Ecg
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Here is a thorough guide to ECG patterns in MI and ischemia, drawn from Harrison's 22E, Tintinalli's Emergency Medicine, and Goldman-Cecil Medicine.
ECG in Myocardial Infarction and Ischemia
The Physiology Behind the Findings
Ischemia lowers the resting membrane potential and shortens action potential duration, creating a current of injury between normal and ischemic zones. This is what shifts the ST segment on the surface ECG.

- Subendocardial ischemia - ST vector shifts toward the inner cavity → leads overlying the area show ST depression (with reciprocal ST elevation in aVR)
- Transmural (epicardial) injury - ST vector shifts outward → overlying leads show ST elevation
STEMI vs NSTEMI - Key Distinction
| Feature | STEMI | NSTEMI |
|---|---|---|
| ST changes | ST elevation meeting criteria | ST depression / T-wave changes / no changes |
| Troponin | Elevated | Elevated |
| Reperfusion urgency | Immediate (cath lab activation) | Guided by risk stratification |
| Mechanism | Complete occlusion (usually) | Partial occlusion / demand ischemia |
The distinction matters because emergency reperfusion (primary PCI or thrombolysis) is consistently effective for STEMI, while the indication in NSTEMI depends on ongoing risk assessment. - Harrison's 22E
STEMI: Diagnostic ECG Criteria by Location
(From Tintinalli's Emergency Medicine)
| Territory | Leads with ST Elevation | Artery |
|---|---|---|
| Anteroseptal | V1, V2 (± V3) | Proximal LAD |
| Anterior | V1 - V4 | LAD |
| Anterolateral | V1 - V6, I, aVL | Proximal LAD |
| Lateral | I, aVL | Diagonal / LCx |
| Inferior | II, III, aVF | RCA (80%) or LCx (20%) |
| Inferolateral | II, III, aVF + V5, V6 | LCx |
| True posterior | Tall R in V1-V2 (R/S ≥ 1, R > 0.04 s); ST elevation on posterior leads V7-V9 | LCx or RCA |
| Right ventricular | II, III, aVF + ST elevation in right-sided leads (V3R-V6R) | Proximal RCA |
