Pancreatic secretion Short answer thpe
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough short-answer type response. Here it is:
Pancreatic Secretion
Overview
The exocrine pancreas secretes approximately 1 litre of fluid per day into the duodenum. The secretion has two components:
- Aqueous (HCO3- rich) component - secreted by centroacinar and ductal cells
- Enzymatic component - secreted by acinar cells
Both components flow through the pancreatic duct, which joins the common bile duct and empties into the duodenum at the papilla of Vater, surrounded by the sphincter of Oddi.
Enzymatic Component (Acinar Cells)
The pancreas secretes enzymes for digesting all three macronutrients:
Proteolytic Enzymes
| Inactive (Zymogen) | Active Form | Action |
|---|---|---|
| Trypsinogen | Trypsin | Splits proteins/peptides into smaller peptides |
| Chymotrypsinogen | Chymotrypsin | Splits proteins/peptides |
| Procarboxypeptidase | Carboxypeptidase | Cleaves terminal amino acids from peptides |
- Trypsinogen is activated by enterokinase (enteropeptidase) secreted by intestinal mucosa, and also by autocatalysis (trypsin activating more trypsinogen)
- Trypsin then activates chymotrypsinogen and procarboxypeptidase
Carbohydrate-Digesting Enzyme
- Pancreatic amylase - hydrolyzes starch, glycogen (not cellulose) into disaccharides and trisaccharides
Fat-Digesting Enzymes
- Pancreatic lipase - hydrolyzes neutral fats into fatty acids and monoglycerides
- Cholesterol esterase - hydrolyzes cholesterol esters
- Phospholipase - splits fatty acids from phospholipids
Trypsin Inhibitor - Self-Protection Mechanism
Proteolytic enzymes are stored as inactive zymogens to prevent autodigestion. Pancreatic cells also secrete trypsin inhibitor, which inactivates any trypsin accidentally formed inside the pancreas or its ducts. Failure of this mechanism leads to acute pancreatitis.
Aqueous (HCO3-) Component (Ductal Cells)
- Centroacinar and ductal cells secrete a Na+/HCO3--rich, isosmotic solution
- Function: Neutralizes the acidic chyme arriving from the stomach, bringing duodenal pH to ~7, which is optimal for pancreatic enzyme activity (especially lipase, which is inactivated at low pH)
- HCO3- secretion is directly proportional to flow rate - at high flow rates, HCO3- is ~150 mEq/L; at low flow rates, Cl- predominates
Regulation of Pancreatic Secretion
Three basic stimuli regulate secretion:
| Stimulus | Source | Target Cell | Effect |
|---|---|---|---|
| Acetylcholine (ACh) | Vagus nerve / enteric nervous system | Acinar cells | Enzyme secretion |
| Cholecystokinin (CCK) | I cells of duodenum/jejunum | Acinar cells | Enzyme secretion |
| Secretin | S cells of duodenum/jejunum | Ductal cells | HCO3- and water secretion |
Second messengers:
- CCK and ACh act via IP3 / Ca2+ pathway on acinar cells
- Secretin acts via cAMP pathway on ductal cells
Potentiation: All three stimuli act synergistically - the combined effect is far greater than the sum of individual effects.
