Hydrocele
Reading File
Finding Sources
Searching PubMed
hydrocele
Reading File
Reading File
Reading File
Finding Sources
Searching Images
hydrocele testis scrotal swelling
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Hydrocele
Definition
A hydrocele is a fluid collection that resides within the tunica vaginalis in the scrotum, or within the processus vaginalis in the inguinal canal. It is the most common cause of painless scrotal swelling in children.
Anatomy & Embryology
As the testis descends into the scrotum, the peritoneal extension alongside it (the processus vaginalis) forms a serous covering called the tunica vaginalis. Normally, the processus vaginalis obliterates after descent. Failure of obliteration leads to various anatomic conditions:
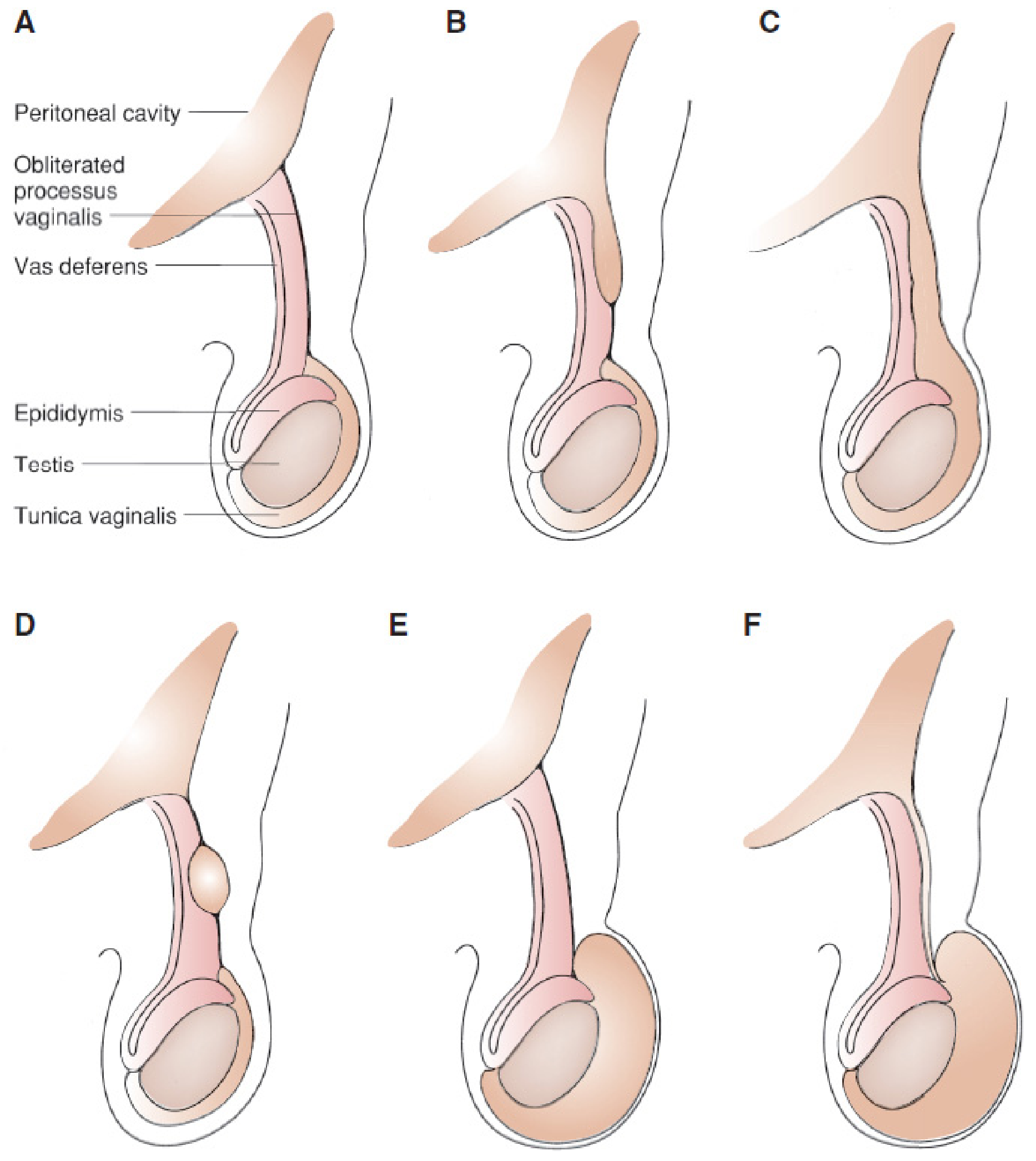
A: Normal (obliterated); B: Proximal hernia sac, distal obliterated; C: Complete hernia into scrotum; D: Hydrocele of the cord (proximal + distal obliteration, mid-segment open); E: Non-communicating scrotal hydrocele; F: Patent processus with communicating hydrocele
(Mulholland & Greenfield's Surgery, 7e)
The incidence of patent processus vaginalis is 80–94% in newborns, declining to 20–30% in adulthood.
