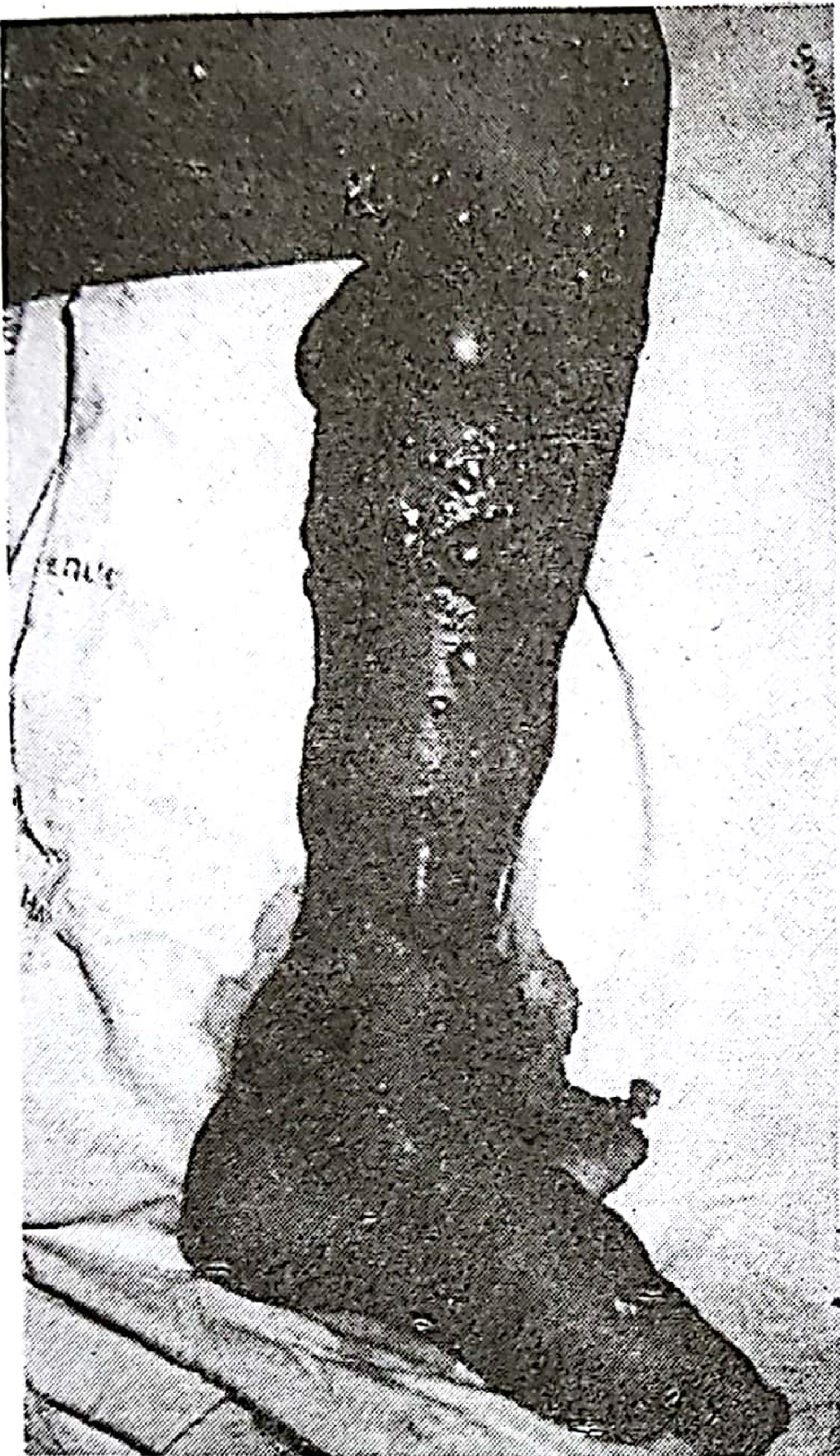
Post snake bite
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Here is the complete, well-structured answer:
Post Snake Bite - Clinical Management
Epidemiology
Approximately 5 million snake bites occur globally each year, resulting in up to 2.4 million envenomings, 94,000-125,000 deaths, and around 400,000 amputations or permanent disabilities. Most occur in Africa, Asia, and Latin America. Incidence peaks during planting/harvesting seasons and in agricultural workers. About 70% of bites are from non-venomous snakes, and only 50% of bites by venomous species actually envenomate the patient. - Park's Textbook of Preventive and Social Medicine, p.465; Pye's Surgical Handicraft, p.427
Types of Venom
| Venom Type | Snakes | Primary Effect |
|---|---|---|
| Neurotoxic | Cobras, kraits, coral snakes, elapids | Flaccid paralysis via d-tubocurarine-like NMJ blockade; respiratory/cardiac failure |
| Vasculotoxic / Hemotoxic | Vipers (Russell's viper, saw-scaled/carpet viper) | Intravascular hemolysis, coagulation defects, hemorrhage |
| Myotoxic | Sea snakes, some Australasian elapids | Rhabdomyolysis, myoglobinuria, renal failure |
| Mixed | Rattlesnakes, copperheads | Cytotoxic + hemorrhagic + neurotoxic |
- The Essentials of Forensic Medicine and Toxicology, 36th ed., p.564
Clinical Features
Colubrine (Neurotoxic - Cobra/Krait) vs. Viperine Bite - Key Differences
| Feature | Colubrine (Elapid) | Viperine |
|---|---|---|
| Bite area | Reddish wheal, slight burning pain | Marked pain and bloody oozing |
| Swelling | Minimal or absent | Spreads to entire limb and trunk |
| Symptoms onset | After 30+ minutes | Immediate to 15 minutes |
| Paralysis | Lower limbs → trunk → head (ascending) | Absent |
| Hemorrhage | Absent | Prominent |
| BP | Normal | Hypotension |
| Clotting time | Normal | Prolonged |
| Cause of death | Respiratory failure | Circulatory failure (hemolysis/hemorrhage) |
- Forensic Medicine and Toxicology, 36th ed., p.565
Local Envenomation (Viperidae)
- Massive swelling progressing over days, involving the entire bitten limb and adjacent trunk
- Linear erythema/bruising along superficial lymphatics
- Blisters (serous or serosanguinous) at bite site, extending proximally with severe envenomation
Neurotoxic Envenomation Sequence (Cobra)
- Local symptoms within 6-8 minutes (small reddish-bluish wheal, tender, burning pain)
- Systemic symptoms at ~30 minutes: sleepiness, leg weakness, nausea/vomiting
- Ptosis - earliest neuroparalytic sign
- Ophthalmoplegia, diplopia, dysarthria, dysphagia
- Ascending flaccid paralysis: limbs → trunk → facial muscles, palate, tongue, neck
- Excessive salivation, headache, perioral paraesthesias
- Respiratory arrest (obstruction by paralyzed tongue/vomitus, or intercostal/diaphragmatic paralysis)
