Fibroendenoma of breast
Reading File
Finding Sources
Searching PubMed
"fibroadenoma" AND "breast"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Fibroadenoma of the Breast
Definition and Overview
A fibroadenoma is the most common benign stromal tumor of the female breast and the most frequent cause of a breast lump in women aged 15-25 years. It is a fibroepithelial tumor arising from hyperplasia of a single breast lobule, consisting of both epithelial and stromal (fibrous) components.
Etiopathogenesis
-
Arises from hyperplasia of intralobular stroma and ductal epithelium within a single breast lobule.
-
Two-thirds harbor driver mutations in MED12 - a gene encoding a subunit of the mediator complex that regulates RNA polymerase II-dependent transcription. This same mutation is found in uterine leiomyomas (both arising from hormone-responsive stromal cells).
-
~One-third have mutations in RARA (retinoic acid receptor alpha), an estrogen target gene.
-
The tumor is hormonally responsive - grows during pregnancy, may regress post-menopause.
-
Almost half of females on cyclosporin A after renal transplantation develop multiple bilateral fibroadenomas (likely reactive hyperplasia).
-
Robbins Pathologic Basis of Disease, p. 984
Types / Classification
By Histological Pattern
| Type | Description | Size | Age Group |
|---|---|---|---|
| Pericanalicular | Fibrous tissue surrounds small tubular (round) glands | Smaller, hard | 15-30 years |
| Intracanalicular | Glands are compressed into elongated slit-like clefts by fibrous tissue | Larger, soft | 35-50 years |
In practice, both patterns are often seen in the same tumor.
By Size / Special Subtypes
-
Simple fibroadenoma - typical, <5 cm, slight increase in cancer RR (1.5-1.7)
-
Giant fibroadenoma - >5 cm; descriptive term; excision recommended
-
Juvenile fibroadenoma - large, more cellular histologically; occurs in adolescents; excision if >5 cm or persists to adulthood
-
Complex fibroadenoma - contains cysts >0.3 cm, sclerosing adenosis, epithelial calcifications, or papillary apocrine change; cancer RR 3.4-3.7; especially high RR (3.0-4.0) with family history of breast cancer
-
Myxoid fibroadenoma - sporadic or associated with Carney complex (autosomal dominant; PRKAR1A mutations)
-
Bailey and Love's Short Practice of Surgery 28th ed., p. 408; Robbins, p. 984
Morphology / Pathology
Gross
- Well-circumscribed, rubbery, gray-white nodule that bulges above surrounding tissue
- Contains slit-like spaces lined by epithelium
- Usually 2-3 cm; surrounded by a well-defined capsule
- In older females: stroma is densely hyalinized, epithelium is atrophic
