Meniers disease
Reading File
Finding Sources
Searching PubMed
"Meniere disease"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the complete answer.
Meniere's Disease
A chronic inner ear disorder characterized by the classic tetrad of episodic vertigo, fluctuating sensorineural hearing loss, tinnitus, and aural fullness, caused by endolymphatic hydrops in the membranous labyrinth.
Epidemiology & Overview
- Prevalence roughly 0.2% of the population; onset typically in 4th-5th decade
- Unilateral in 85% of cases initially; however, the second ear is affected in about 20-40% of patients over time, usually within 36 months of first-ear onset
- Natural history: spontaneous remission of vertigo occurs in ~57% within 2 years and ~71% by 8 years
Pathophysiology
The hallmark pathologic finding is endolymphatic hydrops - over-accumulation of endolymph that distends the membranous labyrinth at the expense of the perilymphatic space. On histopathology, Reissner's membrane is seen ballooning into the scala tympani.
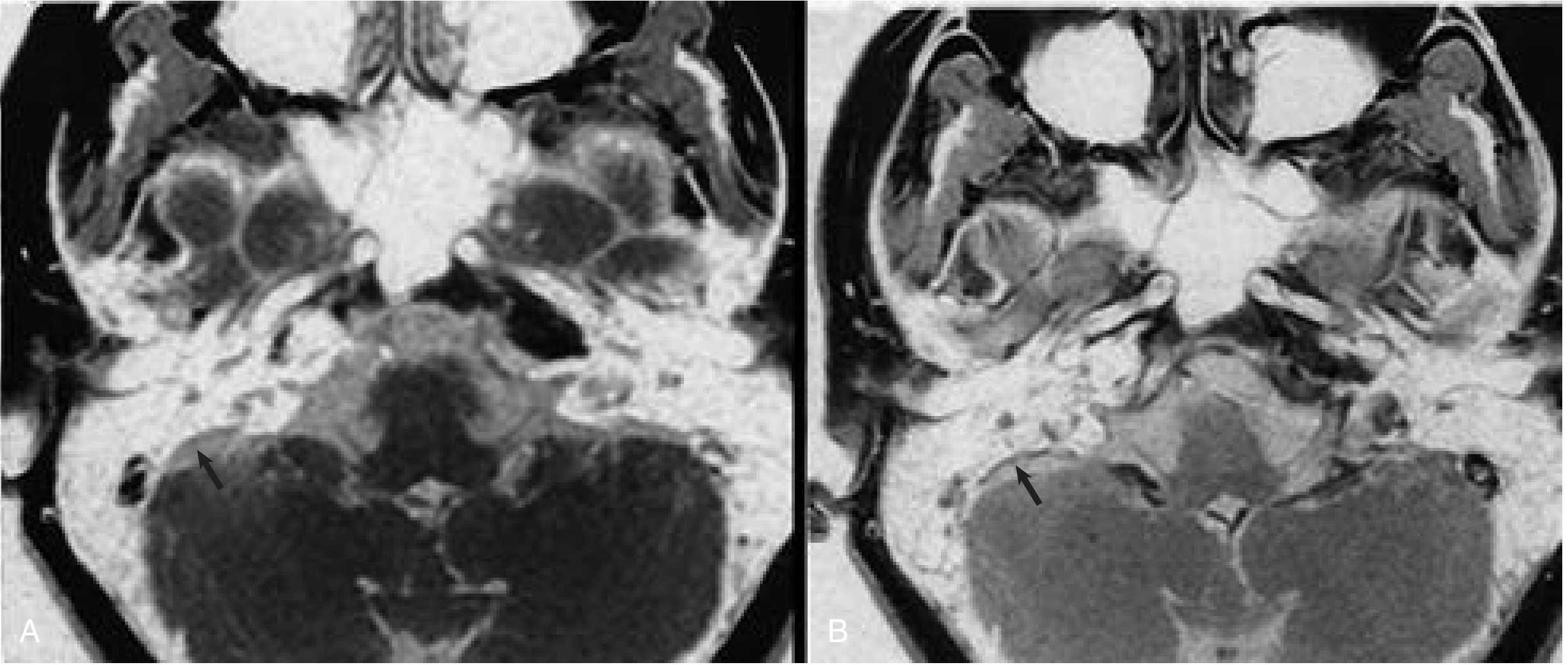
Fig: (A) Non-enhanced vs. (B) post-gadolinium MRI showing endolymphatic sac enhancement in Meniere disease. - Cummings Otolaryngology
Mechanisms of symptom generation (the Schuknecht theory):
Ruptures in the membranous labyrinth allow leakage of potassium-rich endolymph into the perilymph, which bathes the CN VIII and the lateral sides of hair cells. High extracellular potassium depolarizes and then inactivates auditory/vestibular neurons, producing the acute attack. Healing of the membrane restores the normal milieu and ends the episode. Chronic repeated exposures cause permanent hair cell injury.
