Neonatal jaundice from ghai
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content needed. Let me compile a comprehensive, well-structured answer on neonatal jaundice as covered in standard pediatric textbooks (equivalent to Ghai's approach).
Neonatal Jaundice
Note: Ghai's Essential Pediatrics is not available in this library. The following is a comprehensive, standard-curriculum-level coverage drawn from Rosen's Emergency Medicine and The Harriet Lane Handbook (Johns Hopkins), which cover neonatal jaundice in the same depth and framework as Ghai.
Pathophysiology
Bilirubin is formed from the breakdown of heme-containing proteins, primarily hemoglobin. Unconjugated (indirect) bilirubin binds to albumin, is carried to the liver, and is conjugated by UDP-glucuronyl transferase, then excreted into bile.
Three physiologic factors contribute to neonatal jaundice:
- Increased bilirubin production (higher RBC mass, shorter RBC lifespan ~70–90 days vs 120 days in adults)
- Decreased hepatic clearance and excretion (immature glucuronyl transferase)
- Increased enterohepatic resorption (gut flora immature, beta-glucuronidase deconjugates bilirubin back)
Jaundice becomes visible clinically when total bilirubin rises above ~5 mg/dL. Nearly every newborn develops unconjugated bilirubin >1 mg/dL (the adult upper limit) during the first week of life.
Classification
Unconjugated (Indirect) Hyperbilirubinemia
| Category | Cause |
|---|---|
| Benign/physiologic | Physiologic jaundice, breast milk jaundice |
| Hemolytic | ABO incompatibility, Rh incompatibility, G6PD deficiency, spherocytosis, elliptocytosis, sickle cell, thalassemia, pyruvate kinase deficiency |
| Birth trauma | Cephalhematoma reabsorption, IVH/ICH |
| Infectious | TORCHS, UTI, sepsis |
| Obstructive (enterohepatic) | Meconium ileus, Hirschsprung, pyloric stenosis, duodenal atresia |
| Metabolic/genetic | Galactosemia, hypothyroidism, Crigler-Najjar syndrome, Gilbert syndrome |
| Miscellaneous | Dehydration, polycythemia, drugs, hypoalbuminemia, panhypopituitarism |
Conjugated (Direct) Hyperbilirubinemia
Always pathologic. Direct bilirubin >2.0 mg/dL and >10% of total serum bilirubin.
| Category | Cause |
|---|---|
| Biliary obstruction | Biliary atresia, choledochal cyst, inspissated bile syndrome, Alagille syndrome |
| Infectious | CMV, hepatitis B, HSV, rubella, toxoplasmosis, gram-negative sepsis, UTI |
| Metabolic/genetic | α1-antitrypsin deficiency, galactosemia, tyrosinemia, glycogen storage disease, cystic fibrosis, Dubin-Johnson/Rotor syndrome, Niemann-Pick, Gaucher, Wilson disease |
| Chromosomal | Trisomy 18, trisomy 21, Turner syndrome |
| Drugs/toxins | Parenteral nutrition, acetaminophen, erythromycin |
Types in Detail
1. Physiologic Jaundice
- Occurs in ~50% of normal newborns
- Due to immature bilirubin metabolism
- Appears after 24 hours of life
- TSB peaks at 6–8 mg/dL on days 2–4 in term infants (up to 12 mg/dL in some)
- Resolves by 2 weeks in term infants (up to 3 weeks in preterm)
- During first 3–4 days: TSB increases to 6.5 ± 2.5 mg/dL; max normal rise rate = 5 mg/dL/24 h or 0.2 mg/dL/h
2. Breast Milk Jaundice
- Second most common cause of neonatal jaundice
- Pathophysiology uncertain — possibly hormonally mediated or increased enterohepatic resorption
- Peaks later (~10–21 days), may persist 3–10 weeks
- Mild unconjugated hyperbilirubinemia; infant otherwise well
- Treatment: temporary cessation of breastfeeding confirms diagnosis; usually not necessary
3. Pathologic Jaundice — Red Flags
Any jaundice is pathologic if:
- Appears within 24 hours of birth
- TSB rises >5 mg/dL/24 hr
- TSB exceeds exchange transfusion threshold
- Persists beyond 3 weeks of age
- Associated with direct/conjugated hyperbilirubinemia
- Infant appears sick
Risk Factors for Severe Hyperbilirubinemia
- Birth weight <2500 g / prematurity
- Exclusive breastfeeding
- ABO or Rh incompatibility
- Cephalhematoma or significant bruising
- Predischarge TSB in high-risk zone
- G6PD deficiency
- Previous sibling requiring phototherapy
- Low albumin, sepsis, acidosis
- Infant of diabetic mother
Neurotoxicity: BIND and Kernicterus
Unconjugated bilirubin crosses the blood-brain barrier, causing neuronal death. At levels >20–25 mg/dL, risk of bilirubin-induced neurologic dysfunction (BIND) increases.