Microscopic
- Delicate, often myxoid stroma resembling normal intralobular stroma
- Pericanalicular pattern: stroma surrounds patent round/oval ducts
- Intracanalicular pattern: stroma compresses and distorts ducts into cleft-like spaces (the "interlocking antlers" appearance on H&E)
- Sharply delimited from surrounding tissue
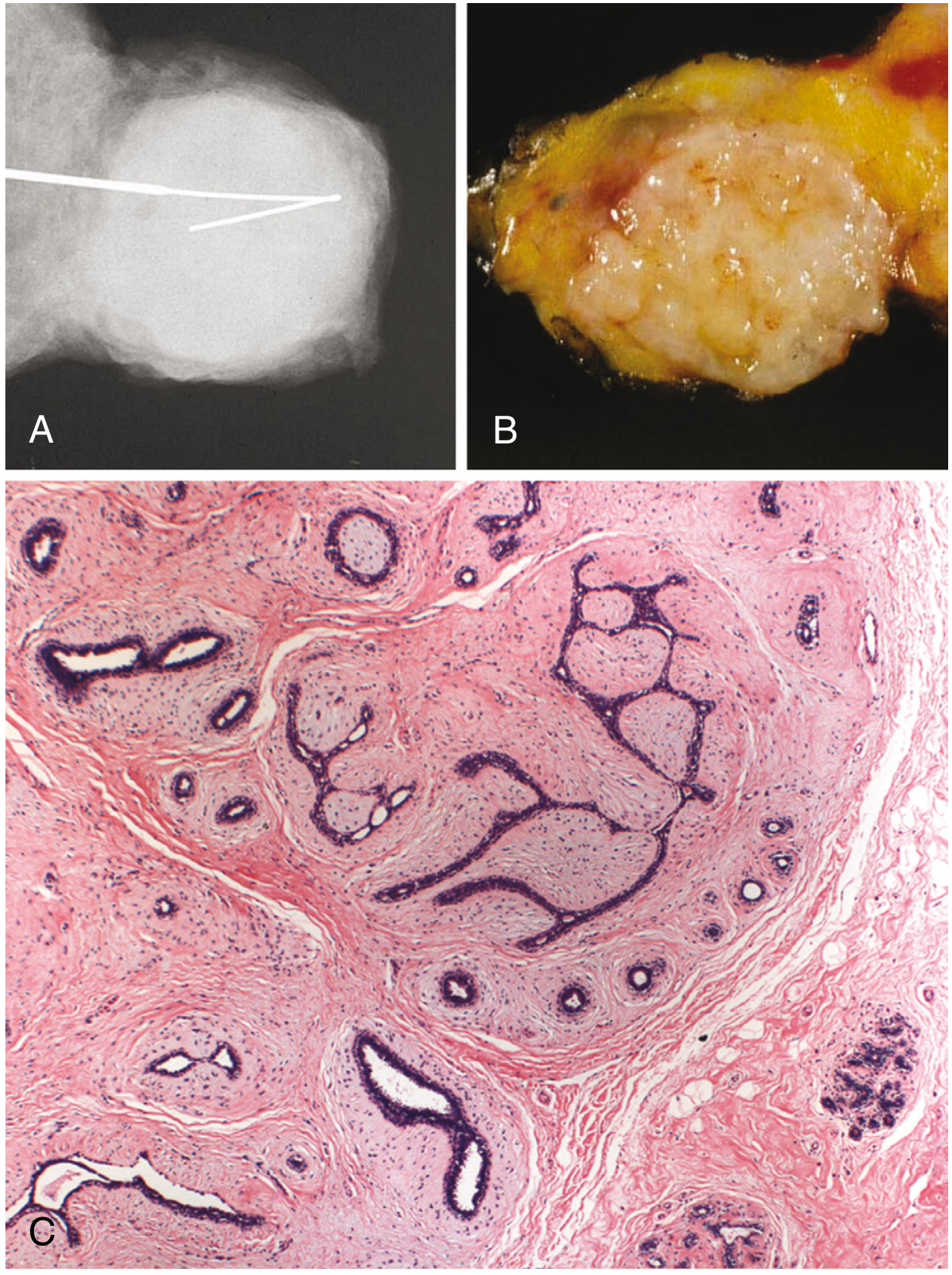
- Robbins Pathologic Basis of Disease, p. 984
Clinical Features
-
Age: most common in women in their 20s and 30s; pericanalicular type in 15-30 yr, intracanalicular in 35-50 yr
-
Presentation: painless, solitary lump (occasionally multiple/bilateral)
-
Examination findings:
- Smooth, firm, well-defined margin
- Not fixed to skin or deeper structures
- Highly mobile within breast - classically called "breast mouse" or "floating tumor"
- No axillary lymphadenopathy
- No skin changes, no nipple discharge
-
Multiple and bilateral fibroadenomas are not uncommon
-
Rapid growth during pregnancy (occasionally with infarction) can mimic carcinoma
-
Regresses after menopause
-
S Das Manual on Clinical Surgery 13th ed., p. 434
Investigations
Triple Assessment (standard approach)
- Clinical examination - characteristic "breast mouse" mobility
- Imaging
- Ultrasonography (preferred in young women <35 yr): well-circumscribed, oval, homogeneous hypoechoic mass with gentle lobulations; posterior acoustic enhancement
- Mammography: well-circumscribed density; may show "popcorn" calcifications in older/involuting lesions
- Tissue diagnosis (FNAC / core biopsy)
- FNAC: shows clusters of benign ductal epithelial cells with background stromal fragments ("antler-horn" stroma)
- Core biopsy: required if >25 years or atypical features
A clinically typical fibroadenoma confirmed on ultrasonography may be observed without biopsy (if the patient is under 25).
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Breast cyst | Fluctuant, transilluminates, US shows anechoic |
| Phyllodes tumor | Larger, bosselated surface, older women (>30 yr), stromal overgrowth on histology |
| Breast carcinoma | Hard, irregular, fixed, skin changes, lymphadenopathy |
| Breast abscess | Tender, hot, fluctuant, fever |
| Lipoma | Soft, lobulated, fatty consistency |
Risk of Malignancy
| Lesion | Relative Risk (RR) |
|---|---|
| Simple fibroadenoma | 1.5-1.7 |
| Complex fibroadenoma | 3.4-3.7 |
| Complex fibroadenoma + family history | 3.0-4.0 |
Cancer arising within a fibroadenoma is rare. The surrounding breast parenchyma (e.g., atypical hyperplasia found nearby) is thought to be the true driver of elevated risk in complex fibroadenomas.