Standard numeric thresholds:
- ≥ 1 mm ST elevation in 2 contiguous limb leads
- ≥ 2 mm in 2 contiguous precordial leads (≥ 2.5 mm in men < 40 yrs; ≥ 1.5 mm in women in V2-V3)
Localizing the Culprit Artery
Inferior STEMI:
- ST elevation in III > II, with ST depression >1 mm in I and aVL → RCA
- Above findings + ST elevation in V1 or V4R → Proximal RCA (with RV involvement)
- ST elevation in I, aVL, V5-V6 with isoelectric/elevated ST in I → Left Circumflex (LCx)
- ST elevation aVR > V1 → Left main or proximal LAD
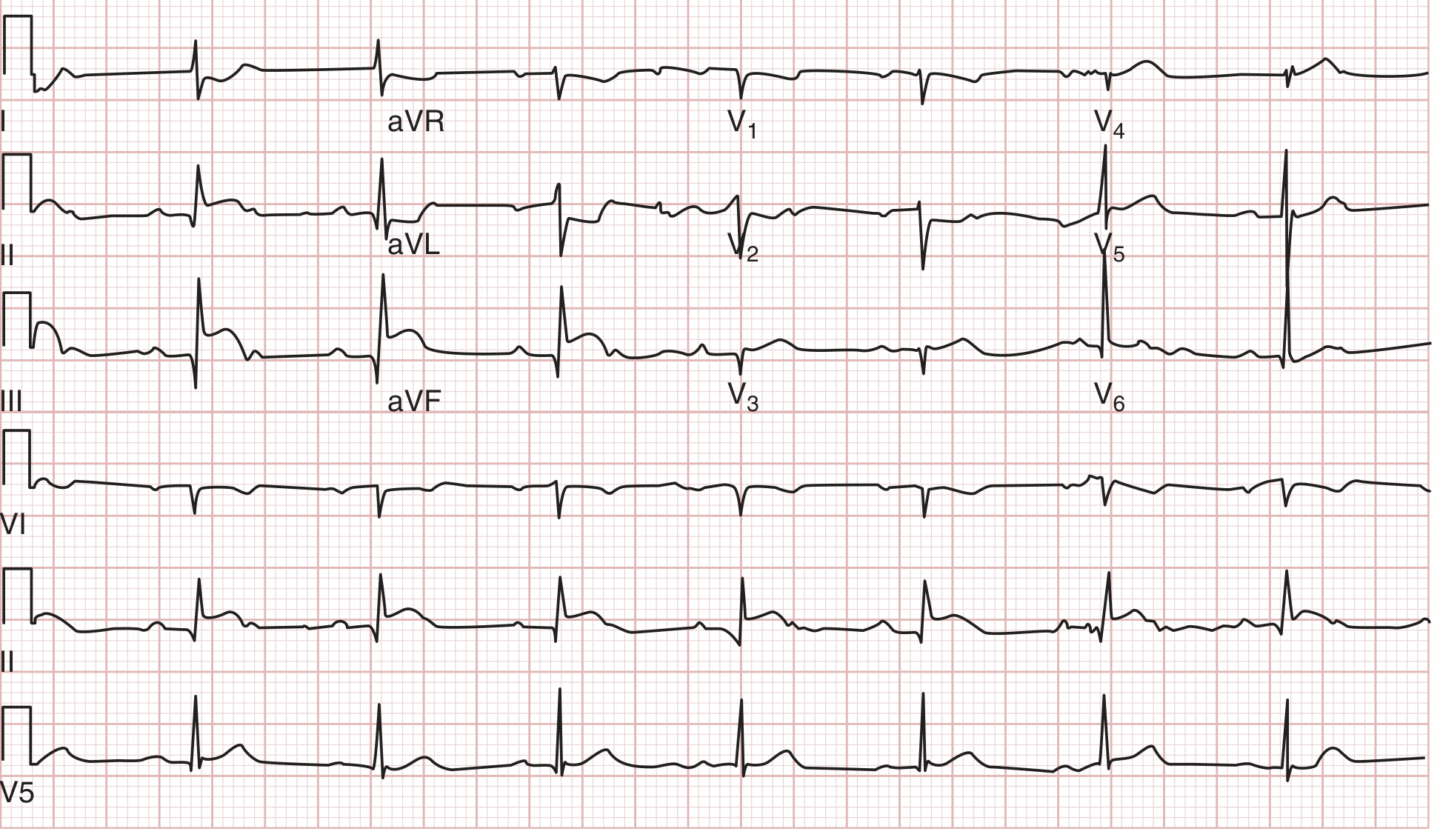
Right Ventricular Infarction:
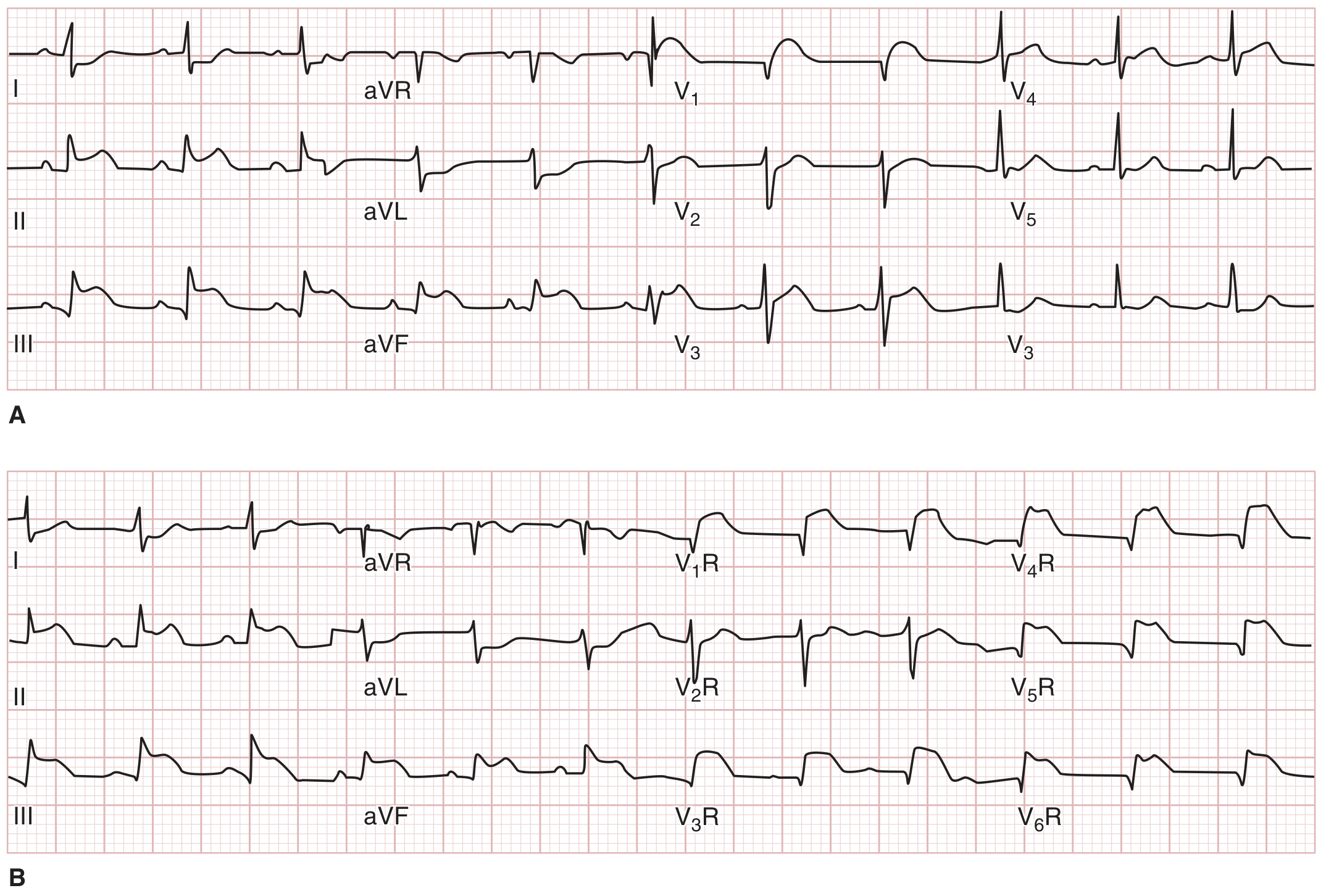
Always obtain right-sided leads (V3R-V6R) in inferior STEMI to detect RV involvement. RV infarction has higher morbidity than isolated inferior infarction.
Temporal Evolution of STEMI
| Phase | ECG Findings |
|---|---|
| Earliest (minutes) | Hyperacute T waves - tall, peaked, broad |
| Early (hours) | ST elevation - upward-sloping ("tombstone"), ± loss of R wave |
| Established | Q waves develop (necrosis), ST begins to settle |
| Days to weeks | T-wave inversions in affected leads |
| Chronic | Q waves persist; T waves may normalize over months |
After Q-wave infarction, persistent ST elevation weeks later correlates with a severe wall motion disorder (possible ventricular aneurysm), not acute re-injury.
Q Waves
- A Q wave is abnormal if it is > 40 ms wide or > 25% of the R-wave amplitude in the same lead
- Q waves indicate myocardial necrosis sufficient to lose depolarization forces
- Old teaching: Q waves = transmural MI; no Q waves = subendocardial. This is no longer reliable - transmural infarcts can occur without Q waves, and subendocardial infarcts can produce Q waves
- Classify instead as Q-wave MI vs non-Q-wave MI
Reciprocal Changes
Reciprocal ST depression (in leads opposite the infarct zone) indicates:
- Larger area of injury at risk
- More severe underlying CAD
