Perioperative acute kidney injury for 10 marks dnb exam
Reading File
Finding Sources
Finding Sources
Searching PubMed
"perioperative acute kidney injury" AND prevention
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, textbook-backed content to write a thorough 10-mark DNB answer. Here it is:
Perioperative Acute Kidney Injury (10 Marks - DNB)
Definition and Incidence
Acute kidney injury (AKI) - previously termed acute renal failure - is characterized by a rapid decline in glomerular filtration rate (GFR) with accumulation of nitrogenous waste products (BUN and creatinine). AKI occurs in approximately 5-25% of all hospitalized patients and in 1-7% of patients after cardiac or major vascular surgery. Mortality ranges from 10-35% for mild AKI and 50-80% in the ICU setting.
- Miller's Anesthesia, 10e
Diagnostic Criteria / Staging (KDIGO 2012)
The three widely used systems - RIFLE, AKIN, and KDIGO - share the same urine output criteria:
| Stage | Serum Creatinine Criteria | Urine Output |
|---|---|---|
| Stage 1 | Rise ≥0.3 mg/dL in <48 h, OR ≥50% rise in <7 days | <0.5 mL/kg/h for >6 hours |
| Stage 2 | Rise ≥100% (2x baseline) | <0.5 mL/kg/h for >12 hours |
| Stage 3 | Rise ≥200% (3x baseline) or need for RRT | <0.3 mL/kg/h for >24 h or anuria >12 h |
RIFLE additionally includes Loss (RRT >4 weeks) and End-stage (RRT >3 months).
The KDIGO definition requires either criterion to be met: an absolute rise of >0.3 mg/dL within 48 hours OR a relative rise of >50% within 7 days.
- Brenner and Rector's The Kidney, p. 1244-1245
Risk Factors
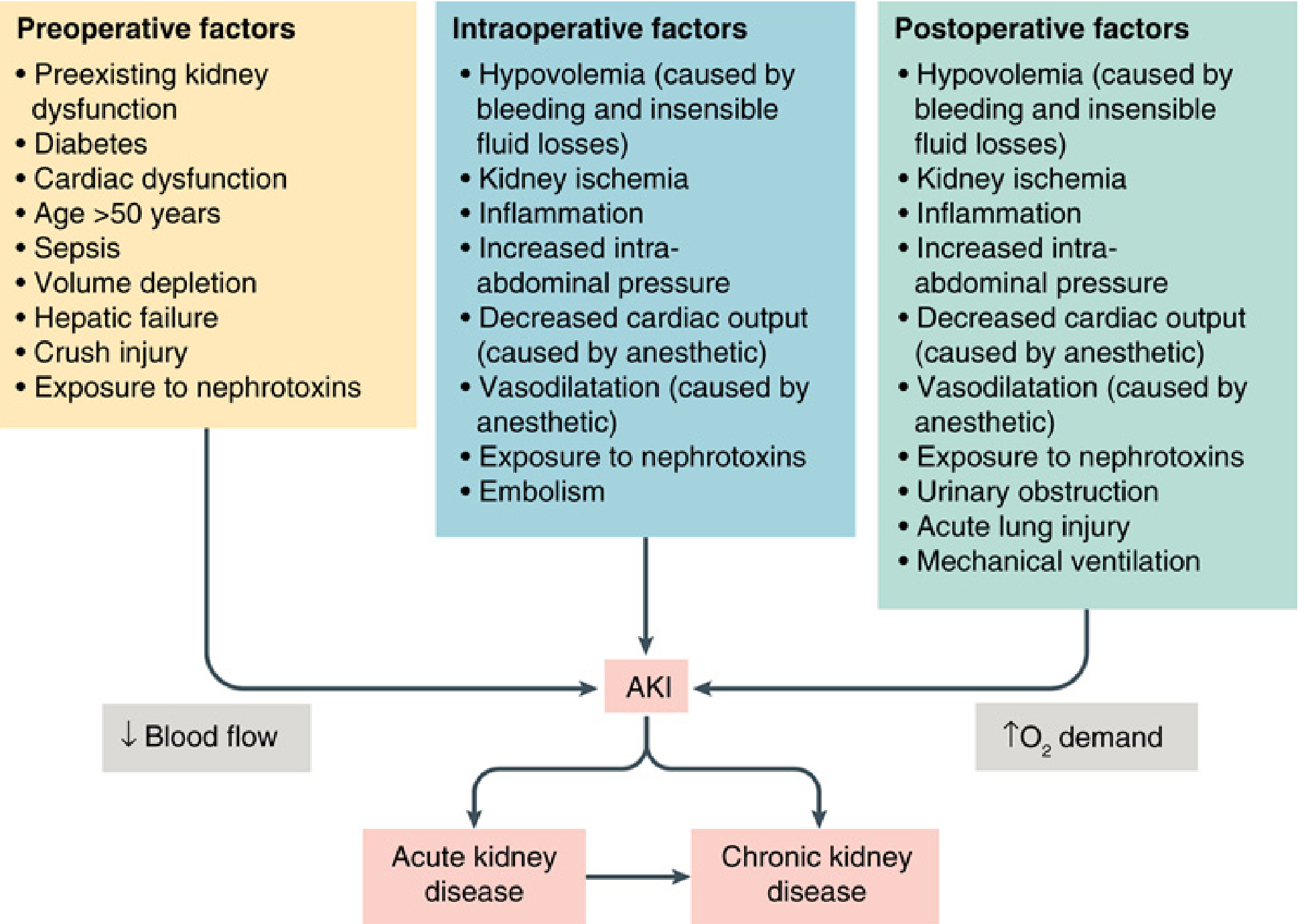
Preoperative:
- Pre-existing kidney dysfunction / CKD
- Diabetes mellitus, age >50 years
- Cardiac dysfunction, hepatic failure