Inadequate endolymph absorption by the endolymphatic sac is the other major theory. The endolymphatic duct likely acts as a valve; its disruption or hypoplasia predisposes to hydrops.
Etiology
Meniere's disease is idiopathic endolymphatic hydrops - when a known cause is identified, it is termed secondary endolymphatic hydrops. Several proposed mechanisms include:
| Factor | Details |
|---|---|
| Autoimmune | Increased specific HLA types; some patients respond to steroids and allergy desensitization |
| Viral | Possible subclinical viral injury; "delayed endolymphatic hydrops" years after viral deafness |
| Ischemic/Vascular | Sac ischemia; possible shared mechanism with migraine |
| Anatomic | Hypoplastic endolymphatic duct/sac (visible on MRI); develops by age 3 |
| Trauma/Otitis | Labyrinthitis, serous labyrinthitis, syphilis, temporal bone trauma |
Recent 2026 genome-wide analysis (PMID 42302782) implicates inner ear development pathways as a genetic basis, and a 2025 systematic review (PMID 40987969) highlighted the role of stria vascularis in pathogenesis.
Clinical Features
Classic tetrad (all four together in 50% of patients at initial presentation):
- Episodic vertigo - spinning, usually horizontal axis, lasts 20 min to 24 h (most commonly 2-3 h); associated nausea, vomiting, diaphoresis; exacerbated by head movement
- Fluctuating SNHL - low-frequency initially; audiogram shows "upsloping" pattern; progressive over time; diplacusis and loudness recruitment occur
- Tinnitus - low-pitched, roaring, louder during attacks; usually unilateral
- Aural fullness - pressure/bloating sensation in the affected ear
Prodrome: Increasing ear fullness and tinnitus often precede attacks.
Important variants:
- Otolithic crisis of Tumarkin (drop attacks): Sudden fall without loss of consciousness; occurs in 2-6% of patients; patient feels "pushed" or thrown down; due to acute utriculosaccular dysfunction; occurs late in the disease
- Lermoyez syndrome: Increasing tinnitus, hearing loss, and fullness that is relieved when a vertigo attack occurs (paradoxical)
- Delayed endolymphatic hydrops: Profound SNHL in one ear followed years later by hydrops symptoms in either the same or opposite ear
Diagnosis
No single test is diagnostic. Diagnosis is clinical, based on the AAO-HNS criteria.
