Chicago classification for alchasia
Reading File
Finding Sources
Finding Sources
Searching the Web
Chicago classification v4.0 achalasia subtypes types I II III manometry
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a complete, well-sourced overview of the Chicago Classification for achalasia:
Chicago Classification of Achalasia (HRM-Based)
High-resolution manometry (HRM) is the gold standard for diagnosing achalasia. The Chicago Classification (CC) - first introduced by Pandolfino et al. in 2008 and currently at version 4.0 - uses two core parameters to classify achalasia:
- IRP (Integrated Relaxation Pressure): measures EGJ relaxation during swallowing. Abnormal = >15 mmHg (upper limit of normal).
- Peristalsis pattern: how the esophageal body responds to wet swallows.
A diagnosis of achalasia requires BOTH:
- Elevated median IRP (impaired EGJ relaxation)
- 100% absent/failed peristalsis (DCI <100 mmHg·s·cm for all swallows)
The Three Subtypes
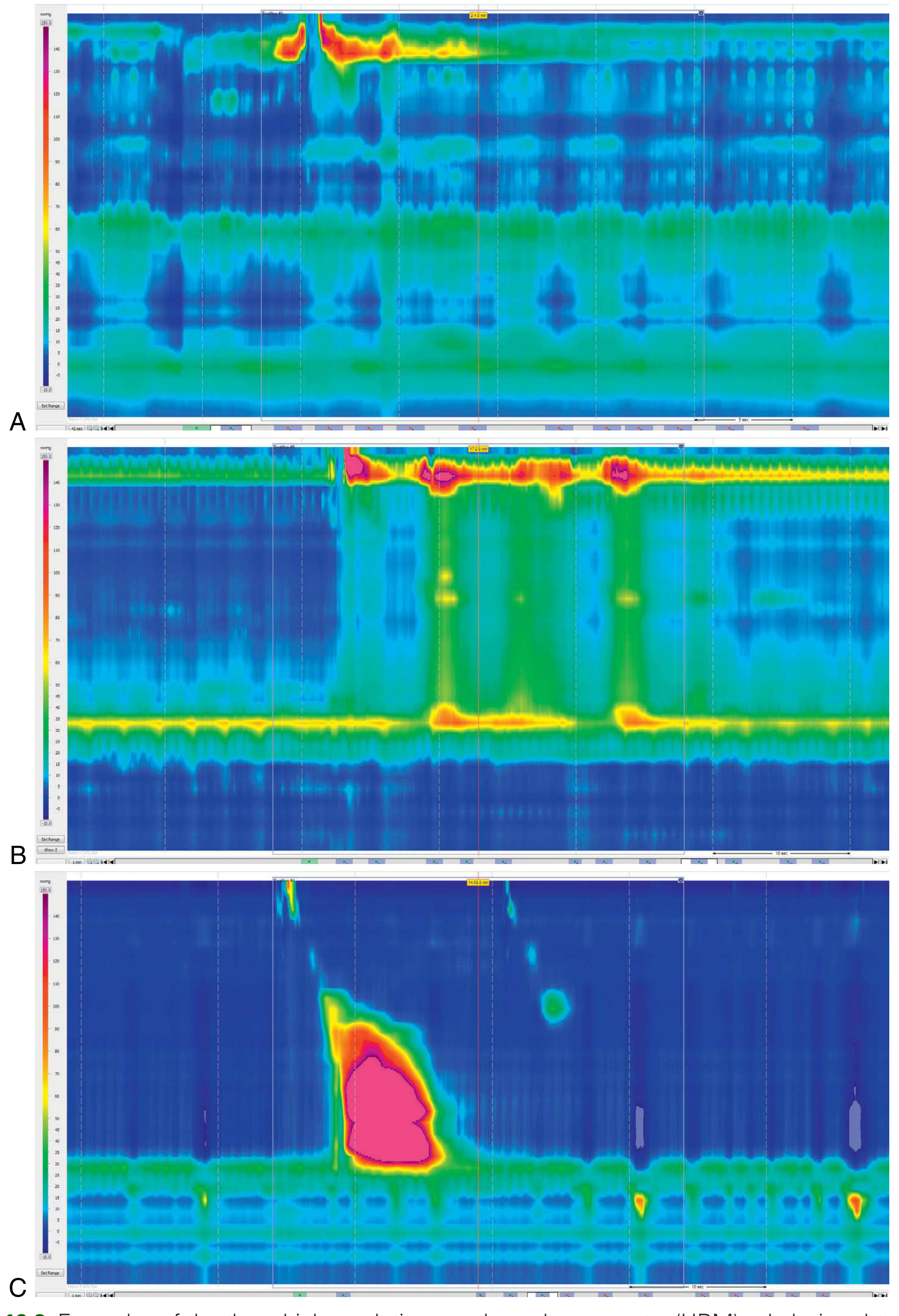
HRM pressure topography plots of the three achalasia subtypes - A: Type I (classic), B: Type II (with pressurization), C: Type III (spastic). - Clinical Gastrointestinal Endoscopy, Fig. 19.3
Type I - Classic Achalasia
| Feature | Detail |
|---|---|
| IRP | Elevated (>15 mmHg) |
| Esophageal body | 100% failed peristalsis - absent contractility, no pressurization |
| Pressurization | <20% of swallows show pan-esophageal pressurization |
| Appearance | Often dilated esophagus with negligible pressure in the body |
- The esophageal body is essentially silent - no contractions, no pressurization.