- Sepsis, volume depletion
- Crush injury, prior nephrotoxin exposure
Intraoperative:
- Hypovolemia (bleeding, insensible losses)
- Kidney ischemia, intraoperative hypotension
- Inflammation (surgical stress)
- Increased intra-abdominal pressure
- Decreased cardiac output (anesthetic effect)
- Vasodilatation (anesthetic effect)
- Embolism (atheroemboli, air embolism)
- Nephrotoxin exposure
Postoperative:
-
Continued hypovolemia and ischemia
-
Urinary obstruction
-
Acute lung injury / mechanical ventilation
-
Ongoing inflammation
-
Miller's Anesthesia, 10e, Fig. 38.1
Pathophysiology
The primary cause of perioperative AKI is acute tubular necrosis (ATN). The mechanisms are multifactorial and commonly involve:
1. Ischemia-Reperfusion Injury
- The kidney's outer medulla is susceptible to ischemia due to its high metabolic demand and marginal oxygen supply (medullary pO2 ~10-20 mmHg at baseline).
- Anesthetic agents cause vasodilation and negative inotropy, reducing renal blood flow (RBF).
- Intraoperative hypotension with mean arterial pressure (MAP) below the autoregulatory threshold leads to a fall in GFR. The renal cortex is primarily supplied by the peritubular capillary network, and ischemia-reperfusion injury damages the S3 segment of the proximal tubule.
- Reperfusion generates reactive oxygen species (ROS) causing further cellular damage.
2. Inflammation
- Surgery activates the systemic inflammatory response (SIRS) via complement, cytokines (TNF-α, IL-1, IL-6), and neutrophil-endothelial adhesion.
- Inflammatory mediators cause afferent arteriolar vasoconstriction and tubular epithelial injury.
3. Nephrotoxin-Mediated Injury
- Nephrotoxins disturb either renal O2 delivery or utilization and promote ischemia.
