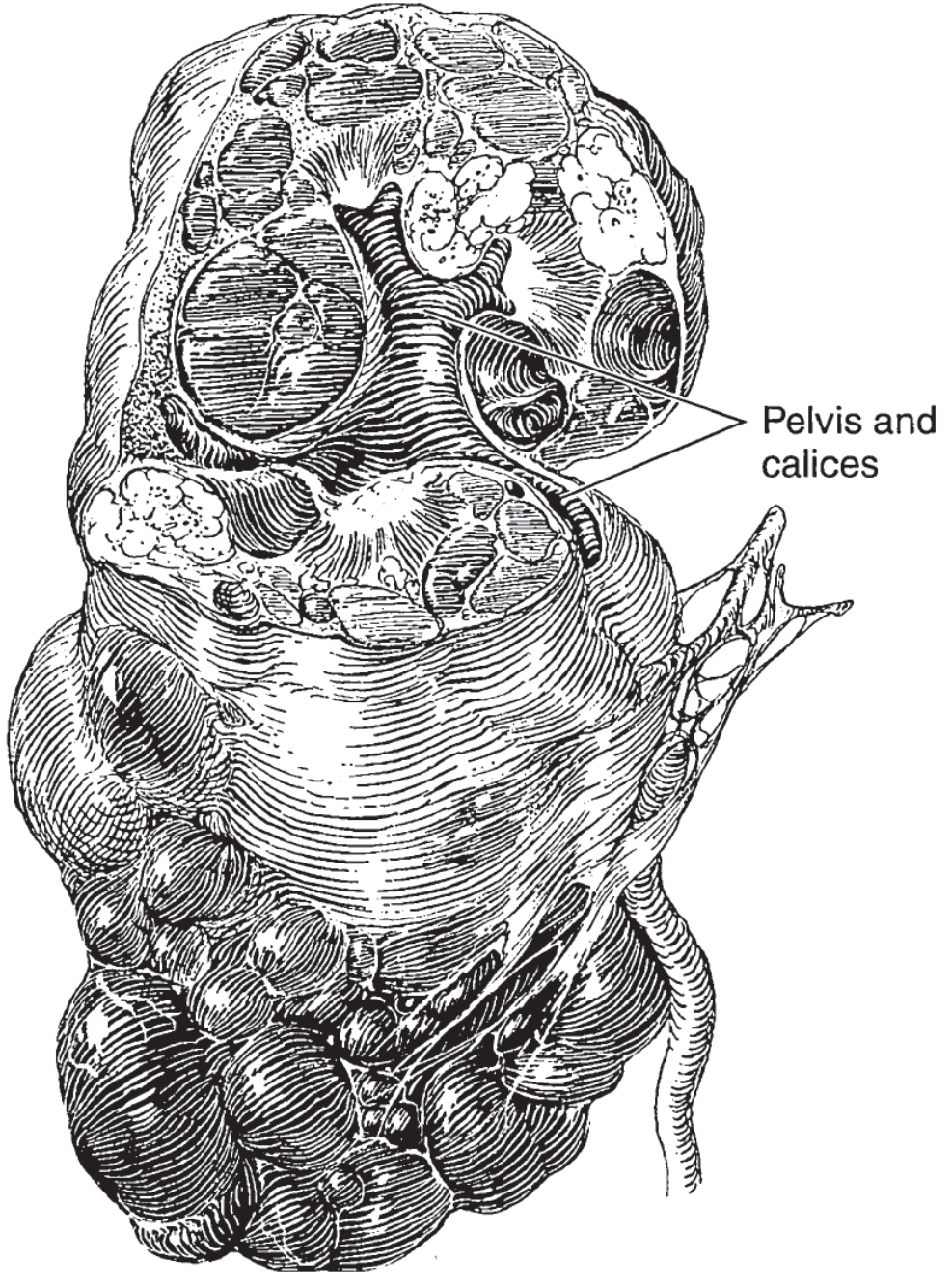
Polycystic kidney
Reading File
Finding Sources
Searching PubMed
"polycystic kidney disease"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer.
Polycystic Kidney Disease (PKD)
PKD is a group of hereditary disorders characterized by progressive bilateral renal cyst development leading to kidney enlargement and eventual renal failure. Two major forms exist: autosomal dominant (ADPKD) and autosomal recessive (ARPKD).
