Iron deficiency anaemia
Reading File
Finding Sources
Searching PubMed
"iron deficiency anemia"[MeSH Terms] AND "diagnosis OR treatment"
Finding Sources
Searching PubMed
"iron deficiency anemia"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of iron deficiency anaemia (IDA), drawn from Goldman-Cecil Medicine, Harrison's Principles, and the Tietz Textbook of Laboratory Medicine.
Iron Deficiency Anaemia
Definition
Iron deficiency occurs when body iron stores are insufficient to support normal iron metabolism. It exists on a spectrum:
- Iron deficiency without anaemia - depleted stores cause fatigue, alopecia, and tissue symptoms before the blood count falls
- Iron deficiency anaemia (IDA) - further depletion impairs erythropoiesis, producing progressive microcytic anaemia
- Functional iron deficiency - stores are adequate but iron cannot be mobilised (e.g. in chronic inflammation due to hepcidin excess)
Epidemiology
IDA is the most common nutritional deficiency worldwide. Approximately half of the estimated 1 billion people with anaemia globally have iron deficiency, with highest prevalence in South Asia and Sub-Saharan Africa. In the United States:
- 1-2% of adult men
- ~14.7% of premenopausal women
- ~18% of pregnant women
- 11% of preschool children
Women are at greatest risk due to menstrual losses (average 16 mg iron per cycle). Pregnancy requires ~900 mg of iron stores in total, with demands rising to 6 mg/day in the third trimester.
Causes
| Category | Examples |
|---|---|
| Increased losses | Menorrhagia, GI bleeding (ulcers, cancer, NSAIDs), haematuria |
| Increased demand | Pregnancy, growth in infancy/adolescence |
| Decreased intake | Poor diet, vegetarian/vegan diet (non-haem iron poorly absorbed) |
| Malabsorption | Coeliac disease, autoimmune gastritis, H. pylori, post-gastrectomy, bariatric surgery |
Important: Gastrointestinal cancer (especially colon, also gastric) is found in up to 10% of older patients with IDA. Any man with unexplained IDA, or iron-deficient women over 40, should undergo upper and lower GI endoscopy.
Pathophysiology
Iron absorption: Dietary iron exists as haem iron (in meat, Fe²+, 30-40% absorbed) and non-haem iron (Fe³+, reduced to Fe²+ by gastric acid, then transported by DMT1 - far less efficient). Iron exits the enterocyte via ferroportin and binds transferrin in plasma.
Hepcidin regulation: Hepcidin is the master regulator of iron homeostasis, produced by the liver. It binds ferroportin and causes its degradation, blocking export of iron from enterocytes, macrophages, and hepatocytes. In iron deficiency, hepcidin is suppressed, allowing maximal absorption. In chronic inflammation, elevated IL-6 drives hepcidin upregulation, creating functional iron deficiency (the anemia of chronic disease).
Iron stores: Ferritin stores up to 4,000 iron atoms per molecule. Transferrin carries iron to the bone marrow, where developing red cells internalise the transferrin-receptor complex by endocytosis. Iron in senescent RBCs is recycled by macrophages - this cycle is >95% efficient.
Clinical Features
Because IDA often develops gradually, patients can tolerate marked anaemia before presenting. Features include:
Symptoms of anaemia: Fatigue (most common and disabling), dyspnoea on exertion, palpitations, worsening angina in older patients.