- Bailey and Love 28th ed., p. 414-415; Robbins, p. 984
Management
Conservative (Observation)
- Indicated in women under 25-30 years with typical clinical and US features
- Natural history: regression (~30%), stable, or slow growth
- Regression with tamoxifen or ormeloxifene (anti-oestrogen drugs) has been observed
Indications for Surgical Excision
- Age >30 years
- Suspicious features on imaging (e.g., microlobulation)
- Atypia on histology/cytology
- Size >5 cm (giant fibroadenoma)
- Family history of breast cancer
- Patient preference
- Excision in elderly should include a rim of normal tissue (to exclude malignancy or phyllodes tumor)
Surgical Technique
- Enucleation through a periareolar or submammary (Gaillard Thomas) incision
- Giant fibroadenomas are often enucleated through a submammary incision
Minimally Invasive Options (emerging)
Recent evidence supports non-surgical ablation:
-
Cryoablation - systematic reviews (2025) confirm safety and efficacy for benign fibroadenomas [PMID: 41061430]
-
High-Intensity Focused Ultrasound (HIFU) - a 2026 systematic review and meta-analysis showed comparable efficacy and safety to cryoablation [PMID: 42147239]
-
Bailey and Love 28th ed.; Sabiston Textbook of Surgery 21st ed.
Fibroadenoma vs. Phyllodes Tumor - Key Comparison
| Feature | Fibroadenoma | Phyllodes Tumor |
|---|---|---|
| Age | 15-35 yr | >30 yr |
| Size | Usually 2-3 cm | Often large (can be massive) |
| Growth | Slow | Rapid |
| Surface | Smooth | Bosselated |
| Stroma | Myxoid, loose | Cellular, mitotically active |
| Behavior | Benign | Benign/borderline/malignant |
| MED12 mutations | Yes (2/3) | Yes (majority) |
| TERT/TP53/RB mutations | Rare | More common (malignant types) |
| Treatment | Conservative/enucleation | Wide local excision |
Summary
Fibroadenoma is a benign, hormonally responsive, fibroepithelial tumor of the breast driven largely by MED12 mutations. It presents as a painless, mobile "breast mouse" in young women. Management is conservative in typical cases in young women; surgical excision (enucleation) is indicated for size >5 cm, atypical features, or patient preference. Minimally invasive ablation (cryoablation, HIFU) is increasingly supported by evidence as an alternative to surgery.
Sources: Robbins Pathologic Basis of Disease (p. 984) | Bailey and Love's Short Practice of Surgery 28th ed. | S Das Manual on Clinical Surgery 13th ed. (p. 434) | Sabiston Textbook of Surgery 21st ed. | Recent systematic reviews: PMID 41061430 (cryoablation, 2025), PMID 42147239 (HIFU vs cryoablation, 2026)
Fibroendenoma of breast
The previous response already covered fibroadenoma of the breast in full detail. Here is a clean, consolidated reference:
Fibroadenoma of the Breast
Definition
A fibroadenoma is the most common benign fibroepithelial tumor of the female breast, arising from hyperplasia of a single breast lobule. It contains both epithelial and stromal (fibrous) components.
Etiopathogenesis
- Arises from intralobular stroma of a breast lobule
- 2/3 harbor MED12 mutations (mediator complex subunit regulating RNA Pol II transcription) - same mutation seen in uterine leiomyomas
- ~1/3 have RARA mutations (retinoic acid receptor alpha, an estrogen target gene)
- Tumor is hormonally responsive: grows during pregnancy, regresses post-menopause
- Cyclosporin A after renal transplant can trigger multiple bilateral fibroadenomas
Classification
By Histological Pattern
| Type | Stroma-Duct Relationship | Size | Consistency | Age |
|---|---|---|---|---|
| Pericanalicular | Fibrous tissue surrounds round/oval patent ducts | Smaller | Hard | 15-30 yr |
| Intracanalicular | Fibrous tissue compresses ducts into elongated cleft-like spaces | Larger | Soft | 35-50 yr |
Both patterns often coexist in the same tumor.