AAO-HNS Diagnostic Classification (1995, still most widely used):
| Level | Criteria |
|---|---|
| Possible | Episodic vertigo without documented hearing loss, OR fluctuating/fixed SNHL with dysequilibrium but no definite episodes |
| Probable | One definitive vertigo episode + audiogram-documented hearing loss + tinnitus or aural fullness + other causes excluded |
| Definite | ≥2 spontaneous vertigo episodes lasting ≥20 min + audiometrically documented hearing loss on ≥1 occasion + tinnitus or aural fullness in the affected ear + other causes excluded |
| Certain | Definite Meniere disease + histopathologic confirmation |
Investigations:
- Audiogram: Fluctuating low-frequency SNHL; little tone decay; upsloping pattern
- Electronystagmography (ENG/VNG): Often normal between attacks; during attacks, active spontaneous nystagmus with direction-changing components
- Electrocochleography (ECochG): Increased summating potential to action potential (SP/AP) ratio >0.4 suggests endolymphatic hydrops
- Glycerol test: Oral glycerol 1.2 mL/kg - improvement in hearing and fullness within 1-2 hours (maximum at 2-3 h), then symptoms return; has diagnostic value
- MRI with gadolinium: Enhancement of endolymphatic sac; rules out vestibular schwannoma or endolymphatic sac tumor - the main indication for imaging
- High-Tesla MRI can image hydrops directly but lacks a standard protocol
Management
Acute Attack
- Vestibular suppressants: Meclizine, diazepam, lorazepam
- Antiemetics: Prochlorperazine, promethazine
- Bed rest; patient lies still to minimize symptoms
Medical (Maintenance)
| Treatment | Rationale/Evidence |
|---|---|
| Low-sodium diet (<1500-2000 mg/day) | First proposed by Furstenberg; reduces body fluid retention; low-evidence but widely used ≥50 years |
| Diuretics (hydrochlorothiazide-triamterene, acetazolamide) | Reduces endolymph volume; modest benefit in vertigo |
| Betahistine | Vasodilator; commonly used in Europe; improves microcirculation of inner ear |
| Steroids (oral or intratympanic) | IT dexamethasone for immune-mediated cases; avoids ablative surgery in up to 81-91% of patients in retrospective series |
Intratympanic Treatments
- IT Gentamicin: Chemical ablation of vestibular function; highly effective for vertigo control (75-90%); risk of hearing loss; preferred when hearing is already poor
- IT Dexamethasone: First described by Itoh and Sakta (1987); 80% vertigo relief, 74% tinnitus relief; avoids ototoxicity; optimal protocol unclear
Surgical Options (when medical therapy fails)
| Procedure | Indication | Hearing preservation? |
|---|---|---|
| Endolymphatic sac decompression/shunt | Active disease with useful hearing | Yes (but RCTs show results similar to placebo) |
| Selective vestibular nerve section (retrolabyrinthine, retrosigmoid, or middle fossa) | Disabling vertigo, useful hearing | Yes |
| Labyrinthectomy | No useful hearing remaining | No |
| Cochleosacculotomy | Elderly, disabling vertigo, poor hearing, local anesthesia | No (destroys residual hearing) |
Prognosis & Natural History
- Attacks cluster over periods separated by long remissions
- Spontaneous vertigo control occurs in ~57% at 2 years, ~71% at 8 years
- Hearing loss is subtle and reversible early, then becomes permanent and progressive, characterized by diplacusis and loudness recruitment
- Bilateral involvement develops in 20-40% of cases over a lifetime
- The condition is emotionally disabling in addition to its physical effects
Key Associations & Differential Diagnosis
- Migraine: Lifetime incidence of migraine in Meniere patients is 56% vs. 25% in controls - a strong pathophysiologic link is suspected
- Autoimmune inner ear disease (AIED): Presents as a fulminant variant of Meniere disease
- Vestibular schwannoma: Ruled out by gadolinium MRI
- BPPV: Differentiated by brief positional vertigo (<1 min) without hearing loss
- Labyrinthitis: Acute onset, single prolonged episode, hearing loss
Recent evidence note: A 2025 meta-analysis (PMID 40134376) found a significant association between Meniere's disease and thyroid disorders, suggesting thyroid screening may be warranted.
Sources: Cummings Otolaryngology Head and Neck Surgery | Bradley and Daroff's Neurology in Clinical Practice | Goldman-Cecil Medicine | KJ Lee's Essential Otolaryngology | Scott-Brown's Otorhinolaryngology Vol 2 | Textbook of Family Medicine 9e
What is the mechanism of intratympanic gentamicin and why does it cause hearing loss?
Finding Sources
Searching PubMed
"gentamicin" AND "vestibular" AND "hair cell" AND "ototoxicity"
Finding Sources
Searching PubMed
"intratympanic gentamicin" AND "Meniere"
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
I have reached my query_library_db limit. I have comprehensive information from the textbooks. Let me now compile the full, detailed answer from everything gathered.
