Treatment of asthma
Reading File
Finding Sources
Searching PubMed
"asthma" AND "treatment"
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, well-sourced content from multiple authoritative textbooks. Here is a thorough synthesis:
Treatment of Asthma
Overview
Asthma management is built on two pillars: relievers (bronchodilators for acute symptoms) and controllers (anti-inflammatory agents for long-term control). Treatment is adjusted in a stepwise fashion guided by GINA (Global Initiative for Asthma) and NHLBI-EPR guidelines, with the goal of minimising daily symptoms and exacerbation risk while using the least medication necessary. — Murray & Nadel's Textbook of Respiratory Medicine
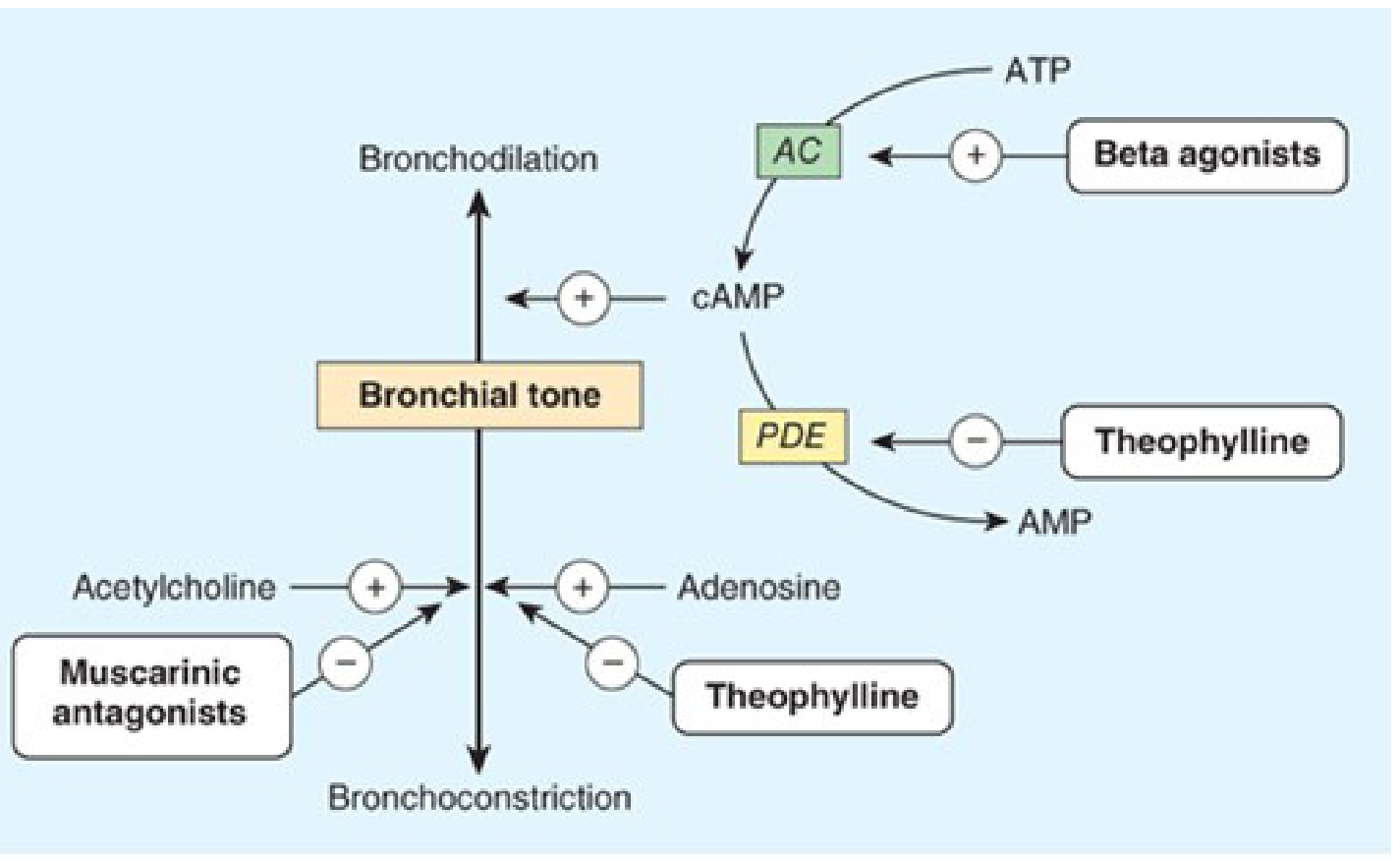
Pharmacological Mechanism Overview
Drug Classes
1. β₂-Adrenoceptor Agonists (Bronchodilators)
The cornerstone of asthma therapy. They bind β₂ receptors on airway smooth muscle → activate adenylyl cyclase → ↑ cAMP → smooth muscle relaxation. They also reduce mast cell mediator release and vascular permeability. — Katzung's Basic and Clinical Pharmacology, 16th Ed.