- Often associated with end-stage, dilated esophagus.
- Treatment response is moderate; more definitive sphincter disruption is required.
Type II - Achalasia with Panesophageal Pressurization
| Feature | Detail |
|---|---|
| IRP | Elevated (>15 mmHg) |
| Esophageal body | 100% failed peristalsis |
| Pressurization | ≥20% of swallows show rapid pan-esophageal pressurization (uniform pressure rise, isobaric) |
| Mechanism | Trapped fluid column is compressed as esophagus shortens |
- The most common subtype encountered clinically.
- Carries the best prognosis - treatment response rates of 95-96% with pneumatic dilation or Heller myotomy.
- The panesophageal pressurization is a passive, homogeneous pressure rise - not a true contraction.
Type III - Spastic (Vigorous) Achalasia
| Feature | Detail |
|---|---|
| IRP | Elevated (>15 mmHg) |
| Esophageal body | ≥20% of swallows show premature/spastic contractions (Distal Latency <4.5 seconds) |
| DCI | Normal or elevated in those spastic contractions |
| Peristalsis | No normal peristalsis; failed peristalsis ± pressurization may also be present |
- Characterized by rapidly propagated, lumen-obliterating contractions in the distal esophagus.
- Worst prognosis among the subtypes - treatment response is 29-70%.
- These patients do not respond well to interventions aimed solely at the LES; POEM (per-oral endoscopic myotomy) with a longer myotomy is often preferred.
Summary Table
| Subtype | IRP | Peristalsis | Key Feature | Treatment Response |
|---|---|---|---|---|
| Type I (Classic) | Elevated | 100% failed, no pressurization | Silent esophagus | Moderate |
| Type II (With pressurization) | Elevated | 100% failed | Pan-esophageal pressurization ≥20% swallows | Best (95-96%) |
| Type III (Spastic) | Elevated | ≥20% premature/spastic (DL <4.5s) | Rapid distal contractions | Worst (29-70%) |
Key Updates in Chicago Classification v4.0
The CCv4.0 (Yadlapati et al., 2021) made several refinements:
- Abnormal IRP can now be defined based on either supine OR upright position (not both required), if the protocol includes 10 wet swallows in the upright position.
- 100% absent peristalsis is strictly required - defined as all swallows having either failed peristalsis OR premature contraction.
- Inconclusive diagnoses are formally recognized - if appreciable peristalsis is seen in a different position, the diagnosis shifts toward inconclusive, requiring supportive testing (barium swallow, EndoFLIP, timed barium esophagram).
- EGJ Outflow Obstruction (EGJOO) with spastic features is now distinguished from Type III - if IRP is elevated with spasm but some peristalsis is preserved, it is classified as EGJOO with spastic features (a potential achalasia variant).
Clinical Relevance: Treatment Choice by Subtype
- All types: Pneumatic dilation, laparoscopic Heller myotomy (LHM), POEM
- Type II: Best outcomes with any modality
- Type III: POEM is preferred because its longer myotomy (extending into the esophageal body) addresses the spastic segment; LHM may be less effective
- Type I: Outcomes are reduced further as the degree of esophageal dilatation increases; esophagectomy may be needed in end-stage megaesophagus
Sources: Clinical Gastrointestinal Endoscopy, 3e, p. 308-309 | Sleisenger & Fordtran's GI and Liver Disease, p. 734-735 | Chicago Classification v4.0, Neurogastroenterol Motil 2021
This is a shared conversation. Sign in to Orris to start your own chat.