Classification
| Type | Key Feature | Natural History |
|---|---|---|
| Non-communicating | Processus vaginalis closed; isolated residual fluid | Usually resolves by 12–18 months |
| Communicating | Patent processus vaginalis — fluid fluctuates with activity/posture | Does not resolve; synonymous with patent processus vaginalis |
| Hydrocele of the cord | Fluid in the processus vaginalis separate from tunica vaginalis | Does not resolve spontaneously |
| Hydrocele of canal of Nuck | Female equivalent; fluid trapped in processus vaginalis | — |
| Abdominoscrotal hydrocele | Rare (~1.25% of all hydroceles); tense, extends into abdomen; bilateral in ~30% | May manifest in infancy; can enlarge, improve, or rarely resolve spontaneously |
Etiology
Congenital/Primary:
- Patent processus vaginalis (children)
Secondary (acquired) causes:
- Trauma
- Epididymo-orchitis / infection
- Testicular/paratesticular tumors
- Lymphatic obstruction (e.g., post-varicocelectomy — incidence 3–33%, avg ~7%)
- Torsion of appendix testis
- Incarcerated inguinal hernia (acute hydrocele)
Clinical Features
- Painless scrotal swelling (hallmark)
- May be intermittent — resolves when supine, enlarges when upright or with Valsalva (communicating type)
- Soft, fluctuant mass; testis not separately palpable
- Transillumination positive — the fluid-filled sac illuminates brightly with a light source; contrast with solid masses or testicular enlargement which do not transilluminate
Diagnosis
Clinical: History + transillumination is usually sufficient.
Scrotal ultrasound (when needed):
- Confirms fluid collection (anechoic area surrounding testis)
- Identifies unpalpable testis surrounded by hydrocele fluid
- Differentiates simple from complex hydrocele (debris, septations = secondary cause)
- Rules out testicular malignancy
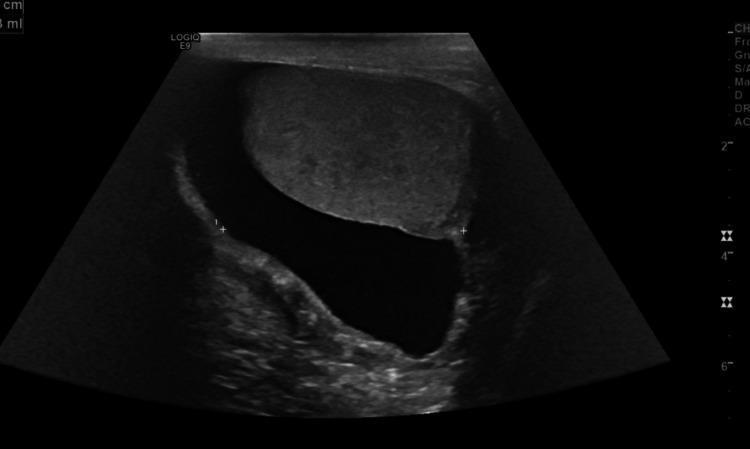
B-mode ultrasound: large anechoic fluid collection surrounding the testis — classic simple hydrocele.
Management
Infants & Children
- Non-communicating hydrocele: Observe until age 12 months — most resolve spontaneously
- Indications for surgery:
- Persists beyond age 1 year
- Enlargement or size fluctuation (implies communication developing)
- Communicating hydrocele (treat as patent processus vaginalis)
- Hydrocele of the spermatic cord (rarely resolves spontaneously)
- Acute hydrocele from incarcerated hernia → urgent surgical exploration
Surgical Techniques
- Children (communicating hydrocele): Inguinal approach — high ligation of the hernia sac at the internal inguinal ring; hydrocele sac excised
- Peripubertal/adults (non-communicating): Trans-scrotal hydrocele repair; inguinal approach only if communicating
- Laparoscopic approach: Increasingly used, particularly for bilateral cases; some centers report single-port techniques
Adults (primary/secondary hydrocele)
| Option | Notes |
|---|---|
| Observation | Asymptomatic small hydroceles |
| Aspiration ± sclerotherapy (AS) | Resolution rate 85–96%; repeat procedures may be needed |
| Hydrocelectomy | Definitive; recurrence rate 0–2% regardless of technique |
Recurrence & Complications
- Surgical recurrence: 0–2% (any operative technique)
- Sclerotherapy resolution: 85–96%
- Post-varicocelectomy hydrocele: 3–33% (avg 7%) — due to lymphatic obstruction; use of microsurgical technique almost eliminates this risk
- Large hydrocele creates an insulating layer around the testis → may impair counter-current heat exchange → potentially affects fertility after varicocelectomy
Special Considerations
Abdominoscrotal hydrocele: Tense, non-communicating scrotal mass extending retroperitoneally/preperitoneally. Ultrasound defines proximal extent. Associated with cryptorchidism, contralateral hernia/hydrocele, and vanishing testis.
Emergency differentiation: Acute non-communicating hydrocele must be differentiated from incarcerated inguinal hernia and inguinal lymphadenitis — transillumination and palpation of normal cord structures above the mass help distinguish.
Sources: Campbell-Walsh-Wein Urology; Mulholland & Greenfield's Surgery, 7e; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.