Mechanism of Intratympanic Gentamicin & Why It Causes Hearing Loss
1. Why Gentamicin Is Used Intratympanically
Gentamicin belongs to the aminoglycoside class of antibiotics. A key pharmacological property of this class is differential organ toxicity - some aminoglycosides preferentially damage the cochlea (cochleotoxic), while others preferentially damage the vestibular apparatus (vestibulotoxic). Gentamicin and streptomycin fall firmly in the vestibulotoxic camp, which is exactly what makes gentamicin useful in Meniere's disease: it can ablate the overactive, hydrops-producing vestibular labyrinth without (in theory) destroying cochlear hearing. This is deliberately exploited as a chemical labyrinthectomy.
2. Route of Entry Into the Inner Ear
After injection into the middle ear space, gentamicin crosses the round window membrane (RWM) - a thin, three-layered structure separating the middle ear from the scala tympani of the cochlea. Drug diffuses passively through the RWM into the perilymph, from where it distributes to inner ear structures.
Key pharmacokinetic points:
- A healthy (non-inflamed) RWM is the main entry route; inflamed membranes in chronic otitis media actually paradoxically reduce permeability and dilute the drug
- Perilymph concentrations after intratympanic delivery are far higher than achievable by systemic administration, while systemic absorption is minimal - this is the rationale for the local route
- Drug also enters via the oval window to a lesser extent
3. Cellular Mechanism of Ototoxicity
Step 1 - Entry into hair cells
Gentamicin enters cochlear and vestibular hair cells via mechanosensitive cation channels (MET channels) at the tips of stereocilia - the same channels that transduce sound/head movement. It is taken up in an energy-dependent, endocytotic process. This uptake is enhanced when the channels are open (i.e., when they are being stimulated).
Step 2 - Reactive oxygen species (ROS) generation
Once inside the hair cell, gentamicin:
- Chelates iron (Fe²⁺/Fe³⁺) from cellular stores to form a gentamicin-iron complex
- This complex catalyzes the production of free radicals - particularly hydroxyl radicals (OH•) and superoxide - via Fenton-type reactions
- The ROS overwhelm the hair cell's antioxidant defenses (glutathione, catalase, superoxide dismutase)
Step 3 - Apoptotic pathway activation
ROS generation is the rate-limiting step that triggers the downstream apoptotic cascade:
- Mitochondrial membrane disruption
- Cytochrome c release
- Activation of caspases (caspase-3, caspase-9)
- Programmed hair cell death
There is also a mitochondrial genetic susceptibility: the A1555G mutation in mitochondrial 12S rRNA creates a binding site that closely resembles the bacterial rRNA target of aminoglycosides. Patients carrying this mutation have extreme aminoglycoside hypersensitivity - even a single dose can cause profound hearing loss. Screening for this mutation before IT gentamicin therapy has been proposed.
4. Why Gentamicin Is Relatively Vestibulo-Selective
This is the crux of why IT gentamicin is used therapeutically. The selectivity is anatomical and biochemical:
| Feature | Vestibular System | Cochlea |
|---|---|---|
| Predominant hair cell type | Type I (calyx-enclosed, end-bulb morphology) | Outer hair cells (OHCs) at cochlear base |
| Gentamicin sensitivity | Type I > Type II; crista ampullaris >> saccule/utricle | OHCs > IHCs; basal turn most sensitive |
| Dark cell uptake | High - dark cells of vestibular labyrinth actively take up aminoglycosides | Stria vascularis has some uptake |
| Antioxidant capacity | Lower in vestibular hair cells | Higher in cochlear hair cells (more catalase) |
| Spontaneous firing rate | High tonic firing rate - MET channels open more → more drug entry | Sound-dependent |
The vestibular Type I hair cells - particularly those in the cristae of the semicircular canals - are the primary target. They are enveloped by calyx nerve endings, have a high resting discharge rate keeping MET channels open, and have lower intrinsic antioxidant defenses compared to cochlear outer hair cells. The dark cells lining the vestibular labyrinth also actively concentrate gentamicin.
