de quervains tenosynovitis treatment
Reading File
Finding Sources
Searching PubMed
de quervain tenosynovitis treatment
Reading File
Reading File
Reading Article
PMID: 38613563
Reading Article
PMID: 38642740
Loading Image
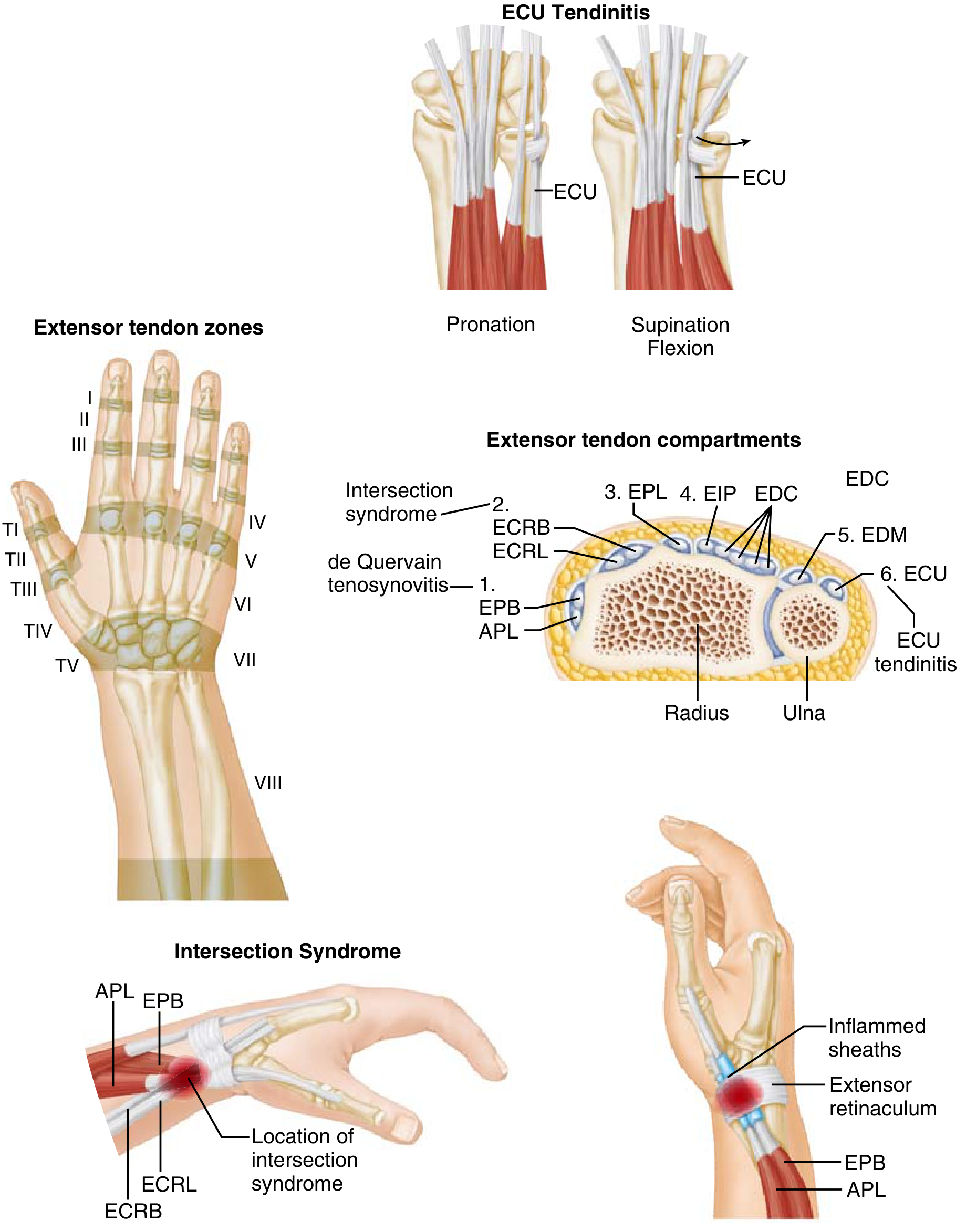
De Quervain Tenosynovitis — Treatment
Pathology recap: An attritional/degenerative condition affecting the first dorsal extensor compartment — specifically the abductor pollicis longus (APL) and extensor pollicis brevis (EPB). Inflammation and narrowing of the tendon sheath cause dorsoradial wrist pain, swelling, and crepitus. Confirmed by the Finkelstein test (thumb folded across palm → passive ulnar deviation reproduces pain).
1. Non-Operative Treatment (First-Line)
| Modality | Details |
|---|---|
| Activity modification / rest | Avoid repetitive thumb pinching/gripping and ulnar deviation |
| Thumb spica splint | Immobilises the first compartment; alone is less effective than injection but useful as adjunct |
| NSAIDs | Oral or topical; symptomatic relief |
| Corticosteroid injection | Gold standard — injection into the first dorsal extensor compartment; success in >80% of patients |
Corticosteroid injection specifics (Goldman-Cecil Medicine):
- Agent: methylprednisolone acetate 40 mg/mL, 0.5 mL
- Injected into the tendon sheath (not intratendinous)
- Risks: skin hypopigmentation, subcutaneous fat atrophy, tendon rupture (with multiple intratendinous injections)
Best practice per 2024 meta-analysis (PMID 38642740, n=1206): Corticosteroid injection alone is superior to immobilisation alone (RR 1.61; 95% CI 1.21–2.15). Combining injection + immobilisation is even more effective than either alone (RR 2.15 vs. immobilisation; RR 1.23 vs. injection alone) — combine both for first-line management.
2. Second-Line / Adjunct Options
Per a 2024 network meta-analysis (PMID 38613563, 14 RCTs):
- Extracorporeal shockwave therapy (ESWT): ranked highest for short- and medium-term VAS pain reduction; statistically superior to placebo — consider when injections fail or are contraindicated
- Laser therapy + orthosis: showed favourable short-term outcomes
- Platelet-rich plasma (PRP): demonstrated sustained benefit at 1 year; useful for patients who decline steroids or have recurrence
- Acupuncture: did not significantly differ from placebo in this analysis; cautious use
⚠️ Isolated injection with PRP or acupuncture alone should be used with caution — no significant benefit over placebo in short-to-medium term.
3. Surgical Treatment
Indication: Failure of non-operative treatment
Procedure: Release (longitudinal incision) of the first extensor compartment retinaculum
- The dorsal retinaculum is preserved/repaired to prevent volar tendon subluxation
- Anatomic variations are frequently found in recalcitrant/failed cases — e.g., multiple APL slips, EPB in its own separate sub-compartment (must be released separately)
- Outcomes are generally excellent
Surgical complications:
- Iatrogenic injury to the superficial branch of the radial nerve (SBRN) — most common
- Tendon subluxation
- Complex regional pain syndrome (CRPS)
- Recurrence from incomplete release
Summary Algorithm
Diagnosis confirmed (Finkelstein +)
↓
Corticosteroid injection (methylprednisolone) + thumb spica splint
↓ (failure after 1–2 injections, ~3–6 months)
ESWT or PRP (if steroid contraindicated/declined)
↓ (persistent symptoms)
Surgical first compartment release
Sources: Miller's Review of Orthopaedics, p. 672; Goldman-Cecil Medicine; Chong et al., J Hand Surg Am 2024 [PMID 38613563]; Cevik et al., Hand Surg Rehabil 2024 [PMID 38642740]
This is a shared conversation. Sign in to Orris to start your own chat.