- Key test: inability to raise head in supine position = imminent respiratory failure
Rhabdomyolysis (Sea snakes, some elapids)
- Generalized muscle aches, stiffness, trismus within 0.5-3.5 hours
- Urine becomes "mahogany" / "Coca-Cola" coloured (myoglobinuria) by 3-8 hours
- Can progress to acute renal failure, hyperkalemia, cardiac arrest
Early Clues to Severe Envenomation
- Snake identified as very dangerous
- Rapid early extension of local swelling from bite site
- Tender enlargement of local lymph nodes (lymphatic spread)
- Early systemic collapse (hypotension, shock, nausea, vomiting, heavy eyelids, drowsiness, ptosis/ophthalmoplegia)
- Early spontaneous systemic bleeding
- Passage of dark brown/black urine (myoglobinuria/hemoglobinuria)
Diagnosis
- 20-Minute Whole Blood Clotting Test (20WBCT): A few mL of fresh venous blood placed in a clean dry glass tube. If blood remains liquid after 20 minutes = non-clotting = viper bite/coagulopathy. Repeat every 6 hours to guide antivenom dosing.
- Snake venom antigen detection: From wound swabs, aspirates, serum, CSF, or urine. By radioimmunoassay (RIA, detects 0.4 μg/L) or enzyme immunoassay (EIA).
- Urinalysis: Myoglobinuria (positive 'stix' for blood/hemoglobin), proteinuria, dark urine.
- Monitoring: Level of consciousness, ptosis, pulse rate, BP, respiratory rate, progression of local swelling, urine output.
Management
First Aid (Pre-Hospital)
DO:
- Reassure the patient (panic accelerates venom absorption)
- Immobilize the bitten limb with a splint/sling - treat like a fractured limb; firm bandaging prevents muscular contraction and lymphatic spread
- Remove constricting items (rings, bracelets, watches, footwear)
- Transport to hospital as quickly, comfortably, and passively as possible
- Bring the snake if safely killed/secured (for identification)
DO NOT:
- Apply tight tourniquets (don't work; can be dangerous)
- Incise, excise, or cauterize the wound
- Apply ice packs
- Give alcohol or stimulants (vasodilators - speed venom absorption)
- Apply suction or electric shock devices
- Give aspirin or NSAIDs (bleeding risk)
At Primary Health Centre
- Assess for local and systemic envenomation (hourly monitoring)
- 20WBCT + urinalysis + snake identification
- Analgesia: Paracetamol (adults 500 mg-1 g; children 10-15 mg/kg) or codeine phosphate (adults 30-60 mg) every 4-6 hours - NOT aspirin/NSAIDs
- Antivenom if indicated and skills/equipment available
- IV fluid challenge (250-500 mL 0.9% saline) for shock/hypotension
- Oxygen + consider atropine and neostigmine for respiratory paralysis; transfer to hospital
Antivenom (Anti-Snake Venom - ASV / Polyvalent Antivenom - PAV)
The only specific treatment for envenomation. It is hyperimmune animal (usually horse) serum.