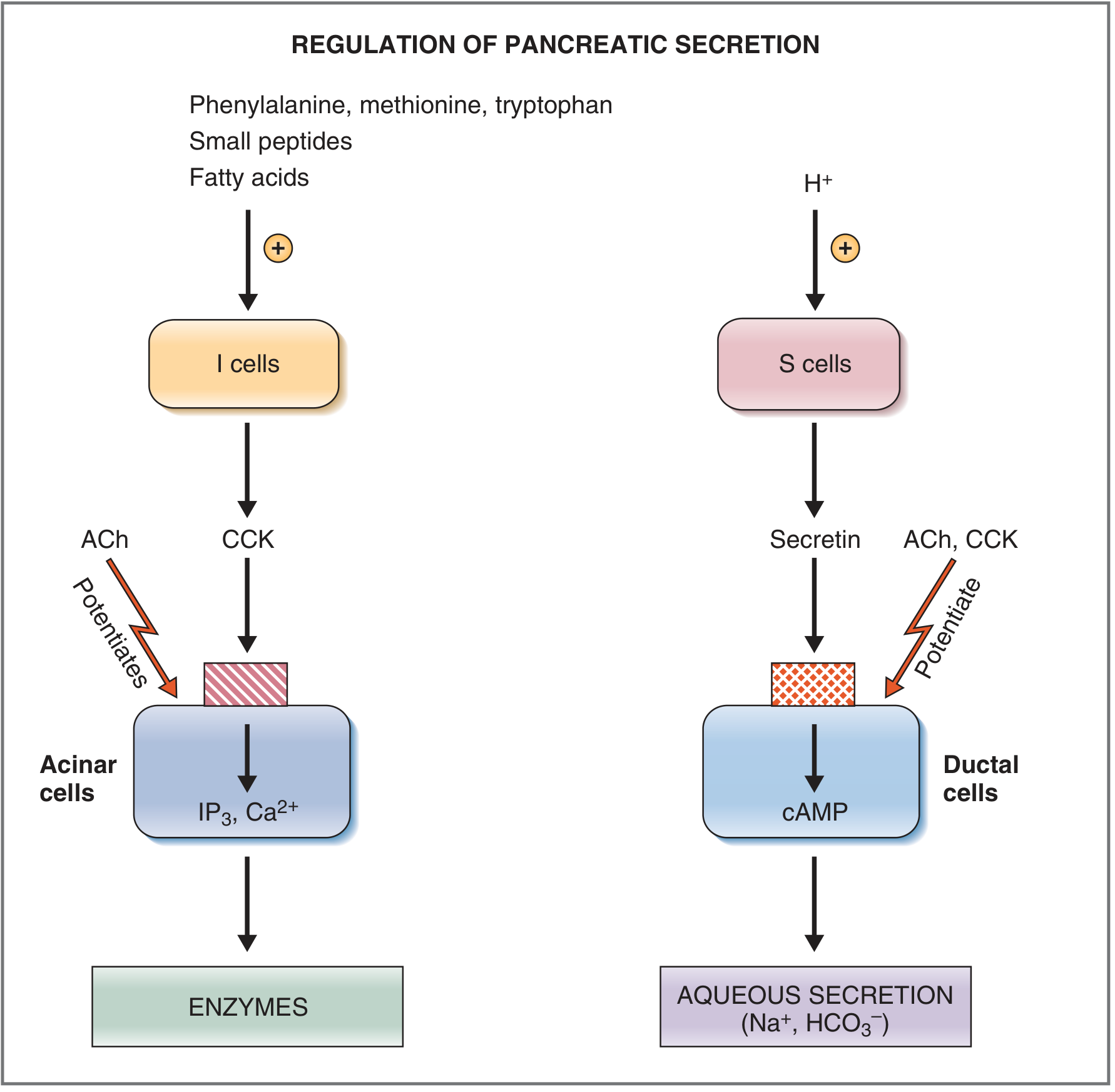
Triggers for Hormone Release:
- CCK release is stimulated by: amino acids (especially phenylalanine, methionine, tryptophan), small peptides, and fatty acids in the duodenum
- Secretin release is stimulated by: HCl (acidic chyme, pH < 4.5-5.0) in the duodenum; it is present as inactive prosecretin in S cells
Phases of Pancreatic Secretion
| Phase | Mediator | Secretion Type | Contribution |
|---|---|---|---|
| Cephalic | Vagus nerve (sight, smell, taste) | Mainly enzymatic | ~20% of total enzymes |
| Gastric | Vagus nerve (gastric distension) | Mainly enzymatic | ~5-10% of total enzymes |
| Intestinal | CCK + Secretin + ACh | Both enzymatic and aqueous | ~70-80% of total secretion |
The intestinal phase is the most important phase, dominated by the action of secretin (for aqueous secretion) and CCK (for enzyme secretion).