Short-Acting β₂ Agonists (SABAs) — Rescue therapy
- Albuterol (salbutamol) — most widely used; onset within 15 min, duration 3–4 h
- Delivered by MDI (100–400 mcg) or nebuliser (2.5–5 mg)
- Used for symptom relief and before exercise
- Overuse (>2 doses/week) signals inadequate control → step-up needed
Long-Acting β₂ Agonists (LABAs) — Add-on controller (never monotherapy)
- Salmeterol, formoterol, indacaterol — duration 12–24 h
- Always combined with an ICS; salmeterol monotherapy was associated with increased asthma-related death
- Formoterol has a faster onset and can be used as both controller and reliever (MART strategy)
Adverse effects: tachycardia, tremor, hypokalaemia (dose-related, mostly with systemic/high-dose inhaled use)
2. Inhaled Corticosteroids (ICS) — Primary Controllers
The most effective anti-inflammatory agents for persistent asthma. They reduce airway hyperresponsiveness, decrease exacerbation frequency, and are the first-line controller at all GINA steps 2–5.
| Drug | Common doses |
|---|---|
| Budesonide | 200–800 mcg/day |
| Fluticasone propionate | 100–500 mcg/day |
| Beclomethasone | 100–400 mcg/day |
| Mometasone | 200–400 mcg/day |
Adverse effects: oral candidiasis, dysphonia (local); with high doses — adrenal suppression, reduced bone density (systemic)
Always use a spacer and rinse mouth after use to reduce oropharyngeal deposition.
3. ICS + LABA Combinations
Adding a LABA to an ICS improves symptom control and reduces exacerbations more than doubling the ICS dose. Examples:
- Budesonide/formoterol (can be used as MART — Maintenance And Reliever Therapy)
- Fluticasone/salmeterol
- Fluticasone furoate/vilanterol (once daily)
4. Muscarinic Antagonists (Anticholinergics)
Block M3 receptors on airway smooth muscle → reduce cholinergic bronchoconstriction.
Short-acting (SAMA): Ipratropium bromide
- Onset ~15–30 min, duration ~4–6 h
- Particularly useful in acute severe asthma in the ED (combined with SABA)
- Dose in acute exacerbation: 0.5 mg nebulised every 20 min × 3, then as needed
Long-acting (LAMA): Tiotropium
- Add-on therapy at GINA step 4–5 for adults with poorly controlled asthma
- Reduces exacerbation risk as an adjunct to ICS ± LABA
5. Methylxanthines (Theophylline)
Mechanism: Inhibits phosphodiesterase (PDE) → ↑ cAMP; also antagonises adenosine receptors. Moderate bronchodilator with mild anti-inflammatory effects.
