Investigation in wilson disease
Reading File
Finding Sources
Searching PubMed
Wilson disease diagnosis investigations
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching PubMed
Wilson disease diagnosis Leipzig score copper investigations
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive data to write a thorough answer. Let me compile everything.
Investigations in Wilson Disease
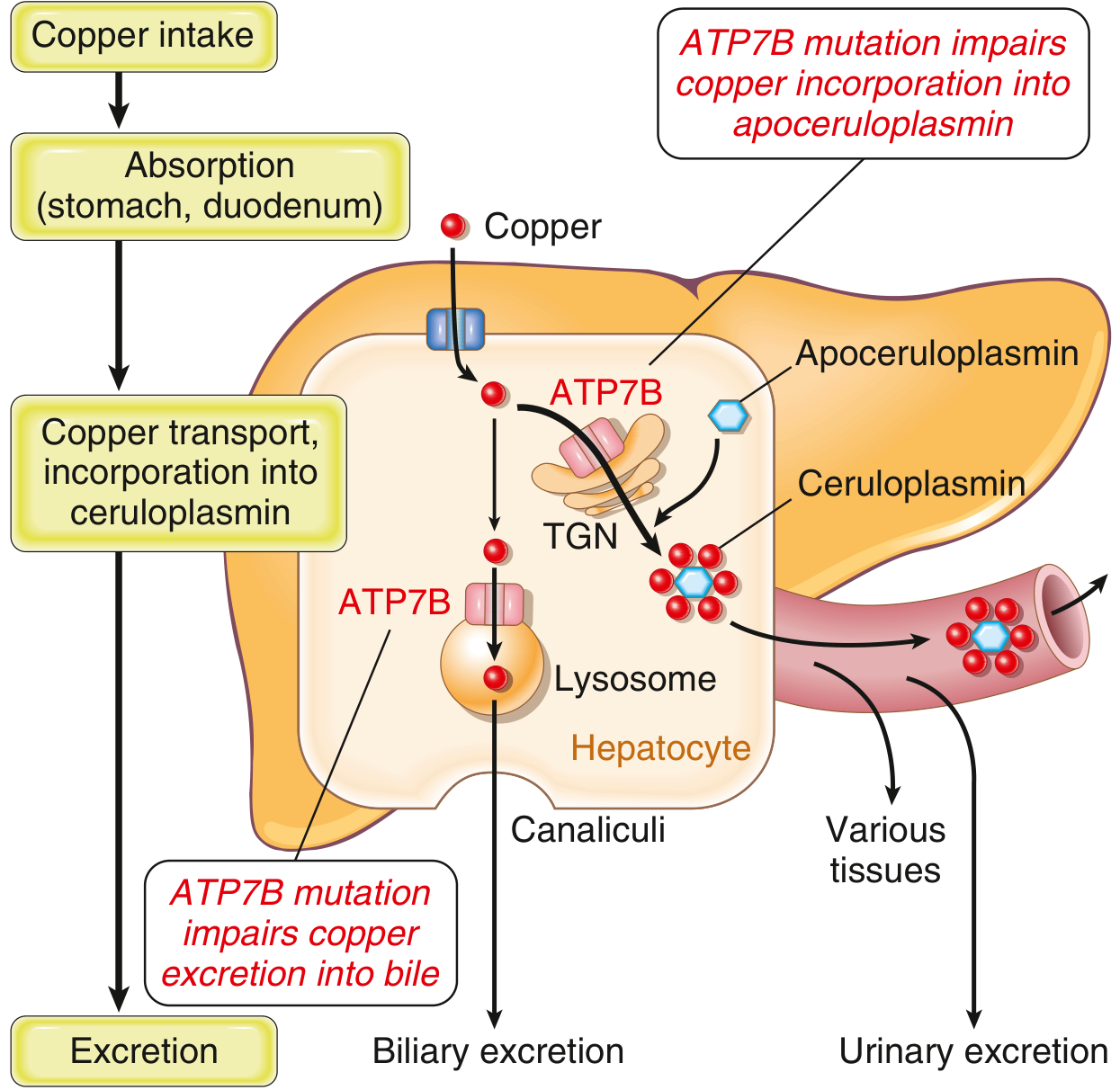
Wilson disease (WD) is an autosomal recessive disorder of copper transport caused by mutations in the ATP7B gene on chromosome 13. The ATP7B protein normally exports copper into bile and incorporates it into ceruloplasmin. When it fails, copper accumulates progressively in the liver, brain, kidneys, corneas, and other tissues.