Inhibition of Pancreatic Secretion
- Peptide YY (from ileal endocrine cells) - inhibits secretion when fat reaches the distal small intestine (the "ileal brake")
- Somatostatin - inhibits secretion
- Sympathetic activity - inhibits pancreatic secretion (contrast: parasympathetic stimulates)
Sources: Guyton and Hall Textbook of Medical Physiology, p.805-807; Costanzo Physiology 7th Edition, p.371-374
In flow charts
Here are the key concepts of Pancreatic Secretion presented as flowcharts:
1. Overview of Pancreatic Secretion
PANCREAS (Exocrine)
│
├─────────────────────────────────────────┐
│ │
ACINAR CELLS CENTROACINAR + DUCTAL CELLS
│ │
ENZYMATIC COMPONENT AQUEOUS COMPONENT
(Digestive enzymes) (HCO₃⁻ + Na⁺ + H₂O)
│ │
└──────────────┬──────────────────────────┘
│
PANCREATIC DUCT
│
COMMON BILE DUCT
│
PAPILLA OF VATER
│
DUODENUM (via Sphincter of Oddi)
2. Enzymatic Component - Activation of Zymogens
ACINAR CELLS secrete INACTIVE ZYMOGENS
│
┌───────────┼────────────────┐
│ │ │
Trypsinogen Chymotrypsinogen Procarboxypeptidase
│
▼
Reaches DUODENUM
│
├──── Enterokinase (from intestinal mucosa) ──► TRYPSIN
│
└──── Autocatalysis (Trypsin activates itself)
│
TRYPSIN activates
│
┌───────────┴───────────────┐
│ │
Chymotrypsinogen Procarboxypeptidase
│ │
Chymotrypsin Carboxypeptidase
│ │
(splits proteins (releases free
into peptides) amino acids)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
TRYPSIN INHIBITOR (secreted by acinar cells)
→ Inactivates any accidental trypsin inside the pancreas
→ Failure → ACUTE PANCREATITIS
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
3. Enzymes by Substrate
CARBOHYDRATES PROTEINS FATS
│ │ │
Pancreatic Amylase Trypsin Pancreatic Lipase
│ Chymotrypsin Cholesterol Esterase
▼ Carboxypeptidase Phospholipase
Disaccharides + │ │
Trisaccharides ▼ ▼
Peptides + Fatty Acids +
Amino acids Monoglycerides +
Cholesterol
4. Regulation - Stimuli & Second Messengers
FOOD IN DUODENUM
│
┌────┴────────────────────────────────┐
│ │
Amino acids / Peptides / Acidic Chyme (pH < 4.5)
Fatty acids │
│ │
▼ ▼