- Narrow therapeutic index: serum levels must be monitored (target 5–15 mcg/mL)
- Use has declined due to availability of safer, more effective agents
- Still used as add-on in severe asthma in resource-limited settings
Adverse effects (dose-related): nausea, vomiting, insomnia, seizures, arrhythmias
6. Leukotriene Receptor Antagonists (LTRAs)
- Montelukast, zafirlukast — block cysteinyl leukotriene (CysLT₁) receptors
- Oral agents; useful for mild persistent asthma, aspirin-sensitive asthma, and exercise-induced bronchoconstriction
- Less effective than ICS as monotherapy; can be used as ICS add-on
- Note: Montelukast carries an FDA black-box warning for neuropsychiatric effects (depression, suicidal ideation)
7. Biologic/Targeted Therapies (GINA Step 5 — Severe Asthma)
For patients with uncontrolled severe asthma despite high-dose ICS + LABA:
| Drug | Target | Indication |
|---|---|---|
| Omalizumab | Anti-IgE | Allergic asthma, elevated serum IgE |
| Mepolizumab, reslizumab | Anti-IL-5 | Eosinophilic asthma |
| Benralizumab | Anti-IL-5Rα | Eosinophilic asthma |
| Dupilumab | Anti-IL-4Rα (blocks IL-4 + IL-13) | Type 2 asthma, also treats atopic dermatitis |
| Tezepelumab | Anti-TSLP | Broad severe asthma (any phenotype) |
8. Systemic Corticosteroids
- Reserved for acute exacerbations and severe persistent asthma not controlled by inhaled therapy
- Oral prednisolone 40–50 mg/day for 5–7 days in acute exacerbations
- Chronic oral steroids: associated with significant adverse effects (osteoporosis, diabetes, immunosuppression, adrenal suppression); minimise where possible
GINA Stepwise Management (Adults)
| Step | Treatment |
|---|---|
| Step 1 (Mild intermittent) | As-needed low-dose ICS-formoterol (preferred) OR as-needed SABA alone |
| Step 2 (Mild persistent) | Low-dose ICS daily + as-needed SABA; or as-needed ICS-formoterol |
| Step 3 (Moderate persistent) | Low-dose ICS-LABA + as-needed SABA/ICS-formoterol; or medium-dose ICS |
| Step 4 (Moderate-severe) | Medium/high-dose ICS-LABA ± tiotropium + as-needed reliever |
| Step 5 (Severe uncontrolled) | Add biologic therapy (omalizumab, anti-IL-5, dupilumab, tezepelumab); consider low-dose oral corticosteroid |
Step-up when asthma is uncontrolled; step-down when well controlled for ≥3 months. — Murray & Nadel's Textbook of Respiratory Medicine
Classification of control (GINA):
- Well controlled: 0 of 4 criteria (no daytime symptoms >2×/week, no night waking, no activity limitation, reliever ≤2×/week)
- Partly controlled: 1–2 criteria
- Uncontrolled: 3–4 criteria
Inhaler Device Selection
Inhaled therapy is the cornerstone of asthma treatment — it delivers drug directly to the lung, requires smaller doses, has faster onset, and fewer systemic effects than oral therapy. — Fishman's Pulmonary Diseases and Disorders