5. Why Hearing Loss Still Occurs
Despite vestibular selectivity, cochlear damage is not zero - it is a dose- and concentration-dependent phenomenon. Several mechanisms explain cochlear collateral damage:
a) Anatomical proximity
The perilymph is a shared fluid space - after crossing the RWM into the scala tympani, gentamicin freely diffuses throughout the entire perilymph. Cochlear outer hair cells at the basal turn (high-frequency region) are closest to the RWM and are therefore exposed to the highest drug concentrations first. This is why IT gentamicin-associated hearing loss is typically high-frequency in onset.
b) Dose dependency
- At low doses / infrequent injections: vestibular ablation occurs with preserved hearing
- At high doses / repeated injections: gentamicin spills over to the cochlea once vestibular hair cells are saturated and drug levels in perilymph continue to rise
- This is why the trend in clinical practice has shifted toward low-dose, titration protocols (single injections given and then waiting 4-6 weeks before re-dosing)
c) Stria vascularis damage
The stria vascularis (the ion-pumping "battery" of the cochlea that maintains endocochlear potential) also takes up aminoglycosides. Strial damage reduces the endocochlear potential (+80 mV), which impairs the electromechanical amplification by outer hair cells even before those OHCs are directly destroyed.
d) Delayed toxicity
A significant delayed effect exists - cochlear hair cell death can progress weeks to months after the last injection, as stored drug continues to generate ROS. This is why hearing loss rates quoted in trials may underestimate long-term cochlear risk.
e) Genetic susceptibility
Patients with the A1555G mitochondrial mutation can experience catastrophic bilateral deafness from even small intratympanic doses.
6. Clinical Consequences
| Parameter | Detail |
|---|---|
| Vertigo control rate | ~75-90% with titrated low-dose protocols |
| Hearing loss risk | ~15-30% with fixed high-dose schedules; <5-10% with titrated low-dose |
| Hearing loss pattern | High-frequency SNHL first; can progress to severe-profound |
| Bilateral disease risk | IT gentamicin is relatively contraindicated when the other ear also has poor hearing (risk of bilateral deafness) |
| Irreversibility | Aminoglycoside hair cell death is permanent - no regeneration occurs in mammals |
7. Protective Strategies Under Investigation
Because the final common pathway is ROS generation, antioxidants are being studied as cochlear protectants:
- Aspirin (salicylates): A placebo-controlled trial in China showed benefit in reducing aminoglycoside ototoxicity during systemic therapy - proposed mechanism is iron chelation and free radical scavenging
- D-methionine, N-acetyl cysteine, glutathione analogs: Preclinical promise
- Caspase inhibitors: Target the downstream apoptotic cascade
Summary
Intratympanic gentamicin crosses the round window membrane into perilymph, enters vestibular (and to a lesser extent cochlear) hair cells via open MET channels, chelates iron to generate hydroxyl radicals, and triggers apoptosis. Its vestibular selectivity - due to the high tonic activity and lower antioxidant defenses of vestibular Type I hair cells - makes it a useful ablative tool in Meniere's disease. Hearing loss occurs when cochlear outer hair cells (especially in the basal turn nearest the RWM) are exposed to sufficient drug concentrations, and is magnified by high doses, repeated injections, delayed ROS generation, and genetic susceptibility (A1555G mtDNA mutation).
Sources: Cummings Otolaryngology Head and Neck Surgery | Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2 | Shambaugh Surgery of the Ear | Cochrane Review - IT gentamicin for Meniere's (PMID 36847592)
NTEP
Finding Sources
Searching the Web
NTEP National Tuberculosis Elimination Programme India 2025 guidelines overview
Reading File
Reading Web Page
https://journals.lww.com/jalh/fulltext/2025/04000/a_to_z_of_…
Reading File
Reading File
Reading File
Reading File
I now have comprehensive textbook and web content. Let me compile the full answer.