I cells (duodenum/jejunum) S cells (duodenum/jejunum)
│ │
CCK released SECRETIN released
into blood into blood
│ │
▼ ▼
ACINAR CELLS DUCTAL CELLS
(CCK-A receptors) (Secretin receptors)
│ │
IP₃ / Ca²⁺ pathway cAMP pathway
│ │
▼ ▼
ENZYME SECRETION HCO₃⁻ + H₂O SECRETION
(Proteases, Lipase, Amylase) (Neutralizes gastric acid)
↑ POTENTIATED BY ↑
Acetylcholine (ACh)
(Vagus nerve)
Acts on BOTH acinar & ductal cells
5. Phases of Pancreatic Secretion
MEAL INGESTION
│
▼
CEPHALIC PHASE (~20% of enzyme output)
Trigger: Sight / Smell / Taste / Thought of food
Mediator: Vagus nerve → ACh
Product: Mainly ENZYMES (little fluid)
│
▼
GASTRIC PHASE (~5–10% of enzyme output)
Trigger: Gastric distension
Mediator: Vagal reflex → ACh
Product: Mainly ENZYMES (little fluid)
│
▼
INTESTINAL PHASE (~70–80% of total secretion) ← MOST IMPORTANT
Trigger: Chyme enters duodenum
│
├── H⁺ (acid) → Secretin → DUCTAL CELLS → HCO₃⁻ secretion
│
└── Amino acids / Fatty acids → CCK → ACINAR CELLS → ENZYME secretion
+ ACh (vagovagal reflex) potentiates both
6. Inhibition of Pancreatic Secretion
Fat in DISTAL small intestine (ileum)
│
▼
Peptide YY (from ileal cells)
│
▼
INHIBITS pancreatic secretion
│
(also: Somatostatin)
│
(also: Sympathetic NS activity)
→ Signals end of intestinal phase of digestion
→ "ILEAL BRAKE" mechanism
7. Summary - One Glance
STIMULUS → HORMONE/NERVE → CELL TYPE → SECOND MESSENGER → PRODUCT
H⁺ in duodenum → SECRETIN (S cells) → Ductal cells → cAMP → HCO₃⁻ + H₂O
AA/FA in duodenum → CCK (I cells) → Acinar cells → IP₃/Ca²⁺ → ENZYMES
Sight/smell/distension → ACh (Vagus) → Both cells → IP₃/Ca²⁺/cAMP → ENZYMES + HCO₃⁻
Fat in ileum → Peptide YY → ↓ Secretion (inhibition)
These flowcharts cover the full short-answer scope: components, enzyme activation, regulation (hormonal + neural), phases, and inhibition. All content sourced from Guyton & Hall Medical Physiology and Costanzo Physiology 7th Edition.
Calcium metabolism physiology
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the content needed. Let me compile the comprehensive flowchart-based answer on Calcium Metabolism Physiology.