Indications for Antivenom
Systemic envenomation:
- Hypotension, shock, other cardiovascular toxicity
- Neurotoxicity (ptosis, ophthalmoplegia, paralysis)
- Rhabdomyolysis
- Impaired consciousness
- Spontaneous systemic bleeding
- Non-clotting blood (positive 20WBCT)
- Leukocytosis (WBC >20,000/μL), elevated serum enzymes
- Acidosis
Local envenomation:
- Swelling involving >half of bitten limb
- Rapid progression of swelling (e.g., crossing a joint within 1-2 hours)
- Known necrotic venom species
- Bites on digits or tight fascial compartments
Dosing (PAV/ASV)
| Severity | Dose |
|---|---|
| Minimal (local swelling, no systemic signs) | 5 vials |
| Moderate (swelling beyond bite site + systemic signs) | 10 vials |
| Severe (marked local + severe systemic) | 10-15 vials |
- Lyophilized powder diluted in 500 mL distilled water/normal saline, infused over 1 hour
- Children require the same dose as adults
- In neurotoxic envenomation: repeat 10 vials after 1 hour if no response
- In hemotoxic envenomation: repeat initial dose every 6 hours until 20WBCT normalizes (liver needs 6 hours to restore clotting factors); then check every 12 hours for at least 48 hours for recurrence
- Most useful within 4 hours of bite; less effective at 8 hours; doubtful value after 24 hours
- Skin/conjunctival sensitivity tests should NOT be given (poor predictors of anaphylaxis; may presensitize)
Antivenom Reactions
- Early (anaphylactic): Itching, urticaria, tachycardia, fever, cough, vomiting within 10 min-2 hours
- At first sign of reaction (urticaria, shivering, hypotension, bronchospasm): stop infusion immediately, give IM adrenaline (epinephrine)
- Late (serum sickness): Occurs 5-10 days later; treat with antihistamines and corticosteroids
Treatment of Specific Complications
| Complication | Treatment |
|---|---|
| Respiratory paralysis | O₂, mechanical ventilation; neostigmine + atropine (for postsynaptic NMJ block) |
| Hypotension/shock | Antivenom + IV fluids (fresh blood or fresh frozen plasma); refractory: dopamine 2.5-5 μg/kg/min via central vein |
| Renal failure | Cautious rehydration + diuretics + dopamine; peritoneal dialysis or hemodialysis if conservative treatment fails |
| Necrosis | Surgical debridement at earliest signs; split-skin grafting; prophylactic antimicrobials (penicillin or erythromycin); tetanus toxoid booster |
| Coagulopathy | Antivenom (primary); FFP if needed; avoid heparin |
| Local blisters/bullae | Leave intact unless large and threatening to rupture - then aspirate with fine needle; avoid occlusive dressings |
Fatal Doses and Periods (Forensic Reference)
| Snake | Fatal Dose (dry venom) | Fatal Period |
|---|---|---|
| Cobra (Naja naja) | 12 mg | 0.5 - 6 hours |
| Russell's viper | 15 mg | 1-2 days |
| Krait (Bungarus caeruleus) | 6 mg | - |
| Echis (saw-scaled viper) | 8 mg | - |
- Forensic Medicine and Toxicology, 36th ed., p.565-566
Key Points to Remember
- "Dry bite": No venom injected - occurs in 1/3 to 1/2 of bites by venomous snakes; may be due to washing of area, bite through thick clothing, superficial bite in mobile body part
- Fright reactions (tachycardia, cold clammy skin, hypotension) from a non-venomous bite can mimic envenomation - distinguish carefully
- The most common early neuroparalytic sign is ptosis
- Neostigmine test: If ptosis reverses after neostigmine, it confirms postsynaptic NMJ blockade (elapid venom) and guides ongoing treatment
- Severely envenomed patients must be observed in hospital for several days due to late recurrence from continued venom absorption
Sources: Pye's 22nd Edition Surgical Handicraft, Park's Textbook of Preventive and Social Medicine, The Essentials of Forensic Medicine and Toxicology 36th ed. (2026)
This is a shared conversation. Sign in to Orris to start your own chat.