- Higher likelihood of pump failure and cardiovascular complications
- Increased mortality
In general, more ST segments elevated = more extensive injury.
Ischemia Patterns Without Complete Occlusion (NSTEMI / Unstable Angina)
Wellens' Syndrome (critical LAD stenosis)

Deep, symmetric T-wave inversions in V1-V4 (and sometimes I, aVL) indicate critical proximal LAD stenosis (Wellens' sign). ~75% have deeply inverted T waves; ~25% have biphasic T waves in the same leads. The T-wave changes appear when the patient is pain-free and may normalize when pain recurs - serial ECGs and pain correlation are key. This is a high-risk pattern requiring urgent catheterization.
Important ECG Limitations
- A single normal ECG does not exclude MI - a normal tracing throughout the entire course is uncommon but does occur
- LBBB, ventricular pacemaker rhythms, and WPW can all mask ischemic changes
- New (or presumed new) LBBB in the setting of chest pain - Sgarbossa criteria help identify superimposed STEMI:
- Concordant ST elevation ≥ 1 mm in any lead (concordant with QRS direction)
- Concordant ST depression ≥ 1 mm in V1-V3
- Excessive discordant ST elevation ≥ 5 mm (less specific)
- Note: <10% of patients with new LBBB actually have AMI
Summary: Quick Reference
| Finding | Interpretation |
|---|---|
| ST elevation in contiguous leads | STEMI - transmural injury |
| ST depression | Subendocardial ischemia / NSTEMI |
| Hyperacute T waves | Earliest STEMI - pre-elevation phase |
| Deep T inversions V1-V4 | Wellens' - critical LAD stenosis |
| Tall R in V1-V2 + ST depression V1-V3 | Posterior MI (mirror image) |
| ST elevation V3R-V6R | RV infarction |
| New Q waves | Established necrosis |
| Persistent ST elevation weeks post-MI | Wall motion disorder / ventricular aneurysm |
Sources: Harrison's Principles of Internal Medicine 22E (2025), Tintinalli's Emergency Medicine, Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.