| Device | Advantages | Disadvantages |
|---|---|---|
| pMDI | Portable, inexpensive, multidose | Requires hand-breath coordination; high oropharyngeal deposition |
| DPI | Breath-actuated (no coordination needed) | Requires adequate inspiratory flow |
| Nebuliser | Useful for acute/severe patients; tidal breathing | Bulky, time-consuming |
Key point: Always teach and check inhaler technique. Poor technique is a major cause of treatment failure.
Management of Acute Exacerbations (Emergency Department)
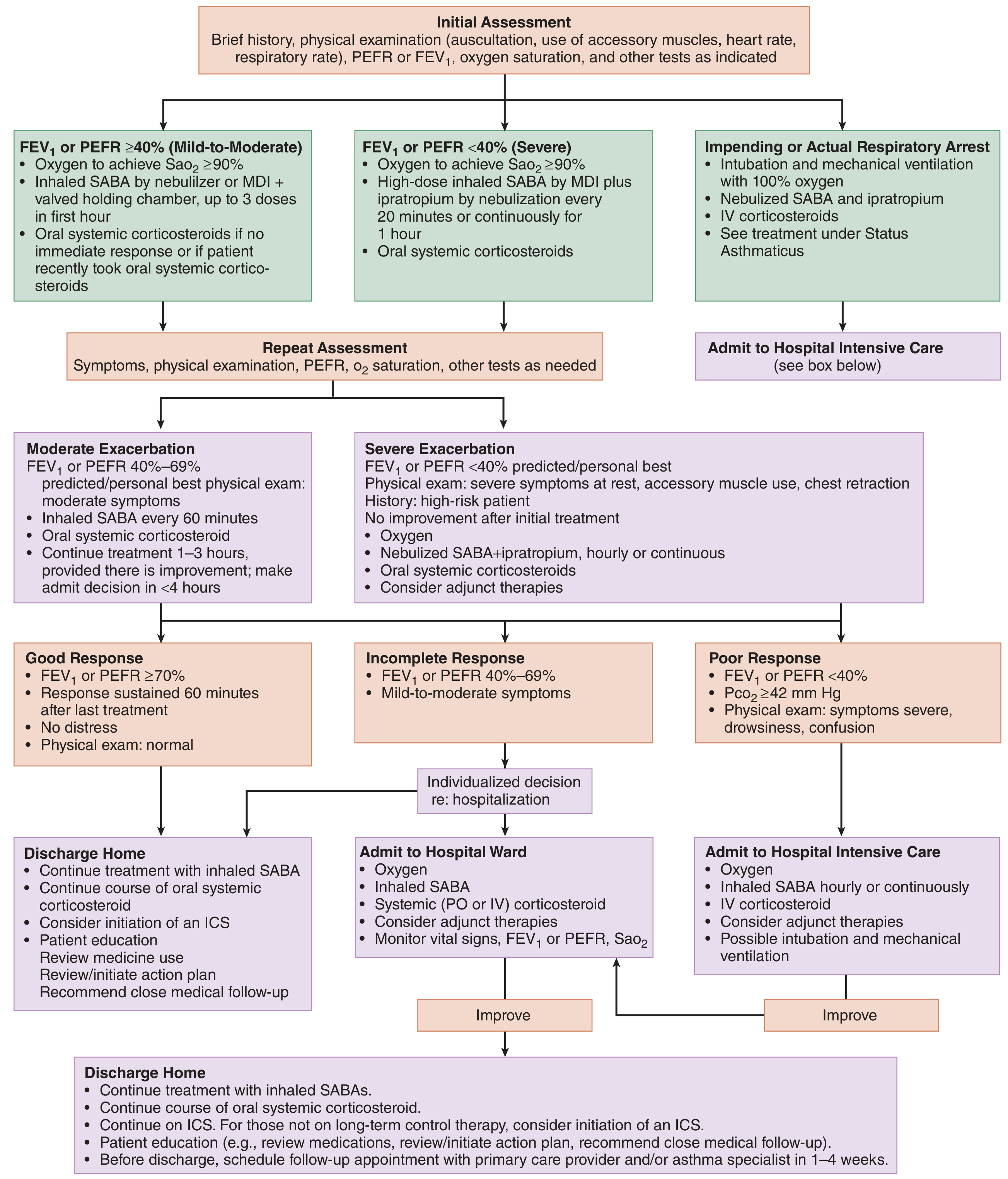
Source: Tintinalli's Emergency Medicine
Goals: rapid reversal of airflow obstruction, adequate oxygenation, reduction of inflammation.
Initial treatment (Mild–Moderate, FEV₁/PEFR ≥40%):
- Oxygen to maintain SaO₂ ≥90%
- Inhaled SABA (albuterol) via nebuliser or MDI+spacer, up to 3 doses in first hour
- Oral systemic corticosteroids if no immediate response
Severe (FEV₁/PEFR <40%):
- Oxygen
- High-dose inhaled SABA + ipratropium by nebulisation every 20 min or continuously for 1 hour
- Oral/IV systemic corticosteroids
Impending respiratory arrest:
- Intubation + mechanical ventilation with 100% oxygen
- Nebulised SABA + ipratropium
- IV corticosteroids
Albuterol dosing (acute):
- Nebuliser: 2.5–5 mg every 20 min × 3 doses, then 2.5–10 mg every 1–4 h as needed; or 10–15 mg/h continuous nebulisation
- Ipratropium: 0.5 mg every 20 min × 3 doses
Discharge criteria (Good response): FEV₁/PEFR ≥70%, sustained 60 min after last treatment, no distress. Discharge with: continued SABA, oral corticosteroid course, ICS initiation, follow-up in 1–4 weeks.
Non-Pharmacological Measures
- Allergen and trigger avoidance (house dust mite, pollen, pet dander, occupational exposures, smoke, NSAIDs in aspirin-sensitive asthma, β-blockers)
- Written Asthma Action Plan — patients use PEFR and symptoms to self-manage
- Smoking cessation
- Weight loss in obese patients (improves control significantly)
- Breathing exercises (Buteyko, diaphragmatic) — adjunct; reduce symptom perception
- Allergen immunotherapy — subcutaneous or sublingual; modifies disease in allergic asthma
Recent Evidence (2024–2025)
A 2025 JAMA network meta-analysis (PMID: 39465893) compared inhaled reliever therapies and found that ICS-formoterol used as-needed reliever was associated with better outcomes than SABA alone, supporting the GINA recommendation for ICS-containing relievers even in mild asthma.
Key sources: Katzung's Basic and Clinical Pharmacology, 16th Ed. · Murray & Nadel's Textbook of Respiratory Medicine · Fishman's Pulmonary Diseases and Disorders · Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.