If a patient on ATT and pemphigus vulgaris presented with total HBcAb positive what does is signifies and how to approach HbsAg negative
Reading File
Finding Sources
Finding Sources
Searching PubMed
isolated anti-HBc immunosuppression reactivation
Searching PubMed
hepatitis B reactivation anti-tuberculosis therapy corticosteroids
Reading File
Reading File
Finding Sources
Searching PubMed
hepatitis B reactivation immunosuppression prophylaxis antiviral
Reading File
Reading Article
PMID: 39863345
Reading Article
PMID: 39206573
Reading Article
PMID: 34427860
Reading File
Reading File
Finding Sources
Loading Image
I now have all the information needed to provide a comprehensive answer. Here it is:
Total Anti-HBc Positive + HBsAg Negative in a Patient on ATT and Pemphigus Vulgaris
What Does "Total HBcAb Positive, HBsAg Negative" Mean?
This serologic pattern is called isolated anti-HBc (or resolved hepatitis B). Total anti-HBc (IgG + IgM) appears within 1-2 weeks of initial HBV infection and persists for life - it is acquired only through natural infection, never from vaccination. HBsAg negativity with anti-HBc positivity can represent three distinct situations:
| Scenario | Interpretation |
|---|---|
| Most common (~95%) | Past resolved HBV infection - patient was infected years ago and cleared the virus naturally |
| Window period | Acute HBV - HBsAg has cleared but anti-HBs not yet detectable (check IgM anti-HBc - would be positive) |
| Occult HBV infection | HBsAg below assay detection threshold, but HBV DNA may still be present in liver (low-level replication) |
| False positive | Rare; cross-reacting immunologic specificity |
Anti-HBc is only acquired during infection and will not be present in vaccinated individuals. - Harrison's Principles of Internal Medicine 22E, p. 2689
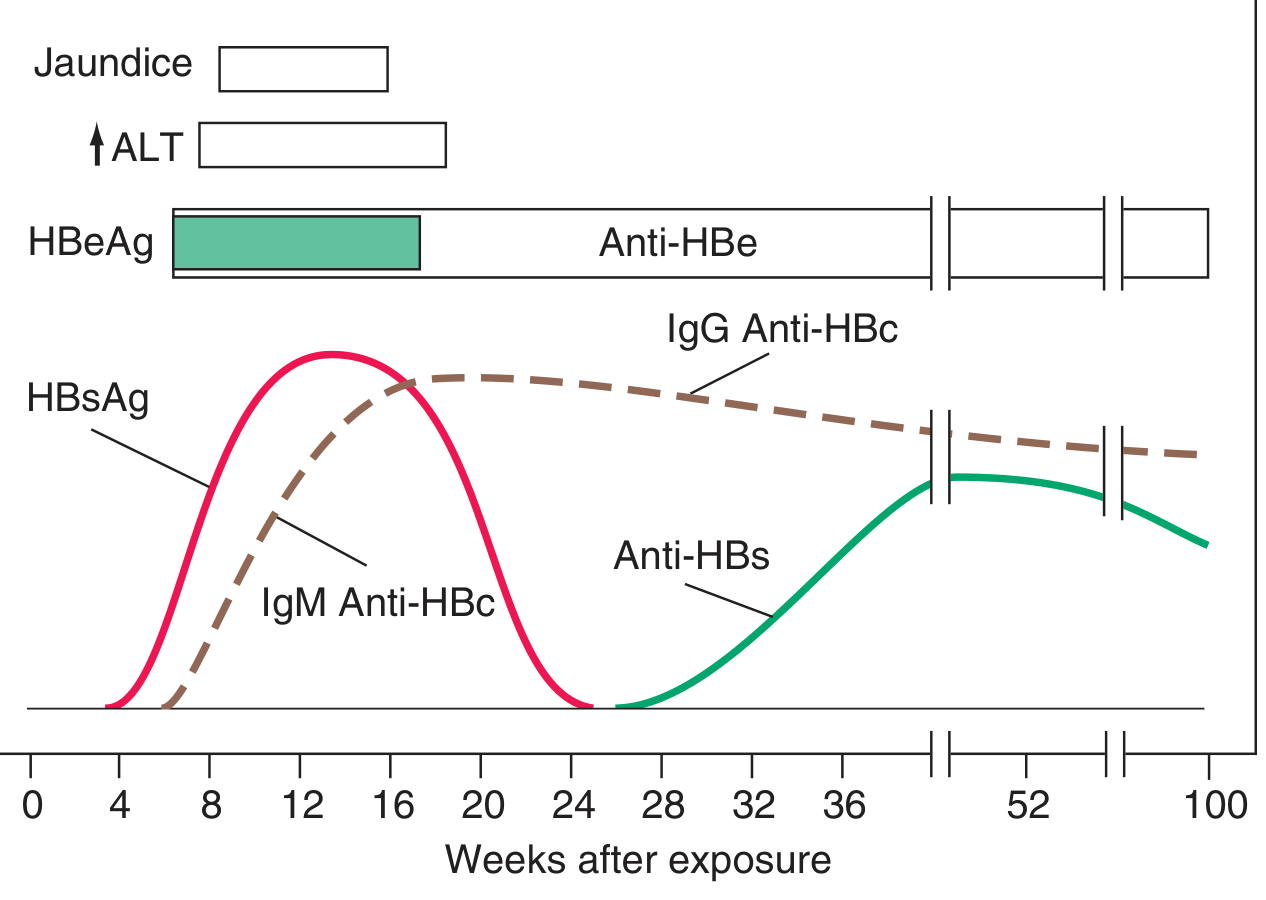
Scheme of typical serologic features of acute hepatitis B showing how IgG anti-HBc persists for life after HBsAg clears - Harrison's 22E
Why This Matters in Your Patient (ATT + Pemphigus Vulgaris)
This is a high-stakes triple problem:
- ATT - rifampicin, isoniazid, pyrazinamide are hepatotoxic on their own; HBV reactivation on ATT can cause fulminant hepatic failure
- Pemphigus vulgaris treatment - requires systemic immunosuppression (high-dose corticosteroids + azathioprine as first-line; or rituximab for refractory disease). Both drug classes are known to trigger HBV reactivation
- Occult HBV - even with HBsAg negative, residual HBV DNA in hepatocytes can re-emerge under immunosuppression