1. Slit-Lamp Examination (Kayser-Fleischer Rings)
Kayser-Fleischer (KF) rings are golden-brown to greenish deposits of copper in the Descemet membrane at the corneal limbus. They are the most specific clinical finding in WD.
- Present in ~98% of patients with neurological WD and ~80% of all WD cases
- Present in only ~50% of patients with isolated hepatic WD - so absence does NOT exclude the diagnosis in liver-only presentations
- Absent KF ring + normal ceruloplasmin together virtually excludes WD in a patient with neurological/psychiatric symptoms
- Must be examined by slit lamp - cannot be reliably seen with the naked eye
"A KF ring is present in 98% of patients with neurological disease and in 80% of all cases of WD." - Bradley and Daroff's Neurology in Clinical Practice
2. Serum Ceruloplasmin
Ceruloplasmin is the major copper-carrying protein in blood. In WD, ATP7B failure means copper cannot be loaded onto apoceruloplasmin, so ceruloplasmin levels fall.
| Result | Interpretation |
|---|---|
| >0.2 g/L (>20 mg/dL) | Normal (0 points) |
| 0.1-0.2 g/L | Borderline low (1 point) |
| <0.1 g/L (<10 mg/dL) | Strongly suggestive (2 points) |
Caveats:
- Low ceruloplasmin is not specific - also seen in severe liver disease of any cause, nephrotic syndrome, protein-losing enteropathy, malnutrition
- Ceruloplasmin can be falsely normal or elevated in WD because it is an acute-phase reactant - pregnancy, infection, and inflammation can raise it
- For patients with liver dysfunction: ceruloplasmin is generally <20 mg/dL
3. 24-Hour Urinary Copper Excretion
This is one of the most useful tests. As copper spills from the injured liver into the bloodstream, renal copper excretion increases markedly.
| Result | Interpretation |
|---|---|
| Normal | <40-100 μg/24h |
| Suggestive of WD | >100 μg/24h (>1.6 μmol/24h) |
| 1-2x upper limit of normal | 1 point (Leipzig) |
| >2x upper limit of normal | 2 points (Leipzig) |
- In fulminant WD: urinary copper is markedly elevated
- False positives: any cholestatic liver disease can raise urine copper
- D-penicillamine challenge: in children, urine copper >25 μmol/24h after 500 mg D-penicillamine is given twice (total 1g over 12h) is suggestive (2 points in Leipzig score)
4. Serum Copper
- Total serum copper is usually low in WD (because ceruloplasmin-bound copper is reduced)
- However, in acute liver failure from WD, massive copper release from the necrotic liver causes serum copper to be strikingly elevated
- Non-ceruloplasmin-bound (free) copper is elevated in most WD patients and is a sensitive indicator, but not widely available in routine labs
5. Liver Biopsy with Quantitative Copper
Quantitative liver copper concentration is the gold standard test.
| Result | Interpretation |
|---|---|
| Normal | <50 μg/g dry weight (−1 point) |
| >Normal but <5x ULN | 1 point |
| >5x upper limit of normal (>250 μg/g dry weight) | 2 points - diagnostic |
Key points:
- Sample must be collected in a trace element-free container on a fresh specimen
- Histochemical stains (rhodanine, rubeanic acid) for copper may be negative even with massive accumulation, and may be positive in other cholestatic conditions - they should NOT be relied upon for diagnosis
- Histological features of WD range from steatosis and focal necrosis to chronic hepatitis with Mallory bodies, to cirrhosis
- Liver biopsy may be contraindicated in fulminant WD due to coagulopathy
"There is no correlation between histochemical staining of copper and quantitative copper measurements of liver biopsy samples in Wilson disease. Therefore, these histochemical stains should not be used to establish or exclude this diagnosis." - Yamada's Textbook of Gastroenterology
6. Special Serum Ratios (for Acute Liver Failure / Fulminant WD)
Two ratios help distinguish WD-related acute liver failure (ALF) from other causes:
| Ratio | Threshold | Significance |
|---|---|---|
| ALP : Total bilirubin | <4 | Strongly suggestive of WD-related ALF |
| AST : ALT | >2.2 | Strongly suggestive of WD-related ALF |
These are particularly useful because in WD-related ALF, ALP is characteristically low relative to bilirubin (unlike most other causes of ALF where ALP rises). KF rings may be absent in up to 50% of fulminant presentations.