Calcium Metabolism - Physiology (Flowcharts)
1. Distribution of Calcium in the Body
TOTAL BODY CALCIUM (~1000 g)
│
┌──────┴───────────────────────────┐
│ │
BONE (~99%) SOFT TISSUES (~1%)
(Reservoir) Cells + ECF
│ │
├─ Structural (99.6%) ├─ Intracellular (~1%)
│ (Hydroxyapatite) └─ Extracellular fluid (~0.1%)
└─ Exchangeable (0.4-1%) ↓
(CaHPO₄, amorphous salts) Normal ECF = 9.4 mg/dL
← Rapid buffer pool (2.4 mmol/L)
2. Forms of Calcium in Plasma
TOTAL PLASMA CALCIUM (9.4 mg/dL)
│
┌─────────┼──────────────────────┐
│ │ │
Protein- Complexed IONIZED Ca²⁺
bound with anions (50%) ← PHYSIOLOGICALLY ACTIVE
(41%) (PO₄, citrate)
(9%)
↑ Alkalosis → ↑ protein binding → ↓ free Ca²⁺ → Tetany
↓ Albumin → ↓ total Ca²⁺ (but ionized Ca²⁺ may be normal)
3. Vitamin D Activation Pathway
SUNLIGHT (UV-B)
│
▼
SKIN: 7-Dehydrocholesterol
│
▼
Vitamin D₃ (Cholecalciferol) ← also from diet
│
▼ (25-hydroxylase)
LIVER
│
▼
25-Hydroxycholecalciferol (calcidiol) ← storage form; serum marker of Vit D status
│
▼ (1α-hydroxylase) ← KEY REGULATORY STEP
KIDNEY
│
├── STIMULATED by: ↓Ca²⁺, ↓PO₄, ↑PTH
└── INHIBITED by: ↑Ca²⁺, ↑PO₄, ↑1,25-(OH)₂D₃ (feedback)
│
▼
1,25-Dihydroxycholecalciferol (Calcitriol) ← ACTIVE FORM
│
├── Intestine: ↑Ca²⁺ + PO₄ absorption (via calbindin)
├── Bone: ↑Ca²⁺ + PO₄ mobilization (with PTH)
└── Kidney: ↑Ca²⁺ reabsorption (minor)
When Ca²⁺ is HIGH → 25-OH-D → 24,25-(OH)₂D (inactive form)
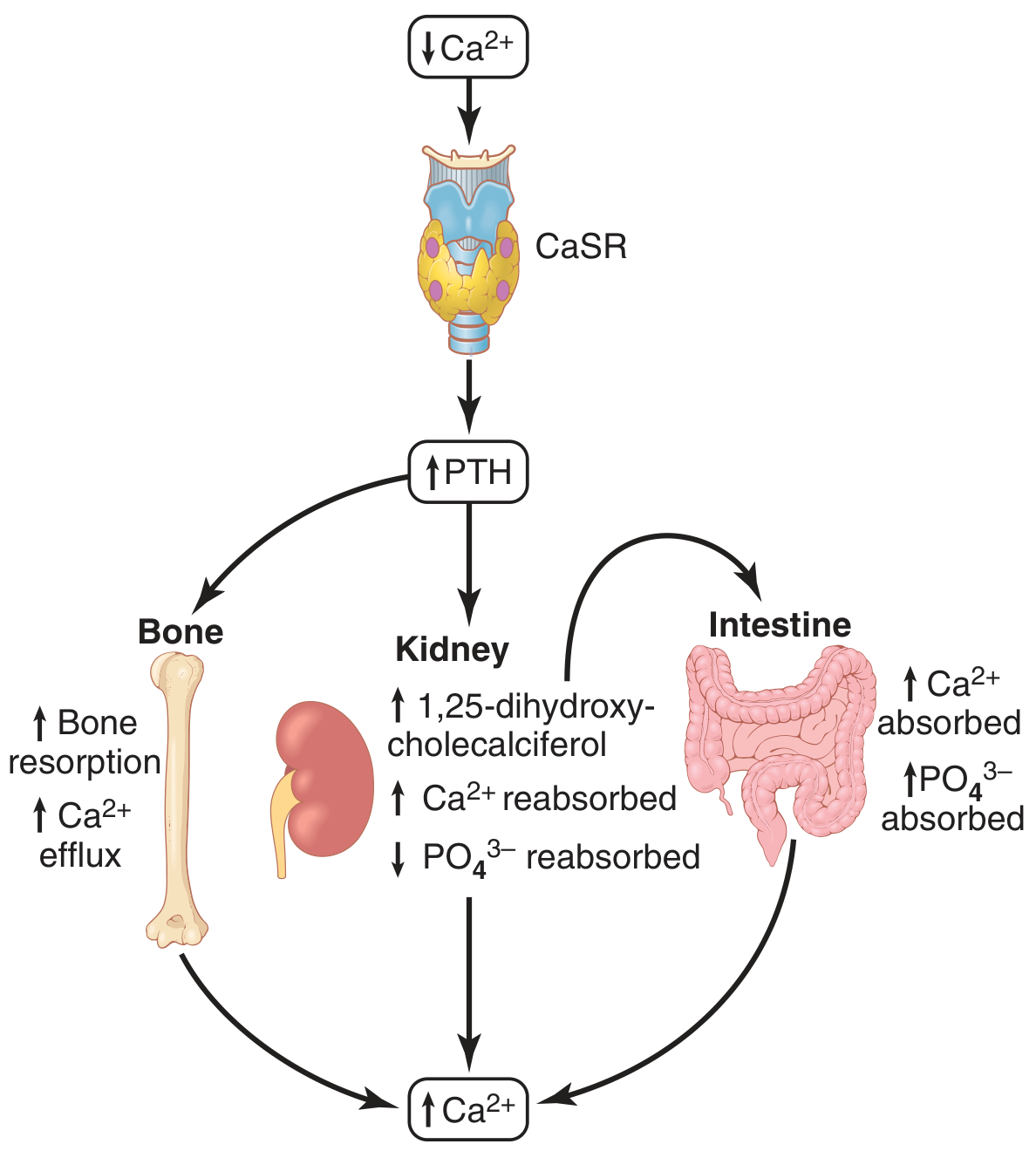
4. PTH - Synthesis, Stimulus & Actions
↓ Plasma Ca²⁺ (< 9 mg/dL)
│
▼
PARATHYROID GLANDS
(detect via CaSR - Calcium-Sensing Receptor)
│
CaSR (G protein-coupled) senses ↓Ca²⁺
│
▼
↑ PTH SECRETED (84 amino acid peptide)
Second messenger: cAMP
│
┌────┴─────────────────────────────────────────┐
│ │ │
BONE KIDNEY INTESTINE
│ │ │
↑ Bone resorption ↑ Ca²⁺ reabsorption ↑ Ca²⁺ absorption
(Osteoclast (distal tubule) (INDIRECT - via
activation via ↑1,25-(OH)₂D₃)
RANKL/RANK) ↓ PO₄ reabsorption
│ (proximal tubule)
↑ Ca²⁺ + PO₄ ↑1α-hydroxylase
into blood → ↑ Calcitriol
│ │
└──────┬───────────┘
▼
↑ Plasma Ca²⁺
│
NEGATIVE FEEDBACK
│
▼
