrs) or 80-90 mmHg (older children/adults)
Confirmed Case
Probable case + any one of:
- Virus isolation from serum, CSF, or autopsy sample
- Fourfold or greater rise in IgG (by HI test) or rise in IgM
- Detection of virus/antigen by immunohistochemistry, immunofluorescence, or ELISA
- Detection of viral genome by RT-PCR
Laboratory Diagnosis
| Test | Best Window | Details |
|---|---|---|
| Virus isolation | Days 1-6 of illness | Serum, plasma, buffy coat, autopsy tissue (liver, spleen, lymph nodes) or mosquitoes |
| RT-PCR | Days 1-6 (acute phase) | Detects viral RNA; serotype identification possible |
| NS1 Antigen ELISA | Day 1 onwards | Early diagnosis - detects from Day 1 of infection |
| IgM ELISA (MAC-ELISA) | After day 5 | IgM rises from day 3-5, peaks at 2 weeks, lasts 2-3 months |
| IgG (HI test) | Fourfold rise in paired sera | Primary infection: IgM > IgG; Secondary infection: IgG rises earlier and higher than IgM |
| Haemagglutination inhibition (HI) | Paired sera | Reference serological test |
- IgM ELISA detects cases after Day 5 of infection
- NS1 ELISA kits can detect cases from Day 1
Treatment
Dengue Fever (DF)
- Supportive: adequate rest, fluids, paracetamol for fever
- Avoid aspirin/NSAIDs (risk of bleeding/Reye's syndrome)
- Oral rehydration if tolerating orally
DHF (Grades I & II) - Volume Replacement Algorithm
- Oral fluids first
- If not tolerated: IV crystalloids (Normal Saline, Ringer Lactate)
- Monitor haematocrit every 3-4 hours
- If Hct continues to rise: switch to colloids (Dextran 40/haemaccel)
- If Hct falls and patient improving: reduce IV fluids
DSS (DHF Grades III & IV)
- Immediate IV fluid resuscitation - crystalloid or colloid
- If Hct rising: colloid (Dextran 40/polygeline) at 10-20 ml/kg/hour
- If Hct declining: internal bleeding suspected → fresh whole blood 10 ml/kg/hour
- Oxygen to all patients in shock
- Monitor ABCS: Acidosis, Bleeding, Calcium (Na⁺, K⁺), Sugar
Indications for Red Cell Transfusion
- Overt blood loss ≥10% total blood volume
- Refractory shock despite fluids + declining haematocrit/Hb
- Replacement: 10 ml/kg at a time + coagulogram
- If fluid overload: give packed cells
Prevention and Control
1. Vector Control (Primary Strategy)
Source Reduction (most effective):
- Eliminate mosquito breeding places
- Weekly Dry Day - empty/scrub/clean all water containers weekly
- Proper covering of stored water
- Filling/sealing permanent water bodies
- Manage roof tops, porticos, sunshades
Chemical Control:
- Larviciding: Temephos (Abate) - for stored water
- Adult mosquito control: Malathion fogging/spraying (outbreak measure)
- Pyrethroid-based insecticides for indoor residual spraying
Biological Control:
- Larvivorous fish (Gambusia, Poecilia) in ornamental tanks, ponds
- Bacillus thuringiensis israelensis (Bti) - biological larvicide
Personal Protection:
- Full-sleeved clothing
- Mosquito repellents (creams, liquids, coils, mats)
- Bed nets (especially for sleeping infants/children during daytime)
- Screens on windows and doors
2. Vaccine - CYD-TDV (Dengvaxia - Sanofi Pasteur)
- World's first licensed dengue vaccine (licensed in Mexico, December 2015)
- Live attenuated tetravalent (all 4 serotypes) - chimeric yellow fever-dengue vaccine
- Schedule: 3 doses × 0.5 ml; 6-month intervals
- Route: Subcutaneous
- Age indication: 9-45 years (or 9-60 years depending on license) in endemic areas
- Contraindicated in:
- Severe allergic reaction to components
- Congenital/acquired immune deficiency
- Symptomatic HIV or asymptomatic HIV with immune impairment
- Pregnant/breastfeeding women
- Note: lower age limit is 9 years (safety concern in children aged 2-5 years in Phase 3 trials)
- Storage: 2-8°C; shelf life 36 months; discard reconstituted vaccine within 6 hours
3. Other Measures
- Isolation of patient under bed nets during first few days of illness (prevents further mosquito bites and transmission)
- Health education on Do's and Don'ts
- Sentinel surveillance hospitals (521 identified by GOI) with lab support
- 14 Apex Referral Laboratories for advanced diagnosis
- IgM capture ELISA kits supplied free by National Institute of Virology, Pune
WHO Global Strategy for Dengue Prevention and Control (2012-2020)
Five key elements:
- Diagnosis and case management
- Integrated surveillance and outbreak preparedness
- Sustainable vector control
- Implementation of future vaccine tools
- Basic operational and implementation research
India's National Programme / GOI Steps
- Monitoring through reports from state health authorities
- Mid-term plan (2011) with components:
- (a) Surveillance (disease + entomological)
- (b) Case management (lab diagnosis + clinical management)
- (c) Vector management (environmental + chemical + personal protection + legislation)
- (d) Outbreak response (epidemic preparedness + media management)
- (e) Capacity building (training + HR strengthening)
- (f) Operational research
- Contingency plan for dengue outbreaks sent to all states since 1996 Delhi outbreak
High-Yield PSM Points (Exam Focus)
| Point | Answer |
|---|---|
| Causative agent | Dengue virus - Flavivirus, RNA virus, 4 serotypes |
| Vector | Aedes aegypti (primary); Aedes albopictus (secondary) |
| Biting time | Daytime (2 hrs post-sunrise + late afternoon) |
| Incubation period | 3-14 days (commonly 4-7 days) |
| Extrinsic incubation period | 8-10 days |
| "Break bone fever" | Dengue fever (due to severe myalgia/arthralgia) |
| Iceberg phenomenon | DF/DHF - majority are asymptomatic |
| Tourniquet test | Positive in DHF (≥10-20 petechiae per inch²) |
| Platelet cut-off for DHF | ≤ 100,000/mm³ |
| Haemoconcentration in DHF | Hct rise ≥ 20% from baseline |
| Pulse pressure in DSS | ≤ 20 mmHg |
| NS1 detects from | Day 1 of illness |
| IgM detects from | Day 5 of illness |
| Vaccine | CYD-TDV (Dengvaxia); 3 doses SC; 6-monthly; age 9-45 yrs |
| Avoid in treatment | Aspirin / NSAIDs |
| Weekly Dry Day | Empty + scrub water containers every week |
| Larvivorous fish | Gambusia, Poecilia |
| Larvicide for stored water | Temephos (Abate) |
| Adult mosquito control | Malathion fogging |
| CFR (India 2019) | 0.1% |
| Global at-risk population | 3.9 billion in 128 countries |
| Annual infections | 390 million; 96 million manifest clinically |
Sources: Park's Textbook of Preventive and Social Medicine; Harrison's Principles of Internal Medicine 22E (2025)
This is a shared conversation. Sign in to Orris to start your own chat.