NTEP - National Tuberculosis Elimination Programme
Background & Renaming
The National Tuberculosis Elimination Programme (NTEP) is the Government of India's flagship anti-tuberculosis initiative, functioning as a component of the National Health Mission (NHM). It was rechristened from the Revised National Tuberculosis Control Programme (RNTCP) on 1st January 2020, in alignment with the WHO's "End TB Strategy" targets and India's own ambitious commitment to eliminate TB by 2025 - five years ahead of the global SDG target of 2030.
The Prime Minister formally launched the "TB Mukt Bharat" (TB Free India) campaign at the Delhi End TB Summit on 13th March 2018, calling for a social movement focused on patient-centric, holistic care.
National Targets (vs. 2015 baseline, to achieve by 2025)
| Target | Goal |
|---|---|
| Reduction in TB incidence | 80% |
| Reduction in TB mortality | 90% |
| Patients with catastrophic expenditure due to TB | 0% |
National Strategic Plan 2017-2025
Driven by the "DETECT - TREAT - PREVENT - BUILD" framework:
- DETECT: Active case finding (TB Mukt Bharat campaign), community screening, institutional screening, private sector engagement
- TREAT: Universal Drug Susceptibility Testing (UDST), daily FDC regimens, shorter MDR regimens, bedaquiline rollout
- PREVENT: TB Preventive Therapy (TPT) for contacts, infection control
- BUILD: Health system strengthening, Nikshay IT platform, workforce training
Organizational Structure (5 Levels)
1. National Level
- Central TB Division (CTD) - technical arm of MoHFW; manages programme for the entire country
- Headed by Deputy Director General - TB (DDG-TB)
- Supported by 6 National Reference Laboratories (NRLs):
- National TB Institute (NTI), Bengaluru
- NIRT, Chennai
- NITRD, Delhi
- JALMA, Agra
- RMRC, Bhubaneswar
- BMHRC, Bhopal
2. State Level
- State TB Cell (STC) under state NHM
- State Tuberculosis Officer (STO) - full-time, trained at national level
- State TB Training and Demonstration Centre (STDC): 3 units - training, supervision/monitoring, Intermediate Reference Laboratory (IRL)
- State Drug Store (SDS): 1 per 5 crore population; ensures uninterrupted 1st and 2nd-line drug supply
3. District Level
- District Tuberculosis Centre (DTC) - nodal point in district
- District Tuberculosis Officer (DTO) - responsible for planning, training, supervising
4. Sub-District / Tuberculosis Unit (TU) Level
- TU is a key operational level
- Population norms:
- 1 TU per 2 lakh population (rural/urban)
- 1 TU per 1 lakh population (hilly/tribal/difficult areas)
- Staff: Medical Officer-TB Control (MO-TC), Senior Treatment Supervisor (STS), Senior TB Laboratory Supervisor (STLS) - 1 STLS per 5 lakh population
5. Peripheral Health Institution (PHI) Level
- Designated Microscopy Centre (DMC): 1 per 1 lakh population (1 per 50,000 in tribal/remote areas)
- DOT providers (ANMs, MPWs, ASHA workers, anganwadi workers, teachers, ex-patients)
Case Finding & Diagnosis
Presumptive TB - anyone presenting with symptoms suspicious of TB - is the entry point.
Diagnostic tools used under NTEP:
| Method | Details |
|---|---|
| Sputum smear microscopy | 2 samples; done at DMCs; STLS rechecks all positives + 10% of negatives |
| CBNAAT / GeneXpert (NAAT) | Real-time PCR - gold standard for rapid diagnosis; 1180+ machines deployed across all districts; detects TB + rifampicin resistance simultaneously |
| Line Probe Assay (LPA) | Conventional PCR for MTB complex + resistance detection |
| Liquid culture & DST | At IRLs for complex DR-TB cases |
| Chest X-ray | Where available; used in active case finding campaigns |
| Tuberculin Skin Test (TST) | Supportive |
Serology is BANNED - The Government of India has banned the import, manufacture, sale, distribution, and use of all TB serological tests due to poor specificity.