Acute Bilirubin Encephalopathy (ABE)
Early (potentially reversible):
- Somnolence, poor feeding, hypotonia/hypertonia, high-pitched cry
Late (may be irreversible):
- Lethargy, hypertonia, retrocollis, opisthotonos, fever, irritability, apnea → seizures → death
Kernicterus
Chronic, irreversible sequelae: cerebral palsy, sensorineural hearing loss, upward gaze palsy, intellectual disability.
Evaluation
| Test | Indication |
|---|---|
| Transcutaneous bilirubinometry | Quick screen in well infants >24h and <7 days old |
| Total + fractionated serum bilirubin | Confirmation and type (conjugated vs unconjugated) |
| CBC + peripheral smear | Hemolysis, infection |
| Direct Coombs test | Isoimmune hemolysis (ABO/Rh) |
| Blood group (mother + infant) | ABO/Rh incompatibility |
| Reticulocyte count | Hemolysis |
| G6PD assay | If risk factors present |
| Blood glucose, electrolytes, urine reducing substances, ammonia, lactate | Ill-appearing infant (IEM workup) |
| Urine culture | Conjugated jaundice — exclude UTI |
| Liver ultrasound | Conjugated jaundice — biliary atresia |
Indications for evaluation of a jaundiced infant (Box 166.1):
- Jaundice within first 24 hours
- Elevated direct bilirubin
- Rapidly rising TSB unexplained by history
- TSB approaching exchange level or not responding to phototherapy
- Jaundice persisting beyond 3 weeks
- Sick-appearing infant
Management
General Principle