- Key culprits: aminoglycoside antibiotics, amphotericin B, radiocontrast agents, NSAIDs, cyclosporine/tacrolimus, ACE inhibitors/ARBs, myoglobin (rhabdomyolysis), free hemoglobin.
- Barash Clinical Anesthesia, 9e
4. Hemodynamic Prerenal Mechanism
- Prerenal azotemia is the commonest precursor. The kidney maximizes solute/water retention, but if hypoperfusion persists, ATN supervenes.
- ACE inhibitors and ARBs impair glomerular efferent arteriolar tone, reducing GFR during low-flow states.
5. Atheroembolism
- Especially relevant in vascular surgery (aortic cross-clamping) - cholesterol crystal emboli occlude small renal vessels.
Causes - Classification
| Category | Examples |
|---|---|
| Prerenal | Hypovolemia (bleeding, third-space), sepsis, cardiac failure, low CO from CPB, hepatorenal syndrome, aortic cross-clamping, increased IAP |
| Renal (Intrinsic) | Inflammation/sepsis, CKD + comorbidities, endogenous toxins (myoglobin), exogenous toxins (contrast dyes), blood transfusions, chloride-rich/HES solutions |
| Postrenal | Ureteric/bladder/urethral obstruction, BPH, neurogenic bladder, surgical injury |
- Bailey & Love's Short Practice of Surgery, 28e, Table 24.4
Effects of Anesthetic Techniques
Regional Anesthesia
- Neuraxial blocks reduce sympathetic tone (T4-L1) innervating the renal vasculature. If hypotension results, RBF falls. Meta-analysis data suggest a 30% reduction in odds of postoperative mortality with neuraxial blockade (Rodgers et al.), with some reduction in renal failure, though confidence intervals were wide.
Inhaled Anesthetics
- Methoxyflurane and enflurane (historical) caused fluoride-induced polyuric renal insufficiency. Sevoflurane generates inorganic fluoride and compound A but is NOT associated with clinically significant AKI - likely due to shorter duration of fluoride elevation and lower intrarenal metabolism compared to methoxyflurane.
Intravenous Anesthetics
-
Propofol increases bone morphogenetic protein-7 (BMP-7), which suppresses TNF-α-induced inflammatory cascade in sepsis-induced AKI and reduces ischemia-reperfusion injury.
-
Dexmedetomidine (α2-adrenoceptor agonist) - meta-analysis data suggest a reduction in postoperative AKI; may stimulate BMP-7 in sepsis/ischemia-reperfusion models.
-
Miller's Anesthesia, 10e
Biomarkers
| Marker | Basis |
|---|---|
| Serum creatinine | Standard; lags 24-48 h behind injury |
| Cystatin C | More sensitive for mild CKD; inconsistent for perioperative AKI |
| NGAL (Neutrophil gelatinase-associated lipocalin) | Early tubular damage marker; rises within hours of injury |
| KIM-1 (Kidney injury molecule-1) | Proximal tubule damage |
| IGFBP7 × TIMP-2 (NephroCheck) | Cell cycle arrest markers; predict AKI 12 h before SCr rise |
| L-FABP, α-GST, π-GST | Tubular enzymuria |
| penKid (proenkephalin A 119-159) | Correlated with GFR; associated with adverse outcomes in critical illness |
Nephrotoxic Drug Considerations (Key Perioperative Points)
- ACE inhibitors/ARBs: Should be withheld 48 hours before elective cardiac surgery - meta-analysis of >50,000 procedures links continuation to higher mortality (20%) and AKI rates (17%).
- NSAIDs: Impair prostaglandin-mediated renal autoregulation; risk magnified in volume depletion.
- Loop diuretics: Chronic therapy and high-dose furosemide independently associated with postoperative AKI.
- Radiocontrast: AKI risk 24-48 h after exposure, peaks at 3-5 days. Mitigation: pre-hydration, minimize contrast dose, withhold NSAIDs/nephrotoxins.