As noted in Goldman-Cecil Medicine, 2-Volume Set: "Some individuals who test positive for anti-HBc antibodies, but not for HBsAg or anti-HBs antibodies, may be viremic; in these cases, some viruses' amino acid substitutions in the HBsAg sequence make HBsAg undetectable... Other individuals may have such low-level HBV replication in their livers that HBV DNA is not detectable in blood ('occult' hepatitis B)."
Step-by-Step Clinical Approach
Step 1: Further Serologic Characterization
Order immediately:
| Test | Why |
|---|---|
| IgM anti-HBc | If positive = acute/recent infection (within 6 months); if negative = remote/resolved or occult |
| Anti-HBs (HBsAb) | If positive = fully resolved (immune); if negative with positive total anti-HBc = "isolated anti-HBc" pattern |
| HBV DNA (quantitative PCR) | The single most important test - determines if occult replication is present |
| HBeAg / Anti-HBe | For completeness |
| LFTs / ALT / AST | Baseline liver function, especially relevant with ATT hepatotoxicity risk |
Interpretation guide:
- HBsAg (-), Anti-HBs (+), Total anti-HBc (+) = Past resolved infection - lower but non-zero reactivation risk
- HBsAg (-), Anti-HBs (-), Total anti-HBc (+) = "Isolated anti-HBc" = highest risk group for occult HBV; requires HBV DNA testing urgently
- HBV DNA detectable = Occult HBV infection confirmed - treat as active infection from a prophylaxis standpoint
Step 2: Risk Stratification for HBV Reactivation
The risk depends on the immunosuppressive agents being used or planned:
| Agent | Reactivation risk (HBsAg-neg, anti-HBc-pos) |
|---|---|
| High-dose corticosteroids (>20 mg/day prednisone for >4 weeks) | Moderate |
| Rituximab (used in refractory pemphigus) | HIGH - highest risk of all agents |
| Azathioprine / mycophenolate | Low-moderate |
| Corticosteroids + azathioprine combined | Moderate |
| Corticosteroids + rituximab | Very high |
The 2025 AGA Clinical Practice Guideline (PMID: 39863345) stratifies management:
- High risk: Strong recommendation for antiviral prophylaxis
- Moderate risk: Conditional recommendation for antiviral prophylaxis
- Low risk: Monitoring alone acceptable
The 2024 meta-analysis (PMID: 39206573) of 8,034 HBsAg-neg/anti-HBc-pos patients found an overall HBV reactivation rate of 4% under immunosuppression - and prophylaxis was "strongly recommended" for rituximab-based regimens and "appropriate" for immune-mediated diseases like pemphigus.