Goal: prevent BIND and kernicterus. Encourage feeding (including breastfeeding) — stimulates gut motility, reduces enterohepatic recirculation.
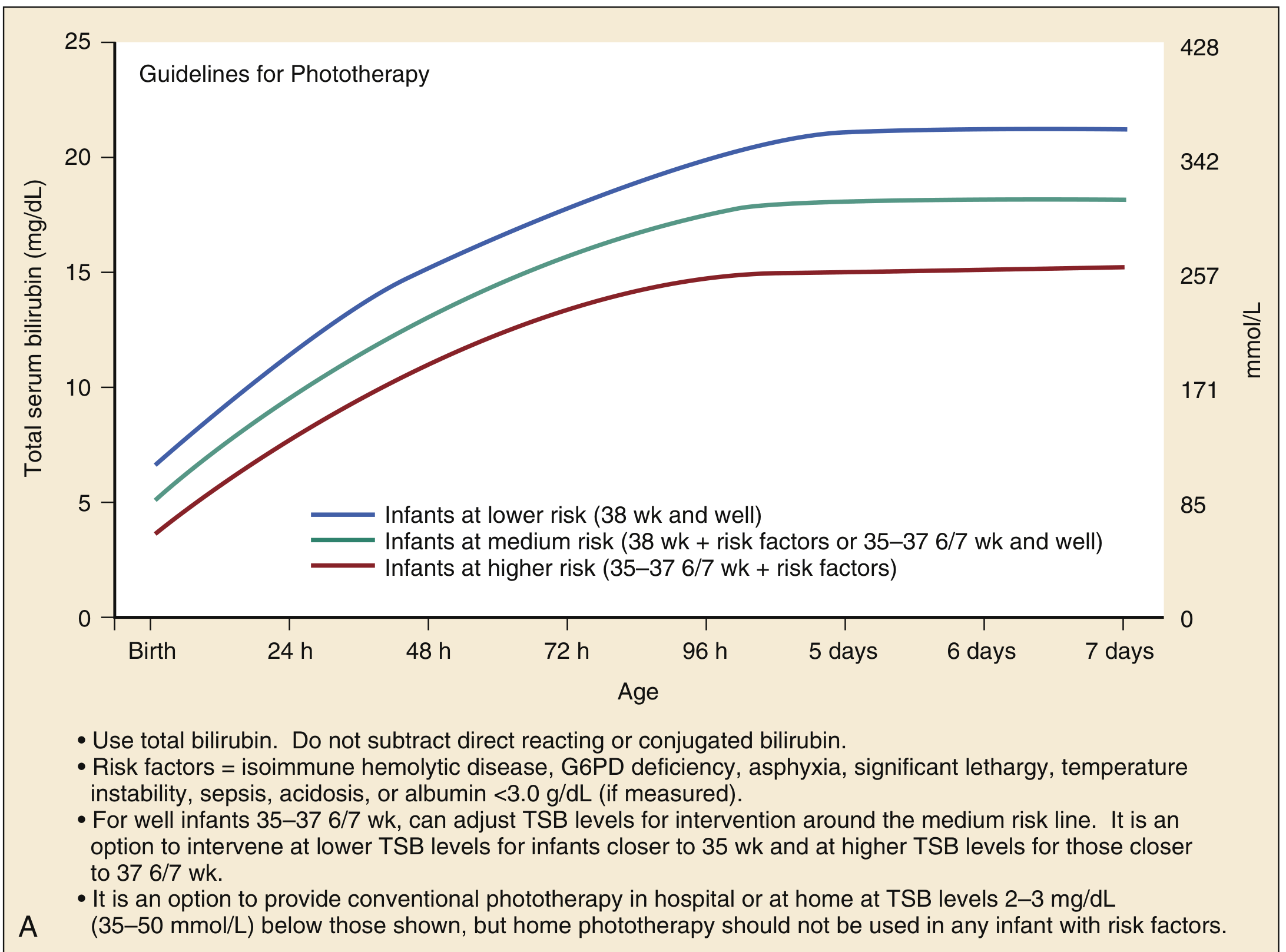
Phototherapy
Mechanism: Blue-spectrum light (wavelength ~460 nm) converts unconjugated bilirubin in the skin to water-soluble photoisomers (lumirubin) excreted in bile/urine without conjugation.
Intensive phototherapy should achieve a TSB decline of 1–2 mg/dL within 4–6 hours.
Guidelines for term infants (≥35 weeks) — AAP:
Guidelines for preterm infants (<35 weeks, Harriet Lane):
| Gestational Age | Phototherapy Threshold | Consider Exchange Transfusion |
|---|---|---|
| <28 weeks | 5–6 mg/dL | 11–14 mg/dL |
| 28–29 6/7 weeks | 6–8 mg/dL | 12–14 mg/dL |
| 30–31 6/7 weeks | 8–10 mg/dL | 13–16 mg/dL |
| 32–33 6/7 weeks | 10–12 mg/dL | 15–18 mg/dL |
Risk factors that lower threshold: isoimmune hemolytic disease, G6PD deficiency, asphyxia, significant lethargy, temperature instability, sepsis, acidosis, albumin <3.0 g/dL.
Exchange Transfusion (Double-Volume)
Used when phototherapy fails or TSB reaches dangerous levels.
Indications:
- TSB continues to rise or remains above exchange threshold despite intensive phototherapy
- Signs of acute bilirubin encephalopathy (hypertonia, retrocollis, opisthotonos, fever, high-pitched cry) — immediate exchange transfusion
- TSB ≥5 mg/dL above the exchange line
