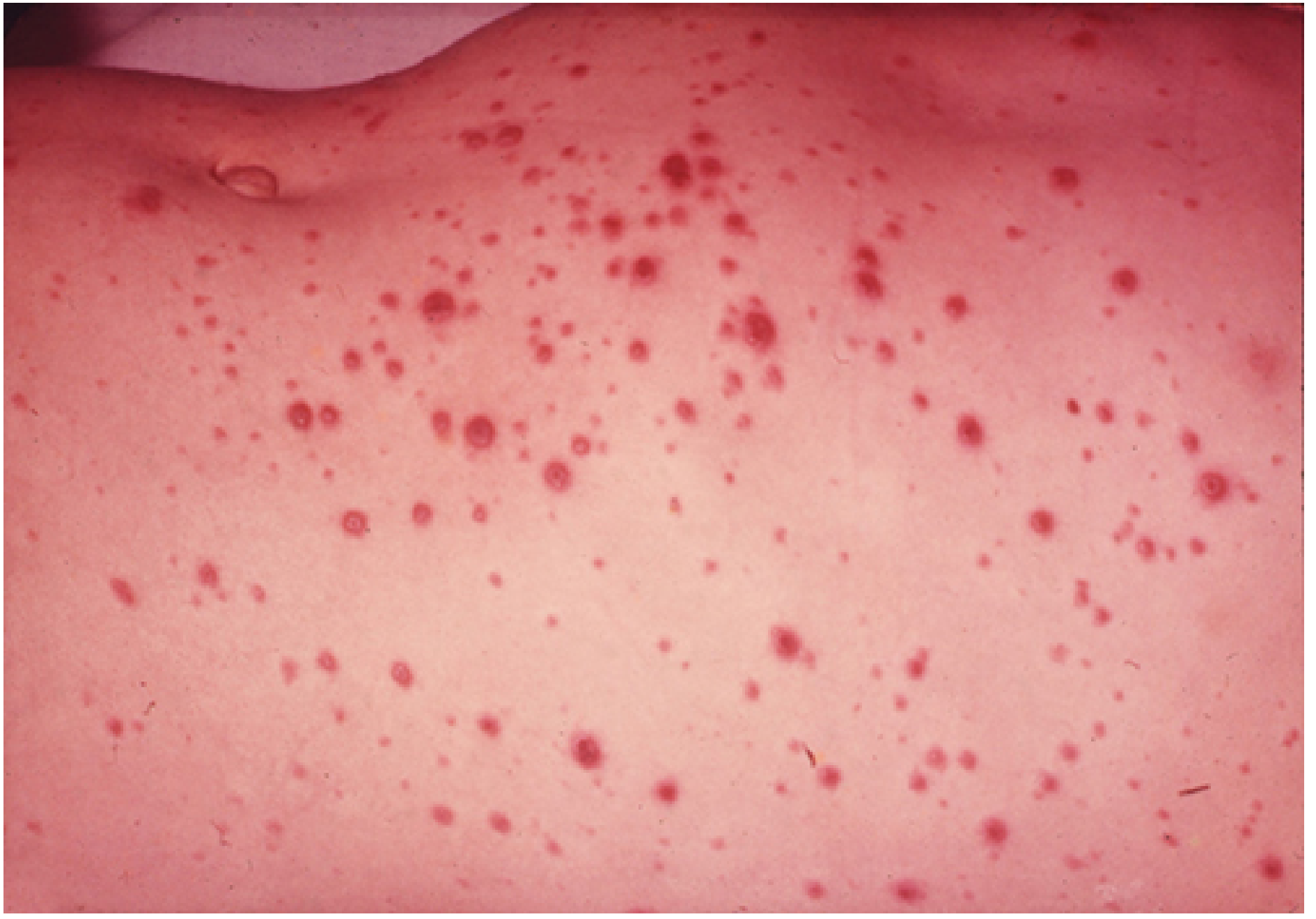
Chicken pox in 8 years old
Reading File
Finding Sources
Searching PubMed
"varicella" AND "children"
Searching the Web
chickenpox varicella 8 year old child treatment management guidelines 2024
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Here is the full clinical summary:
Chickenpox (Varicella) in an 8-Year-Old Child
Causative Agent
Varicella-Zoster Virus (VZV), also known as human herpesvirus 3 (HHV-3), a member of the family Herpesviridae, subfamily Alphaherpesvirinae.