↓ PTH secretion
5. PTH Effects on Bone - Two Phases
PTH ACTS ON BONE
│
┌────┴─────────────────────────────────────────────┐
│ │
RAPID PHASE (minutes-hours) SLOW PHASE (days-weeks)
│ │
Activates existing osteocytes Proliferation of osteoclasts
+ osteoblasts (osteolysis) │
│ RANKL (from osteoblasts) + M-CSF
▼ │
Calcium pumped out of bone fluid ▼
into extracellular fluid Osteoclast-mediated bone
resorption (true resorption)
│
↑↑ Ca²⁺ + PO₄ into blood
6. Calcitonin - Counter-Regulatory Hormone
↑ Plasma Ca²⁺ (> 9-10 mg/dL)
│
▼
THYROID GLAND (Parafollicular / C cells)
│
▼
↑ CALCITONIN SECRETED (32 amino acid peptide)
│
┌────┴────────────────────┐
│ │
BONE KIDNEY
│ │
↓ Osteoclast activity ↓ Ca²⁺ & PO₄
↓ Bone resorption reabsorption (minor)
↑ Ca²⁺ deposition
│
▼
↓ Plasma Ca²⁺
Note: Calcitonin effect is TRANSIENT and WEAK in adult humans
(PTH overrides with compensatory ↑)
7. Calcium Balance - Daily Flux
DIETARY INTAKE: ~1000 mg/day
│
▼
INTESTINAL ABSORPTION (~350 mg absorbed, ~150 mg secreted back)
Net absorption = 200 mg/day (regulated by Vit D)
│
▼
EXTRACELLULAR FLUID POOL (~1300 mg)
│
┌────┴───────────────────────┐
│ │
BONE exchange KIDNEY
(500 mg/day in & out) ~10,000 mg filtered/day
(rapid buffer) 98% reabsorbed
│ ↓
│ ~200 mg excreted in urine
│
└── FECAL loss ~800 mg/day (unabsorbed + secreted)
8. Renal Handling of Calcium
GLOMERULAR FILTRATION: ~59% of plasma Ca²⁺ filtered
(ionized 50% + complexed 9%)
│
▼
PROXIMAL TUBULE (60-70% reabsorbed) ← passive, paracellular
│
▼
LOOP OF HENLE (20% reabsorbed)
│
▼
EARLY DISTAL TUBULE (10% reabsorbed)
│
▼
LATE DISTAL TUBULE / COLLECTING DUCT (variable ~5-10%)
← THIS IS THE REGULATED STEP ←
PTH → ↑ Ca²⁺ reabsorption
↑ Ca²⁺ → ↓ Ca²⁺ reabsorption
│
▼
URINE: ~200 mg/day excreted
9. Integrated Feedback Loop - Summary
↓ Ca²⁺ (hypocalcemia)
│
┌──────┴──────────────────────────────┐
│ │
↑ PTH secretion ↑ Calcitriol (1,25-OH₂D₃)
(parathyroid) (kidney, stimulated by PTH)
│ │
┌────┴──────────────┐ ┌───────┴────────────┐
│ │ │ │
BONE KIDNEY INTESTINE BONE
↑ Resorption ↑ Ca²⁺ reabsorp ↑ Ca²⁺ absorp ↑ Ca²⁺ mob.