By Size / Special Subtypes
| Subtype | Definition | Management |
|---|---|---|
| Simple | Typical, <5 cm | Observe / enucleate |
| Giant | >5 cm | Excision recommended |
| Juvenile | Large, cellular; adolescents | Observe if <5 cm; excise if >5 cm or persists |
| Complex | Cysts >0.3 cm + sclerosing adenosis / calcifications / apocrine change | Higher cancer RR; closer follow-up |
| Myxoid | Sporadic or Carney complex (PRKAR1A mutation) | Per size/symptoms |
Pathology / Morphology
Gross
- Well-circumscribed, rubbery, gray-white nodule with a defined capsule
- Bulges above surrounding tissue on cut section
- Contains slit-like spaces lined by epithelium
- In older women: densely hyalinized stroma, atrophic epithelium
Microscopic
- Delicate, myxoid stroma resembling normal intralobular stroma
- Pericanalicular: stroma surrounds patent ducts
- Intracanalicular: stroma distorts ducts into compressed clefts ("antler-horn" pattern)
- Sharp demarcation from surrounding breast tissue
Clinical Features
- Most common breast lump in women aged 15-25 years
- Presentation: painless, solitary lump (may be multiple/bilateral)
- Examination:
- Smooth, firm, well-defined margin
- Not fixed to skin or deeper structures
- Highly mobile - classically called "breast mouse" or "floating tumor"
- No skin tethering, no nipple discharge
- No axillary lymphadenopathy
Investigations (Triple Assessment)
- Clinical examination - characteristic mobility
- Imaging
- Ultrasonography (preferred <35 yr): oval, well-circumscribed, homogeneous hypoechoic mass; posterior acoustic enhancement
- Mammography: well-circumscribed density; "popcorn" calcifications in involuting lesions
- Tissue diagnosis
- FNAC: clusters of benign ductal epithelial cells + stromal fragments (antler-horn stroma)
- Core biopsy: if age >25 or atypical features on imaging
A clinically typical fibroadenoma confirmed on ultrasound in a woman under 25 may be observed without biopsy.
Differential Diagnosis
| Condition | Key Differentiator |
|---|---|
| Breast cyst | Fluctuant, transilluminates, anechoic on US |
| Phyllodes tumor | Larger, bosselated, rapid growth, age >30 yr |
| Breast carcinoma | Hard, irregular, fixed, skin changes, lymphadenopathy |
| Breast abscess | Tender, warm, fluctuant, fever |
| Lipoma | Soft, lobulated, fatty consistency |
Risk of Malignancy
| Lesion | Relative Risk (RR) for Breast Cancer |
|---|---|
| Simple fibroadenoma | 1.5-1.7 |
| Complex fibroadenoma | 3.4-3.7 |
| Complex fibroadenoma + family history | 3.0-4.0 |
Cancer arising directly within a fibroadenoma is rare. The elevated RR in complex fibroadenomas is largely attributed to co-existing atypical hyperplasia in surrounding breast tissue.
Management
Conservative (Observation)
- Women <25-30 yr with typical clinical + US features
- Natural history: regression, stability, or slow growth
- Anti-estrogen therapy: tamoxifen or ormeloxifene can induce regression
Indications for Surgical Excision
- Age >30 years
- Size >5 cm (giant fibroadenoma)
- Suspicious / atypical features on imaging
- Atypia on histology / cytology
- Family history of breast cancer
- Rapid growth or change in character
- Patient's preference
- In elderly: excise with a rim of normal tissue (to exclude phyllodes or malignancy)
Surgical Technique
- Enucleation through a periareolar or submammary (Gaillard Thomas) incision
- Giant fibroadenomas: submammary incision preferred
Minimally Invasive Ablation (emerging evidence)
- Cryoablation: systematic review (2025, PMID 41061430) confirms safety and efficacy
- HIFU (High-Intensity Focused Ultrasound): 2026 meta-analysis (PMID 42147239) shows comparable outcomes to cryoablation
Fibroadenoma vs. Phyllodes Tumor
| Feature | Fibroadenoma | Phyllodes Tumor |
|---|---|---|
| Age | 15-35 yr | >30 yr (typically) |
| Size | 2-3 cm typical | Often large or massive |
| Growth | Slow | Rapid |
| Surface | Smooth | Bosselated / irregular |
| Stroma | Myxoid, loose | Cellular, mitotically active |
| Behavior | Always benign | Benign / borderline / malignant |
| MED12 mutations | Yes (~2/3) | Yes (majority) |
| TERT / TP53 / RB mutations | Rare | Present in malignant types |
| Treatment | Conservative / enucleation | Wide local excision |
Phyllodes tumors are classified by mitotic rate: benign (<4/10 HPF), borderline (4-9/10 HPF), malignant (>10/10 HPF).
Sources: Robbins Pathologic Basis of Disease (p. 984) | Bailey and Love's Short Practice of Surgery 28th ed. | S Das Manual on Clinical Surgery 13th ed. | Sabiston Textbook of Surgery 21st ed. | PMID 41061430 | PMID 42147239
This is a shared conversation. Sign in to Orris to start your own chat.