1. Autosomal Dominant PKD (ADPKD)
Epidemiology
- Prevalence: 1 in 400 to 1 in 1000 - one of the most common hereditary diseases
- Accounts for ~5% of end-stage kidney disease (ESKD) in the US
- More progressive in men than women (gender ratio 1.2-1.3)
- ~30,000 patients have ESKD due to ADPKD in the United States
Genetics
ADPKD is autosomal dominant with complete penetrance for cyst development. Each child of an affected parent has a 50% chance of inheriting the abnormal gene. At least 10% of families arise from de novo mutations.
Two major causative genes:
| Gene | Chromosome | % of Cases | Average Age at ESKD |
|---|---|---|---|
| PKD1 | 16p13.3 | ~78% | 58.1 years |
| PKD2 | 4q21 | ~15% | 79.7 years |
- ~7% have no detectable mutation
- Two newer genes - GANAB and DNAJB11 - produce ADPKD-like phenotypes
- Homozygous mutations in either PKD1 or PKD2 are lethal in utero
- Patients heterozygous for both PKD1 and PKD2 mutations have more severe disease than those with one mutation alone
Pathogenesis
The proteins polycystin-1 (PC1, encoded by PKD1) and polycystin-2 (PC2, encoded by PKD2) form a receptor/ion channel complex localized to primary cilia and the endoplasmic reticulum. Loss-of-function leads to dysregulation of intracellular calcium, increased cAMP signaling, and activation of the mTOR pathway - collectively driving abnormal tubular epithelial proliferation, fluid secretion into cysts, and extracellular matrix remodeling.
Pathology
- Kidneys become massively enlarged, studded with innumerable fluid-filled cysts of all sizes
- Cysts arise from any segment of the nephron (glomerulus to collecting duct) but most originate from the distal tubule and collecting duct
- Cyst fluid is usually amber-colored; may be hemorrhagic
- In end-stage disease, only scattered patches of normal parenchyma remain, with tubulointerstitial fibrosis and arteriolar sclerosis
- Liver cysts are present in up to 90% of adults - the most common extrarenal manifestation
Clinical Features
Symptoms:
- Flank/abdominal pain (from the weight of enlarged kidneys, hemorrhage into a cyst, or infection)
- Gross or microscopic hematuria (can be severe)
- Renal colic (from clots or stones)
- Abdominal mass
- Symptoms of UTI/pyelonephritis
- Nausea, vomiting, weakness, headache when renal insufficiency develops
Signs:
- Palpable, nodular kidneys (bilateral)
- Hypertension in 60-70% of patients (often presents before GFR declines - driven by intrarenal RAAS activation)
- Cardiac enlargement secondary to hypertension
Disease Progression
Kidney volume is the strongest predictor of renal function decline. The CRISP (Consortium for Radiologic Imaging Studies of PKD) cohort showed:
- A height-adjusted total kidney volume (htTKV) ≥600 mL/m at baseline most accurately predicts development of stage 3 CKD within 8 years (AUC 0.84)
- Baseline htTKV remained an independent predictor even at 13-year follow-up; OR 1.35 per 100 mL/m increment for reaching stage 5 CKD or ESRD
- Reduced renal blood flow (increased vascular resistance) is an independent predictor of GFR decline
- Notably, ADPKD patients have less anemia than other CKD patients because polycystic kidneys produce excess erythropoietin
Extrarenal Manifestations
| System | Manifestation |
|---|---|
| Liver | Hepatic cysts (up to 90% of adults); polycystic liver disease (PLD) - usually asymptomatic |
| Vascular | Intracranial aneurysms (ICAs) in ~8% of patients; also aortic and coronary aneurysms, mitral valve prolapse, aortic root dilatation |
| GI | Diverticulosis; abdominal wall/inguinal hernias |
| Pancreas | Pancreatic cysts |
| Other | Seminal vesicle cysts, arachnoid cysts |
Intracranial aneurysms: Occur in ~8% of patients with ADPKD vs. ~3% in the general population. Rupture risk by aneurysm size (ISUIA data): 0% for <7 mm, 2.6-14.5% for 7-12 mm, 14.5-18.4% for 13-24 mm, 44-50% for ≥25 mm at 5 years.
Diagnosis
Ultrasound (first-line) - Revised Pei criteria for at-risk individuals (parent/sibling with ADPKD):
- Age 15-39 years: ≥3 renal cysts (unilateral or bilateral) - PPV 100%
- Age 40-59 years: ≥2 cysts in each kidney - PPV 100%
- Age ≥60 years: ≥4 cysts in each kidney
MRI is more sensitive and is used for total kidney volume measurement (for risk stratification and tolvaptan eligibility). Molecular genetic testing is available but reserved for young at-risk individuals being evaluated as living kidney donors or when imaging is equivocal.