- Statins (protective): Pre-CABG statin use associated with lower dialysis and mortality rates (meta-analysis of 17 studies, >47,000 patients).
- Aminoglycosides/Amphotericin B: Avoid concomitant hypovolemia, fever, other nephrotoxins; monitor electrolytes (hypomagnesemia, hypokalemia worsen toxicity).
- Barash Clinical Anesthesia, 9e
Prevention / Management
General Principles
- Hemodynamic optimization: Maintain MAP above autoregulatory threshold; avoid intraoperative hypotension. Goal-directed therapy (GDT) is beneficial, but overly restrictive fluid protocols have recently been associated with increased AKI risk - balance is key.
- Fluid choice: Balanced salt solutions preferred over normal saline - avoids hyperchloremic metabolic acidosis; may modestly reduce AKI rates.
- Avoid volume overload: Volume overload is an independent risk factor for adverse AKI outcomes.
- Minimize nephrotoxin exposure: Hold ACE inhibitors/ARBs perioperatively; avoid NSAIDs; use ISO-osmolar/low-osmolarity contrast; monitor aminoglycoside levels.
- Urine output monitoring: Carefully monitor intraoperative urine output, though it is not validated as a sole predictor of postoperative renal dysfunction.
Pharmacological Interventions with Evidence
| Agent | Status |
|---|---|
| Mannitol (before aortic clamping) | Clinical trials FAILED to show benefit |
| Dopamine (renal-dose) | NOT associated with improved mortality |
| Atrial natriuretic peptide | NOT associated with improved mortality |
| Fenoldopam (selective DA1 agonist) | May reduce postoperative AKI incidence, but NO reduction in need for RRT or hospital mortality |
| Dexmedetomidine | Meta-analysis suggests potential AKI reduction |
| N-acetylcysteine | No benefit in cardiac surgery RCTs |
- Miller's Anesthesia, 10e
Renal Replacement Therapy (RRT)
- Indicated for severe AKI with refractory hyperkalemia, acidosis, uremia, or volume overload.
- Does not prevent AKI, but treats its metabolic consequences.
- Current evidence does not support early initiation of dialysis or one modality (CRRT vs. IHD) over another.
- Up to 75% of survivors of AKI after major vascular surgery regain kidney function and become dialysis-independent.
- Miller's Anesthesia, 10e
Outcomes and Long-term Consequences
- AKI increases risk of acute kidney disease (AKD) and progression to CKD.
- Even minor elevation in serum creatinine postoperatively correlates with increased short-term mortality.
- After cardiac/major vascular surgery: AKI requiring dialysis is associated with 30-day mortality significantly higher than those without AKI.
- KDIGO defines AKD as AKI or reduction in GFR <60 mL/min/1.73m² or a 35% GFR decrease or >50% SCr increase, lasting <3 months - a bridging category between AKI and CKD.
Summary Points for Exam
- KDIGO defines AKI as SCr rise ≥0.3 mg/dL in 48h OR ≥50% in 7 days OR UO <0.5 mL/kg/h for >6h.
- Primary mechanism of perioperative AKI is ATN, via ischemia-reperfusion, inflammation, and nephrotoxins.
- Perioperative AKI is a mosaic of pure nephropathies; no single treatment reverses it.
- Sevoflurane is safe; avoid methoxyflurane/enflurane (historical).
- Withhold ACE inhibitors/ARBs 48h before cardiac surgery.
- Balanced crystalloids preferred over saline; avoid HES.
- No proven pharmacological renoprotection exists - hemodynamic optimization is the mainstay.
- Dopamine and ANP are NOT renoprotective.
Sources: Miller's Anesthesia, 10e (Ch. 38 & 55); Barash Clinical Anesthesia, 9e (Ch. 50); Bailey & Love's Surgery, 28e (Table 24.4); Brenner & Rector's The Kidney (Table 29.2)
This is a shared conversation. Sign in to Orris to start your own chat.