Guidelines for ≥35 weeks gestation:
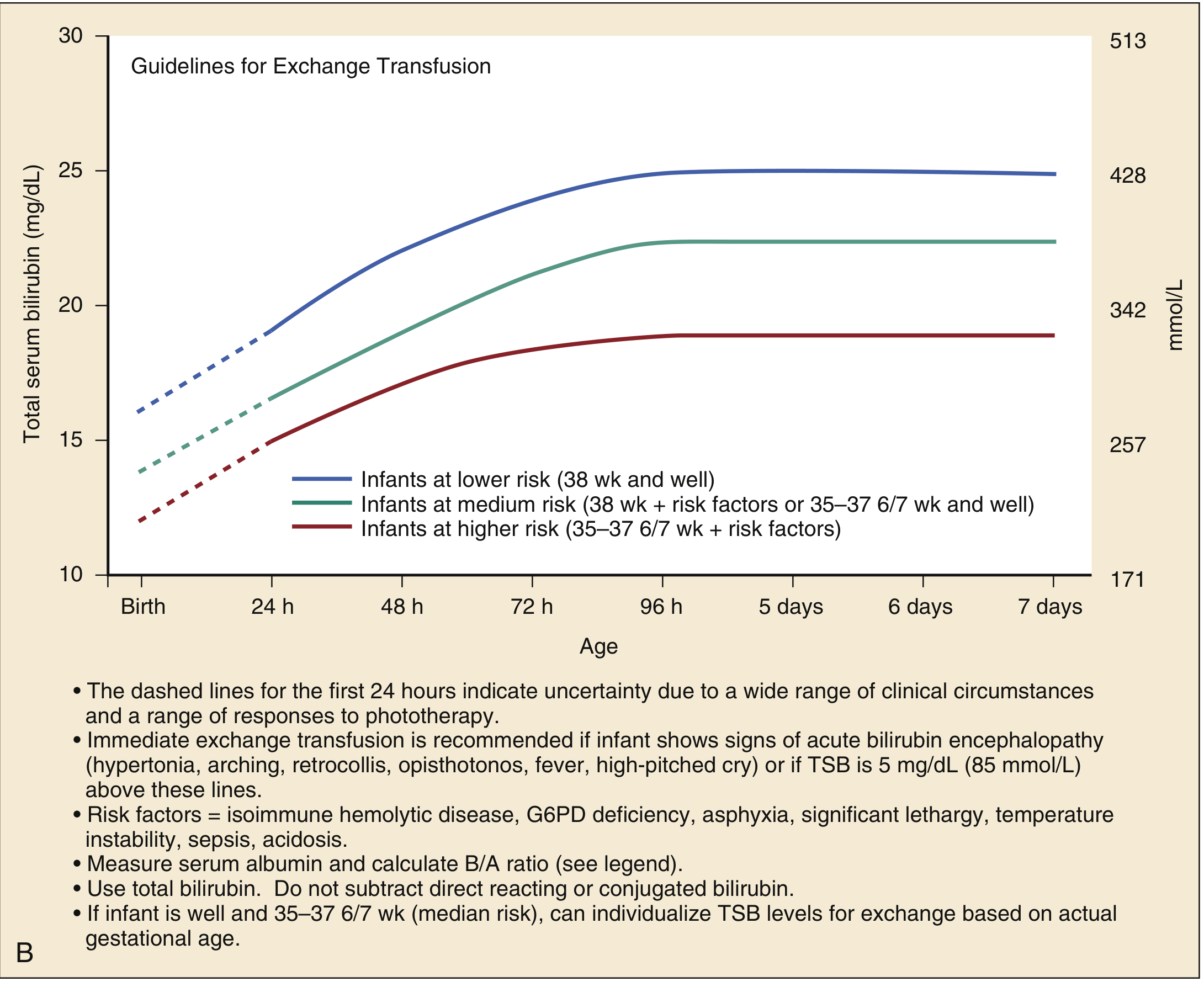
Procedure: Double-volume exchange (160–200 mL/kg) removes ~85% of sensitized RBCs and bilirubin-laden blood, replacing it with donor blood.
IVIG (for Isoimmune Hemolytic Disease)
- Dose: 0.5–1 g/kg IV over 2 hours
- Indicated if TSB is rising despite intensive phototherapy, or TSB is within 2–3 mg/dL of exchange transfusion threshold
Conjugated Hyperbilirubinemia Management
- Depends on underlying etiology
- Ursodiol for infants on full feeds
- Fat-soluble vitamin supplementation (A, D, E, K)
- Phototherapy is not contraindicated but risk of "bronze baby" syndrome (transient dark gray-brown discoloration of skin, serum, urine) must be weighed
- Biliary atresia: surgical referral (Kasai portoenterostomy) — time-sensitive
Summary Table: Physiologic vs Pathologic Jaundice
| Feature | Physiologic | Pathologic |
|---|---|---|
| Onset | After 24 hours | Within 24 hours |
| Peak TSB (term) | ≤12 mg/dL | >12 mg/dL |
| Rise rate | <5 mg/dL/day | >5 mg/dL/day |
| Duration | <2 weeks (term) | >3 weeks |
| Bilirubin type | Unconjugated | May be conjugated |
| General condition | Well infant | May be sick |
Sources: Rosen's Emergency Medicine, 9th Ed., Ch. 166; The Harriet Lane Handbook, 23rd Ed., Ch. 18 — Harriet Lane Handbook (Johns Hopkins)
This is a shared conversation. Sign in to Orris to start your own chat.