Management
Hypertension:
- ACE inhibitors or ARBs are first-line (block the intrarenal RAAS)
- Target BP: The HALT-PKD trial showed aggressive BP control (95-110/60-75 mmHg) in younger patients slowed kidney volume growth and reduced left ventricular mass index
Disease-modifying therapy:
- Tolvaptan (vasopressin V2-receptor antagonist) - the first approved therapy to slow cyst growth and GFR decline in patients with rapidly progressive ADPKD (htTKV-based Mayo classification 1C-1E or PRO-PKD score >6). The TEMPO 3:4 and REPRISE trials demonstrated significant reduction in kidney volume growth and GFR decline. Hepatotoxicity is a risk - requires REMS enrollment and monitoring.
- mTOR inhibitors (sirolimus, everolimus) - showed reduction in kidney volume growth in trials but did not preserve GFR; not currently standard of care
- Statins, dietary protein restriction, and increased water intake (to suppress AVP) are often recommended but lack robust trial evidence
Complications:
- Cyst infection: fluoroquinolones or TMP-SMX (penetrate into cyst fluid)
- Hematuria: conservative management; spontaneously resolves in most cases
- Nephrolithiasis: 20-36% prevalence; uric acid and calcium oxalate stones
Renal replacement therapy:
- ADPKD patients on peritoneal dialysis (PD) have similar or better outcomes than other PD patients. Concern about large kidney volume causing inadequate dwell volume occasionally necessitates nephrectomy before initiating PD.
- Kidney transplantation: outcomes are excellent; bilateral native nephrectomy may be required for space
2. Autosomal Recessive PKD (ARPKD)
Epidemiology & Genetics
- Prevalence: 1 in 20,000; carrier frequency ~1 in 70
- Caused by mutations in PKHD1 (chromosome 6p21.1-p12) encoding fibrocystin (also called polyductin)
- PKHD1 is one of the largest human genes (~470 kb, 67 exons)
- Two truncating mutations = lethal neonatal phenotype; at least one non-truncating mutation = survival possible
- Biallelic mutations in DZLP1 or specific PMM2 mutations can produce ARPKD-like phenotypes
Pathology & Pathogenesis
- Fibrocystin is a large transmembrane protein localized to the primary cilium and basal body, particularly in collecting duct and thick ascending limb epithelium, and in the bile duct
- Cysts are characteristically fusiform dilations of the collecting ducts, creating a radially striated appearance on imaging
- Invariably associated with congenital hepatic fibrosis (CHF) - periportal fibrosis causing portal hypertension
- Non-obstructive intrahepatic bile duct dilatation (Caroli disease) is variably present
Clinical Features
- Presents at birth or in infancy with massive bilateral renal enlargement (can be detected on prenatal ultrasound)
- Severely affected neonates have Potter sequence (oligohydramnios, pulmonary hypoplasia, limb contractures, characteristic facies) - often die from respiratory failure
- Surviving infants/children develop progressive CKD
- Portal hypertension, esophageal varices, and cholangitis dominate in older patients who survive the neonatal period
Management
- No disease-specific therapy exists
- Supportive: antihypertensives, treatment of portal hypertension, management of CKD
- Combined kidney-liver transplantation may be required in severe cases
Summary Comparison
| Feature | ADPKD | ARPKD |
|---|---|---|
| Inheritance | Autosomal dominant | Autosomal recessive |
| Gene(s) | PKD1 (chr 16), PKD2 (chr 4) | PKHD1 (chr 6) |
| Protein | Polycystin-1/2 | Fibrocystin |
| Onset | 4th-5th decade (usually) | Perinatal/infancy |
| Cyst origin | All nephron segments | Collecting ducts |
| Liver | Hepatic cysts | Congenital hepatic fibrosis |
| Prevalence | 1 in 400-1,000 | 1 in 20,000 |
| ESKD | ~58 yrs (PKD1), ~79 yrs (PKD2) | Childhood to early adulthood |
| Specific therapy | Tolvaptan (ADPKD) | None approved |
Sources: Brenner and Rector's The Kidney, 2-Volume Set; Smith and Tanagho's General Urology, 19th ed.; National Kidney Foundation Primer on Kidney Diseases, 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.