Step 3: Management Algorithm
Total Anti-HBc (+), HBsAg (-)
↓
Check: HBV DNA + Anti-HBs + IgM anti-HBc + LFTs
↓
┌─────────────────────────────┐
│ HBV DNA detectable │ → Treat as occult HBV
│ (occult HBV confirmed) │ → Antiviral prophylaxis MANDATORY
└─────────────────────────────┘
↓
┌─────────────────────────────┐
│ HBV DNA undetectable │ → Risk stratify by
│ │ immunosuppressive regimen
└─────────────────────────────┘
↓
If rituximab planned: → Antiviral prophylaxis MANDATORY
If high-dose steroids only: → Consider prophylaxis (conditional)
If steroids + azathioprine: → Consider prophylaxis
Step 4: Antiviral Prophylaxis - Choice and Duration
If prophylaxis is indicated:
- Entecavir 0.5 mg/day - preferred (high barrier to resistance, potent)
- Tenofovir disoproxil fumarate (TDF) 245 mg/day or Tenofovir alafenamide (TAF) 25 mg/day - equally valid, TAF preferred if renal concerns
Goldman-Cecil Medicine: "HBV-infected patients who require corticosteroids, rituximab, or other chemotherapy for other conditions should receive entecavir 0.5 mg/day, tenofovir disoproxil fumarate 245 mg/day, or tenofovir alafenamide..."
Duration: Start 1-2 weeks before immunosuppression and continue for 6-12 months after stopping (longer for rituximab given prolonged B-cell depletion - typically 12 months post-rituximab). - APASL 2021 Guideline, PMID: 34427860
Step 5: ATT-Specific Considerations
- ATT drugs (especially pyrazinamide, rifampicin, isoniazid) are directly hepatotoxic
- Concurrent occult HBV reactivation during ATT can be misattributed to drug-induced liver injury (DILI), delaying the correct diagnosis
- Baseline and monthly LFTs are essential
- If ALT rises >3x ULN (symptomatic) or >5x ULN (asymptomatic) during ATT: suspect both ATT-DILI and HBV reactivation
- Check HBV DNA if LFTs rise during ATT, even if HBsAg was initially negative
Summary of Key Actions
- Subclassify the anti-HBc positive result: order HBV DNA + anti-HBs + IgM anti-HBc immediately
- If HBV DNA detectable: start antiviral prophylaxis (entecavir preferred) before continuing or escalating immunosuppression
- If HBV DNA undetectable but anti-HBs negative (isolated anti-HBc): risk stratify by planned therapy - if rituximab is planned, give prophylaxis; if steroids + azathioprine, consider prophylaxis
- If rituximab is needed for refractory pemphigus: antiviral prophylaxis is non-negotiable regardless of HBV DNA result
- Monitor LFTs monthly while on ATT - a rising ALT should trigger HBV DNA re-check to distinguish DILI from HBV reactivation
- Continue antivirals for 12 months after stopping rituximab (6 months after other immunosuppressants)
Key references:
- Harrison's Principles of Internal Medicine 22E, Chapter 350 - HBV serologic markers
- Goldman-Cecil Medicine - isolated anti-HBc and management in immunosuppressed patients
- Sleisenger and Fordtran's GI and Liver Disease - immunosuppressive therapy-induced HBV flares
- AGA Clinical Practice Guideline 2025 on HBV reactivation (PMID: 39863345)
- Meta-analysis: HBsAg-neg/anti-HBc-pos prophylaxis, 2024 (PMID: 39206573)
- APASL 2021 Guideline on HBV reactivation with immunosuppression (PMID: 34427860)
This is a shared conversation. Sign in to Orris to start your own chat.