Universal DST (UDST): All TB patients should ideally undergo DST for RR detection (and further FQ/SLID testing if RR+) before treatment begins - ideally within 15 days of diagnosis.
Treatment
Daily Regimen (current standard - replacing the older thrice-weekly DOT regimen)
Drug-sensitive TB (DS-TB):
| Phase | Drugs | Duration |
|---|---|---|
| Intensive Phase | HRZE (Isoniazid + Rifampicin + Pyrazinamide + Ethambutol) | 2 months |
| Continuation Phase | HR (Isoniazid + Rifampicin) | 4 months |
| Total | 6 months |
Fixed Dose Combinations (FDCs) are used, including child-friendly FDCs in 6 weight bands for paediatric patients.
Drug-Resistant TB (DR-TB)
India has ~1,24,000 MDR-TB cases. NTEP structures DR-TB care at two levels:
1. DR-TB Centre:
- Manages RR-TB / MDR-TB patients on shorter regimens
- Decentralized treatment available at medical colleges
2. Nodal DR-TB Centre (NDR-TBC):
- Tertiary care institutions
- Manages XDR-TB, treatment failures, NTM, drug intolerances
- Requires ≥10 male + 10 female beds, multidisciplinary specialists, free PMDT services
Key DR-TB regimens:
- Shorter MDR regimen (rolled out from 2018)
- Bedaquiline (Bdq)-containing regimens - expanded since 2018; >7,973 patients initiated
Key Schemes & IT Platforms
Nikshay
A web-based case-based IT surveillance system (launched May 2012, enhanced 2018), meaning "Ni + Kshay" = eradication of TB. Functions include:
- TB patient registration, diagnosis, follow-up, contact tracing
- Lab reports (culture, DST, LPA, CBNAAT)
- DR-TB patient tracking
- Private health facility registration and mandatory TB notification
- 99-DOTS digital adherence monitoring (pill-pack with phone-number-coded blisters)
- SMS alerts to patients and programme officers
- Telemedicine and virtual TB care
- Aadhar-linked Direct Benefit Transfer (DBT)
- Automated periodic reports: case finding, sputum conversion, treatment outcomes
Nikshay Poshan Yojana (NPY)
- Direct nutritional support of ₹500/month to every notified TB patient throughout treatment
- Transferred directly to the patient's bank account via DBT
Nikshay Aushadhi
- Logistics and supply chain management system for anti-TB drugs and diagnostics
- Real-time stock visibility at all levels; prevents stockouts
TB Notification (Mandatory since 7th May 2012)
- Every TB case - public or private - must be notified to the District Health Officer/CMO monthly
- TB is a notifiable disease in India
Special Strategies
Active Case Finding (ACF)
- TB Mukt Bharat campaign - door-to-door screening of high-risk populations
- Targeted groups: slums, tribal areas, prisons, old age homes, orphanages, transit camps
- Tools: upfront NAAT + chest X-ray
TB Preventive Therapy (TPT)
- For household contacts of bacteriologically confirmed TB cases
- 6 months Isoniazid (6H) or 3 months Isoniazid + Rifapentine (3HP)
HIV-TB Co-management
- All TB patients offered HIV testing; HIV-positive TB patients started on ART
- 99-DOTS adherence monitoring first piloted in HIV-TB co-infected patients
Private Sector Engagement
- ~70% of patients seek care in private sector first
- NTEP mandates TB notification from private providers
- Nikshay enables private facility registration and patient linkage
- PPM (Public-Private Mix) strategy incentivizes private providers
India's TB Burden (Context)
- India accounts for ~26% of the global TB burden
- ~32% increase in drug-resistant cases is a major concern
- Despite being RNTCP's successor, NTEP represents a philosophical shift - from control to elimination, requiring not just disease management but structural health system transformation
Sources: Park's Textbook of Preventive and Social Medicine | A to Z of NTEP, JALH 2025 | Wikipedia - NTEP | Maharashtra NTEP State Portal
This is a shared conversation. Sign in to Orris to start your own chat.