↑ Ca²⁺ into ECF ↓ PO₄ reabsorp
│
▼
↑ PLASMA Ca²⁺ ← RESTORED
│
Negative feedback:
CaSR on parathyroid →
↓ PTH → equilibrium restored
↑ Ca²⁺ (hypercalcemia)
│
↑ Calcitonin (C cells of thyroid)
│
↓ Osteoclast activity
↑ Ca²⁺ deposition in bone
│
▼
↓ Plasma Ca²⁺ ← restored
10. Key Hormones at a Glance
HORMONE │ SOURCE │ Trigger │ Effect on Ca²⁺ │ Effect on PO₄
────────────────────────────────────────────────────────────────────────────────
PTH │ Parathyroid │ ↓ Ca²⁺ │ ↑ (raise) │ ↓ (lower)
Calcitriol │ Kidney (Vit D) │ ↑ PTH / ↓Ca²⁺ │ ↑ (raise) │ ↑ (raise)
Calcitonin │ C cells/Thyroid │ ↑ Ca²⁺ │ ↓ (lower) │ ↓ (lower)
Source: Guyton and Hall Textbook of Medical Physiology, Ch. 80 (p.979-992)
In short answer type
Here is Calcium Metabolism Physiology in short answer type format:
Calcium Metabolism - Physiology
1. Normal Values
- Total plasma calcium: 9.4 mg/dL (2.4 mmol/L)
- Only ionized Ca²⁺ (50%) is physiologically active
- The rest: protein-bound (41%) + complexed with anions (9%)
- Total body calcium: ~1000 g; 99% in bone, <1% in ECF
2. Forms of Calcium in Plasma
| Form | % | Notes |
|---|---|---|
| Ionized (free) Ca²⁺ | 50% | Active form; regulated |
| Protein-bound (mainly albumin) | 41% | Inactive; affected by albumin levels |
| Complexed (PO₄, citrate) | 9% | Inactive |
Key point: Alkalosis → ↑ protein binding → ↓ free Ca²⁺ → tetany despite normal total Ca²⁺
3. Vitamin D Activation
Skin (UV-B) → Vitamin D₃ (Cholecalciferol)
→ Liver (25-hydroxylase) → 25-OH Cholecalciferol (storage form)
→ Kidney (1α-hydroxylase) → 1,25-(OH)₂ Cholecalciferol (Calcitriol) ← ACTIVE FORM
Renal 1α-hydroxylase is stimulated by:
- ↓ Plasma Ca²⁺
- ↓ Plasma PO₄
- ↑ PTH
When Ca²⁺ is high: 25-OH-D → 24,25-(OH)₂D (inactive form) instead
Actions of Calcitriol:
- Intestine → ↑ Ca²⁺ + PO₄ absorption (via calbindin synthesis)
- Bone → ↑ Ca²⁺ mobilization (with PTH)
- Kidney → ↑ Ca²⁺ reabsorption (minor)
4. Parathyroid Hormone (PTH)
Source: Chief cells of parathyroid glands
Structure: 84 amino acid peptide
Trigger: ↓ plasma Ca²⁺ detected by CaSR (calcium-sensing receptor) - a G-protein coupled receptor
Second messenger: cAMP
Actions of PTH:
| Organ | Effect on Ca²⁺ | Effect on PO₄ |
|---|---|---|
| Bone | ↑ resorption (osteoclast activation via RANKL) → ↑ Ca²⁺ release | ↑ PO₄ release |
| Kidney | ↑ reabsorption (distal tubule) | ↓ reabsorption (phosphaturic effect) |
| Kidney | ↑ 1α-hydroxylase → ↑ Calcitriol | - |
| Intestine | ↑ absorption (indirect, via calcitriol) | ↑ absorption |