7. Blood and Haematological Tests
- Coombs-negative (DAT-negative) haemolytic anaemia: in acute/fulminant WD, massive copper release from the necrotic liver causes direct erythrocyte lysis - this is a hallmark finding (1 point, Leipzig)
- Liver function tests: elevated transaminases, variable bilirubin (conjugated then unconjugated if haemolysis present), low albumin in advanced disease
- Serum uric acid: characteristically low in WD due to Fanconi-type renal tubular losses - a valuable clue
- Coagulation screen: PT/INR prolonged in severe hepatic involvement
- FBC: anaemia (haemolytic or from chronic disease), thrombocytopenia if hypersplenism/cirrhosis
8. Genetic Testing (ATP7B Mutation Analysis)
| Finding | Points (Leipzig) |
|---|---|
| Two pathogenic mutations (both chromosomes) | 4 points |
| One pathogenic mutation | 1 point |
| No pathogenic mutations | 0 points |
- Over 300 pathogenic mutations identified; most are small deletions or missense mutations
- Most common mutation: His1069Gln (up to 40% of cases in some ethnic populations)
- Absence of mutations does NOT exclude WD when clinical suspicion is high - testing is considered "uninformative" in that setting
- Most useful for family screening of first-degree relatives once a proband is identified
9. Neuroimaging (MRI Brain)
- MRI shows T2 hyperintensity in the basal ganglia (especially putamen), thalamus, midbrain, pons, cerebellum
- "Face of the giant panda" sign on axial MRI - hyperintensity in the tegmentum with preserved red nuclei and substantia nigra
- Cerebral and cerebellar atrophy is common
- Not diagnostic alone, but supports the diagnosis in neurological WD
10. The Leipzig Scoring System
This is the internationally used diagnostic algorithm synthesizing all test results. Scores >4 are diagnostic; ≤2 makes WD unlikely; score of 3 requires further testing.
| Parameter | Finding | Points |
|---|---|---|
| Kayser-Fleischer rings | Present | +2 |
| Absent | 0 | |
| Neurological symptoms | Severe | +2 |
| Mild | +1 | |
| Absent | 0 | |
| Ceruloplasmin | Normal >0.2 g/L | 0 |
| 0.1-0.2 g/L | +1 | |
| <0.1 g/L | +2 | |
| DAT-negative haemolytic anaemia | Present | +1 |
| Liver copper (no cholestasis) | >5x ULN | +2 |
| >Normal, <5x ULN | +1 | |
| Normal | -1 | |
| Positive copper stain (if no quantitative copper done) | +1 | |
| 24-hr urine copper (no acute hepatitis) | >2x ULN | +2 |
| 1-2x ULN | +1 | |
| Normal | 0 | |
| Positive penicillamine challenge | +2 | |
| ATP7B mutation analysis | Two pathogenic mutations | +4 |
| One pathogenic mutation | +1 | |
| No mutations | 0 |
Score interpretation:
- ≥4: Wilson disease diagnosis confirmed
- 3: Further testing required
- ≤2: Wilson disease unlikely
Summary: Investigation Approach by Presentation
| Presentation | First-line investigations |
|---|---|
| Any suspected WD | Slit-lamp for KF rings, serum ceruloplasmin, 24-hr urine copper, LFTs, FBC, serum uric acid |
| Neurological/Psychiatric | Above + MRI brain; absence of KF ring + normal ceruloplasmin nearly excludes WD |
| Hepatic (chronic) | Above + liver biopsy with quantitative copper if diagnosis uncertain |
| Acute liver failure | ALP:bilirubin ratio, AST:ALT ratio, serum copper (elevated), slit-lamp, urine copper |
| Family screening | ATP7B mutation analysis + ceruloplasmin + 24-hr urine copper + slit lamp |
Sources:
- Yamada's Textbook of Gastroenterology, 7th ed. (Chapter 94)
- Robbins & Kumar Basic Pathology
- Bradley and Daroff's Neurology in Clinical Practice
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.