Symptoms specific to iron deficiency itself:
- Hair loss (diffuse non-scarring alopecia; ferritin <100 ng/mL)
- Cold intolerance (iron is needed for thyroid hormone efficacy)
- Restless leg syndrome
- Pica (craving for ice - pagophagia - is sensitive and specific; or clay/earth - geophagia)
- Pruritus, easy bruising
Signs of severe/chronic IDA:
- Koilonychia (spoon-shaped nails)
- Glossitis, angular stomatitis
- Plummer-Vinson syndrome (dysphagia from oesophageal webs)
- Pallor
Blood Film
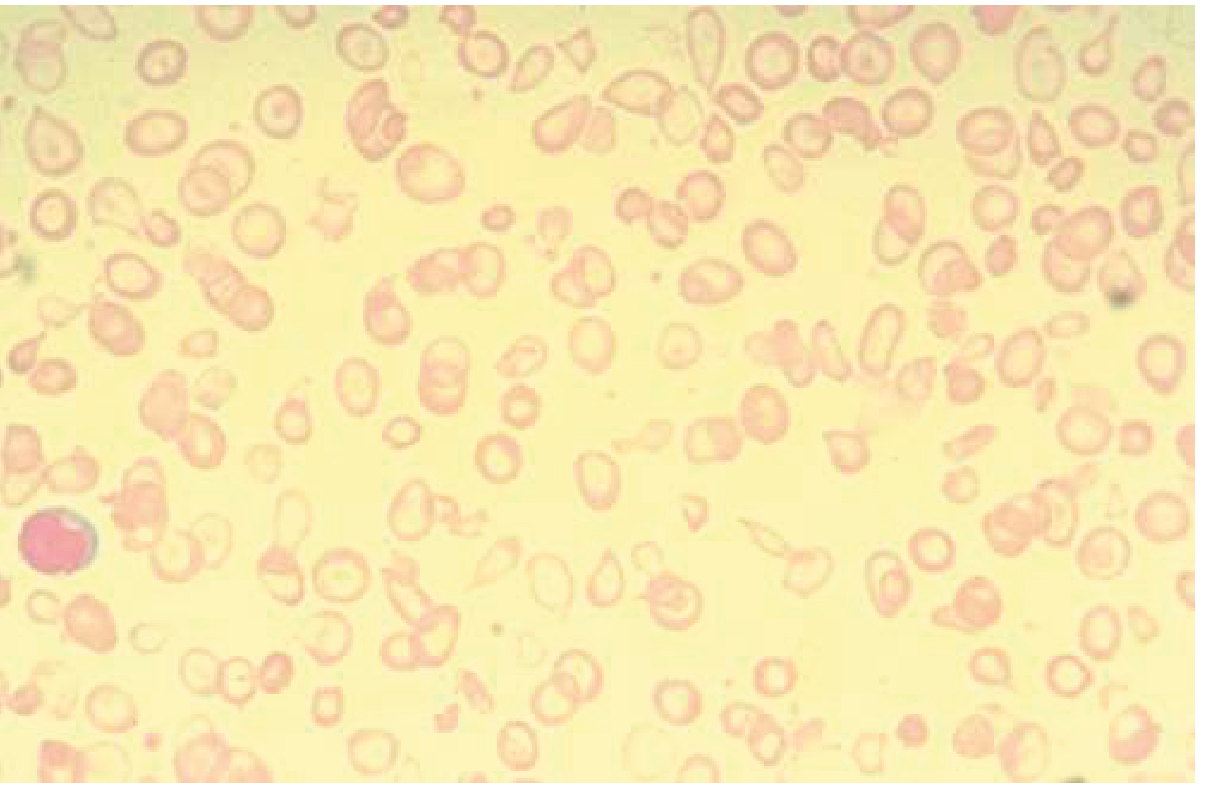
Microcytic, hypochromic red cells with marked anisocytosis and poikilocytosis - characteristic of iron deficiency anaemia. Note the small cell size and enlarged central pallor (>1/3 of cell diameter).