Epidemiology
- Humans are the only source; highly contagious via direct contact with lesions or airborne spread
- Incubation period: 10-21 days (usually 14-16 days); extended up to 28 days after VZIG
- Contagious from 1-2 days before rash onset until all lesions have crusted/dried
- An 8-year-old falls in the classic age group; household secondary cases tend to have more lesions than the index case
- Immunity after wild-type infection is generally lifelong
Clinical Presentation
Prodrome (1-2 days):
- Low-grade fever, malaise, headache, anorexia
Rash (characteristic - the hallmark):
- Starts on the back of the head/ears, then spreads centrifugally to face, trunk, proximal extremities
- Mucous membrane involvement is common
- 250-500 lesions in an unvaccinated child, varying in number from 10 to several hundred
- Key feature: lesions appear in successive crops - simultaneously showing macules, papules, vesicles, pustules, and crusts at different stages
Progression of individual lesions:
- Erythematous macule/papule
- Fluid-filled vesicle ("dewdrop on a rose petal")
- Vesicle becomes turbid/cloudy in 1-2 days
- Crust forms
Diagnosis
- Primarily clinical - the characteristic rash at multiple stages is usually diagnostic
- Lab confirmation (if needed - atypical/severe cases):
- PCR - most sensitive; from vesicular swabs, scrapings, or CSF
- Direct Fluorescent Antibody (DFA) - rapid antigen detection from lesion scraping
- Multinucleated giant cells on Tzanck smear (not VZV-specific)
Complications in Children
In an immunocompetent 8-year-old, most cases are mild, but complications can occur:
| Complication | Notes |
|---|---|
| Bacterial superinfection | Most common in children - group A Streptococcus or Staphylococcus from scratched lesions |
| Acute cerebellar ataxia | Most common neurologic complication in immunocompetent children |
| Encephalitis | Less common; serious |
| Thrombocytopenia | Can be hemorrhagic |
| Reye syndrome | Risk with aspirin use - aspirin is absolutely contraindicated |
| Pneumonia | More common in adults; uncommon in immunocompetent children |
| Hepatitis, arthritis, glomerulonephritis | Rare |
| Progressive varicella | In immunocompromised patients - visceral dissemination, 20% mortality |
Mortality in children aged 1-14 years: less than 1 in 100,000 (Red Book 2021).
High-risk groups for severe disease in pediatric patients:
- Immunocompromised (T-cell defects, HIV, malignancy)
- High-dose systemic corticosteroids (>2 mg/kg/day prednisone)
- Chronic skin or pulmonary disorders
- Long-term salicylate therapy
- Infants and adolescents
Treatment
For a healthy 8-year-old (immunocompetent)
Antiviral therapy is NOT routinely recommended for healthy children under 12 years.
Supportive care (mainstay):
- Daily bathing and meticulous skin care; keep fingernails short to reduce scratching
- Tepid water baths and wet compresses for pruritus (better than drying lotions)
- Oral antihistamines (e.g., diphenhydramine) for itch
- Acetaminophen/paracetamol for fever - NOT aspirin or salicylates (Reye syndrome risk)
- NSAIDs (ibuprofen) - use cautiously; some guidelines advise against ibuprofen due to risk of invasive Group A Streptococcal infection
Antiviral considerations:
- Acyclovir may be considered in children <12 years if started within 24 hours of rash onset (20 mg/kg orally every 6 hours, max 800 mg/dose, for 5 days), but benefit is modest
- Routine use is not AAP-recommended for otherwise healthy children under 12
- The AAP recommends acyclovir for children >12 years, those with chronic skin/pulmonary disorders, on long-term salicylates, or on corticosteroids
Bacterial superinfection:
- Treat with a first-generation cephalosporin if present
For immunocompromised children or severe disease
- IV acyclovir: 10 mg/kg every 8 hours for 7 days
- Reduces visceral dissemination; indicated for immunocompromised, varicella pneumonia, or encephalitis
Isolation and Infection Control
- Isolate the child from school/daycare until all lesions are crusted (typically 5-7 days after rash onset)
- In healthcare settings, strict airborne + contact precautions are required
- Particularly important if immunocompromised contacts are present
Prevention
| Vaccine | Schedule |
|---|---|
| Varivax (single-antigen, live attenuated Oka strain) | 2 doses: 12-15 months + 4-6 years |
| ProQuad / MMRV | Combination measles-mumps-rubella-varicella |
- 2-dose schedule is 98% effective against varicella; 100% effective against severe disease
- If unvaccinated and exposed, post-exposure vaccination within 3-5 days can prevent or attenuate illness
- Varicella-Zoster Immune Globulin (VZIG) within 10 days for high-risk susceptible contacts (immunocompromised, neonates, pregnant seronegative women)
Summary Table for an 8-Year-Old
| Feature | Detail |
|---|---|
| Typical presentation | Pruritic vesicular rash in crops, low-grade fever |
| Contagious period | 1-2 days before rash to all lesions crusted |
| Fever management | Acetaminophen only - NO aspirin |
| Antivirals | Not routine; consider if high-risk features |
| School return | When all lesions crusted |
| Most feared complication | Secondary bacterial infection; cerebellar ataxia |
| Red flags | High fever persisting >5 days, difficulty breathing, neurologic signs, hemorrhagic lesions, severe abdominal pain |
Sources: Red Book 2021 (AAP Committee on Infectious Diseases), Harrison's Principles of Internal Medicine 22E, Tintinalli's Emergency Medicine, Sherris & Ryan's Medical Microbiology 8E, Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.