Define pulmonary edema
Reading File
Finding Sources
Searching the Web
pulmonary edema definition pathophysiology
Reading File
Reading File
Reading File
Reading File
Loading Image
Pulmonary Edema
Definition: Pulmonary edema is the abnormal accumulation of excess fluid in the interstitial spaces and alveoli of the lungs, resulting from a rate of fluid filtration out of the pulmonary capillaries that exceeds the capacity of the lymphatic drainage system. The result is heavy, wet lungs with impaired gas exchange.
Pathophysiology
The same Starling forces that govern edema elsewhere in the body apply in the lung. Fluid moves out of pulmonary capillaries when:
- Hydrostatic pressure rises (pushes fluid out)
- Oncotic pressure falls (less force retaining fluid in vessels)
- Capillary/alveolar membrane permeability increases (barrier disrupted)
- Lymphatic drainage is obstructed or overwhelmed
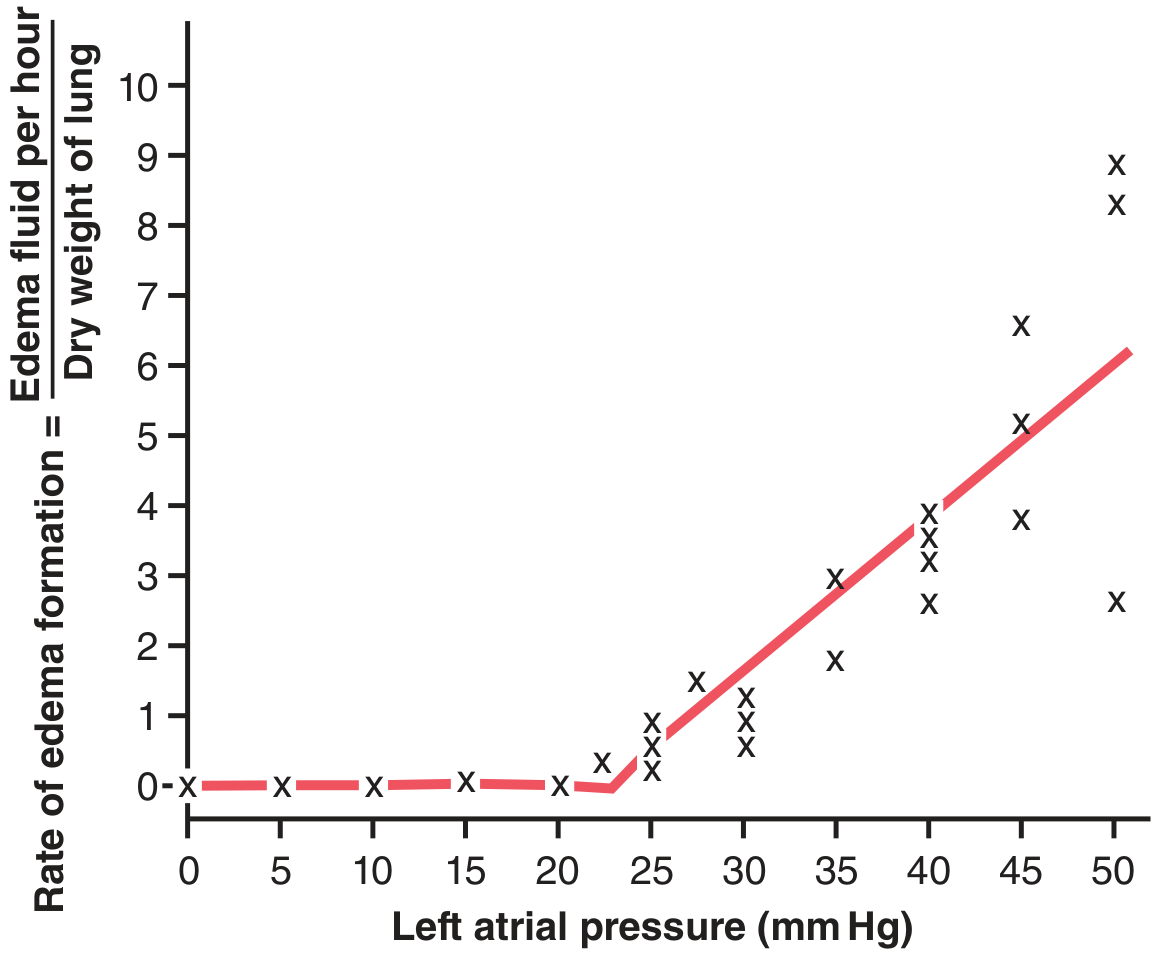
Safety factor: Under normal conditions, pulmonary capillary pressure (~7 mm Hg) is well below plasma colloid osmotic pressure (~28 mm Hg). Significant edema does not form until capillary pressure exceeds the colloid osmotic pressure — an acute safety margin of ~21 mm Hg. In chronic conditions (e.g., mitral stenosis), lymphatic hypertrophy can expand this tolerance; patients have survived with capillary pressures of 40–45 mm Hg without lethal edema.
When capillary pressure rises 25–30 mm Hg above the safety factor, lethal pulmonary edema can develop within 20–30 minutes. — Guyton & Hall, Medical Physiology
Classification
Pulmonary edema is broadly divided into two major categories (Robbins Pathologic Basis of Disease):
1. Cardiogenic (Hemodynamic) Pulmonary Edema
Caused by increased hydrostatic pressure, most commonly from left-sided heart failure. Fluid initially collects in the dependent (basal) lung regions.
Causes include:
- Left-sided heart failure / systolic or diastolic LV dysfunction
- Mitral stenosis or regurgitation
- Volume overload
- Pulmonary vein obstruction
Histology: Engorged alveolar capillaries, intra-alveolar transudate (finely granular pale pink material), alveolar microhemorrhages, and hemosiderin-laden macrophages ("heart failure cells"). Chronic cases show brown induration (fibrosis + hemosiderin deposition).
2. Noncardiogenic Pulmonary Edema
Caused by increased capillary permeability from alveolar-capillary membrane injury, producing a protein-rich exudate rather than a transudate.
Causes of direct injury:
- Bacterial/viral pneumonia
- Inhaled toxins (chlorine, sulfur dioxide, smoke, high O₂)
- Gastric aspiration, near-drowning
- Radiation, lung trauma
Causes of indirect (systemic) injury:
- Sepsis, burns, pancreatitis, extensive trauma (SIRS)
- Transfusion-related (TRALI)
- Drugs: bleomycin, methadone, heroin, cocaine, amphotericin B
Special categories:
- High-altitude pulmonary edema (HAPE)
- Neurogenic pulmonary edema (CNS trauma)
When severe, noncardiogenic pulmonary edema is the hallmark of Acute Respiratory Distress Syndrome (ARDS).
Additional Etiologic Factors (Less Common)
| Mechanism | Example |
|---|---|
| Decreased oncotic pressure | Hypoalbuminemia, nephrotic syndrome, liver disease |
| Lymphatic obstruction | Lymphangitic carcinoma |
| Multifactorial (CKD/ESRD) | Fluid overload + uremic permeability + hypoalbuminemia |
Key Clinical Consequence
Fluid flooding the alveoli prevents effective gas exchange → hypoxemia → respiratory distress. The condition can progress rapidly to respiratory failure, particularly in the acute setting.
Sources: Guyton & Hall Textbook of Medical Physiology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.