Diagnosis
Key Lab Tests
| Test | In IDA | Notes |
|---|---|---|
| Serum ferritin | Low (<15 ng/mL is highly specific; <30 is suggestive) | Best first-line test; but ferritin is an acute-phase reactant - can be falsely normal/high in inflammation. Ferritin >100 ng/mL makes IDA unlikely even with inflammation |
| Serum iron | Low | Unreliable alone - varies day to day, falsely elevated after oral iron dose |
| TIBC (transferrin) | High | Elevated in IDA; but sensitivity is low (reduced by inflammation, aging, malnutrition) |
| Transferrin saturation | Low (<16-20%) | Unreliable alone; also low in anaemia of chronic disease |
| MCV / RBC indices | Low MCV (microcytosis), low MCH (hypochromia) | Late finding in severe IDA; normal in early IDA |
| Reticulocyte count | Low/normal | No reticulocytosis (unlike haemolytic anaemia) |
| Soluble transferrin receptor (sTfR) | High | Useful in inflammatory states; sTfR/log ferritin ratio helps distinguish IDA from anaemia of chronic disease |
| Bone marrow iron stain | Absent iron stores | Gold standard, but rarely necessary |
Diagnostic thresholds to remember:
- Ferritin <15 ng/mL: very specific for IDA
- Ferritin <50 ng/mL: consider abnormal in a symptomatic patient
- Ferritin <100 μg/L: most accepted threshold when inflammation is present
- In CHF/CKD: IDA also defined by transferrin saturation <20% regardless of ferritin
Differential Diagnosis of Microcytic Anaemia
| Condition | Ferritin | Serum Iron | TIBC | Distinguishing feature |
|---|---|---|---|---|
| IDA | Low | Low | High | Response to iron treatment |
| Anaemia of chronic disease | Normal/High | Low | Low/Normal | Raised CRP/ESR, hepcidin elevated |
| Thalassaemia | Normal/High | Normal | Normal | Target cells, Hb electrophoresis |
| Sideroblastic anaemia | High | High | Low | Ring sideroblasts on bone marrow |
Treatment
1. Identify and Treat the Underlying Cause
This is the priority. Blood loss must always be assumed given the body has no active iron excretion mechanism.
2. Oral Iron
- Ferrous sulfate 325 mg once daily is standard; contains ~65 mg elemental iron
- Lower doses (15-20 mg elemental iron/day) are equally effective with fewer GI side effects
- Alternatives: ferrous gluconate (less elemental iron, better tolerated), ferrous fumarate
- Take on empty stomach or with meat protein to maximise absorption
- Vitamin C enhances absorption; calcium, fibre, tea, coffee inhibit absorption (tea can reduce absorption by 90%, coffee by ~60%)
- Reticulocyte count rises within 1 week; Hb begins rising by week 2
- Continue until ferritin reaches 50-100 ng/mL (stores replete)
- 30-50% of patients have GI side effects (constipation, nausea, epigastric pain) - reduce dose or switch to alternate-day dosing
Reasons for failure of oral iron: poor adherence, ongoing blood loss, malabsorption (coeliac disease, autoimmune gastritis, H. pylori), persistent menorrhagia
3. Intravenous Iron
Indicated when:
- Oral iron is not tolerated or absorbed
- Rapid repletion is needed (pre-surgery, severe symptoms)
- Ongoing significant losses (e.g. inflammatory bowel disease, dialysis)
- Heart failure (IV iron is superior to oral in CHF patients)
Available IV preparations include ferric carboxymaltose, ferumoxytol, iron sucrose, and low molecular weight iron dextran. A pragmatic 1000 mg replacement dose is used (formulas calculating total iron deficit are unreliable). Check ferritin 2-4 weeks post-infusion; if <50 ng/mL, repeat. Mild infusion reactions are managed by slowing the rate ± corticosteroids. Anaphylaxis requires epinephrine, fluids, and transfer to acute care.
4. Blood Transfusion
Reserved for haemodynamic instability or severe symptomatic anaemia (e.g. Hb <7 g/dL with cardiac symptoms). Does not replete iron stores.
Special Situations
- Heart failure: IDA is present in 50-60% of CHF patients. IV iron replacement improves quality of life and reduces hospitalisation, though mortality benefit is unproven.
- CKD/dialysis: Proactive iron treatment is preferred over reactive; functional iron deficiency is common due to elevated hepcidin.
- Restless leg syndrome: Iron replacement markedly reduces symptoms when ferritin is low.
- Non-anaemic iron deficiency: Iron supplementation improves fatigue in iron-deficient women even without anaemia (ferritin <50 ng/mL).
Prevention
Recommended dietary iron intake:
- Adult men and postmenopausal women: 8 mg/day
- Premenopausal women: 18 mg/day
- Pregnancy: 27 mg/day
Haem iron from meat is far more bioavailable. Non-meat sources (legumes, leafy vegetables, fortified foods) contain non-haem iron with much lower absorption.
Prognosis
Excellent once stores are replete and the underlying cause addressed. Patients after bariatric surgery or with inflammatory bowel disease may require chronic IV iron infusions to maintain adequate stores.
Sources: Goldman-Cecil Medicine (International Ed.), Harrison's Principles of Internal Medicine 22e (2025), Tietz Textbook of Laboratory Medicine 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.