Net result: ↑ Ca²⁺, ↓ PO₄ in plasma
PTH Bone Effects - Two Phases:
- Rapid (minutes-hours): Activates osteocytes → osteolysis (Ca²⁺ pumped out of bone fluid)
- Slow (days-weeks): Osteoclast proliferation via RANKL/RANK → true bone resorption
Feedback Control of PTH:
- ↓ Ca²⁺ → ↑ PTH → restores Ca²⁺ (negative feedback loop)
- Even a few % drop in Ca²⁺ can cause 100% increase in PTH
- Chronic low Ca²⁺ → parathyroid gland hypertrophy
5. Calcitonin
Source: Parafollicular cells (C cells) of thyroid gland
Structure: 32 amino acid peptide
Trigger: ↑ plasma Ca²⁺
Actions:
- Bone: ↓ osteoclast activity → ↓ bone resorption → ↑ Ca²⁺ deposition → ↓ plasma Ca²⁺
- Kidney: ↓ Ca²⁺ + PO₄ reabsorption (minor effect)
Important: Calcitonin effect is transient and weak in adult humans. PTH is the dominant regulator. Calcitonin is more significant in children and young animals.
6. Daily Calcium Balance
| Process | Amount |
|---|---|
| Dietary intake | ~1000 mg/day |
| Intestinal absorption | ~350 mg absorbed |
| Intestinal secretion | ~150 mg back into gut |
| Net absorption | ~200 mg/day |
| Urinary excretion | ~200 mg/day |
| Fecal loss | ~800 mg/day |
- Kidneys filter ~10,000 mg/day; 98% reabsorbed
- The late distal tubule is the regulated step - controlled by PTH
7. Bone as a Calcium Buffer
- Exchangeable calcium in bone = 0.4-1% of total bone calcium
- In the form of amorphous salts (CaHPO₄)
- Rapidly equilibrates with ECF Ca²⁺
- Acts as rapid buffer - restores Ca²⁺ within 30-60 minutes of sudden change
8. Summary Table - Three Hormones
| PTH | Calcitriol (Vit D) | Calcitonin | |
|---|---|---|---|
| Source | Parathyroid gland | Kidney | Thyroid C cells |
| Trigger | ↓ Ca²⁺ | ↑ PTH / ↓ Ca²⁺ | ↑ Ca²⁺ |
| Ca²⁺ effect | ↑ Raise | ↑ Raise | ↓ Lower |
| PO₄ effect | ↓ Lower | ↑ Raise | ↓ Lower |
| Main site | Bone + Kidney | Intestine | Bone |
9. Clinical Correlates (Exam Points)
| Condition | Mechanism | Ca²⁺ | PO₄ | PTH |
|---|---|---|---|---|
| Hypoparathyroidism | ↓ PTH | ↓ | ↑ | ↓ |
| Hyperparathyroidism | ↑ PTH | ↑ | ↓ | ↑ |
| Vitamin D deficiency | ↓ Ca²⁺ absorption | ↓ | ↓ | ↑ (secondary) |
| Renal failure | ↓ 1α-hydroxylase | ↓ | ↑ | ↑ (secondary) |
| Hypocalcemia | ↓ free Ca²⁺ | Tetany, ↑ neuroexcitability | - | - |
| Hypercalcemia | ↑ free Ca²⁺ | CNS depression, ↓ neuroexcitability | - | - |
Source: Guyton and Hall Textbook of Medical Physiology, Ch. 80
This is a shared conversation. Sign in to Orris to start your own chat.