Hi
Hey! How can I help you today?
Where I can get your app
I'm Orris, an AI assistant - I don't have a standalone app of my own. I run as a conversational AI within whatever platform or interface you're currently using to chat with me.
If you're looking for a general AI assistant app, some popular options include:
- ChatGPT - available at chat.openai.com or on iOS/Android
- Claude - available at claude.ai or on iOS/Android
- Gemini - available at gemini.google.com or on iOS/Android
- Copilot - available at copilot.microsoft.com
Is there something specific you're trying to do? I'm happy to help you right here!
Can you explain me about labor topic for medical student with deep concept note and image
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Load note about labor where it is gone?
It looks like the note got cut off in the previous response — I compiled everything but the final message didn't render the full content. Here it is now in full:
🏥 LABOR - Deep Concept Note for Medical Students
Sources: Guyton & Hall Medical Physiology | Textbook of Family Medicine 9e | Morgan & Mikhail's Clinical Anesthesiology | Tintinalli's Emergency Medicine | Roberts & Hedges' Clinical Procedures
1. DEFINITION
Labor is defined as the presence of sufficient uterine contractions in frequency, intensity, and duration to bring about effacement and dilation of the cervix, ultimately resulting in delivery of the fetus, placenta, and membranes.
- Normally commences at 40 ± 2 weeks after the last menstrual period
- Over 95% of births are cephalic (head-first) presentations
- Buttocks-first = breech presentation
2. PHYSIOLOGY - INITIATION OF LABOR
Understanding WHY labor starts is a high-yield concept. Multiple factors converge:
A. Hormonal Factors
| Factor | Role |
|---|---|
| Estrogen | Increases uterine contractility; increases gap junctions between myometrial cells; increases oxytocin receptor expression |
| Progesterone | Inhibits contractility during pregnancy - acts as a "uterine quiescent agent" |
| Estrogen:Progesterone ratio | Rises near term (estrogen keeps rising, progesterone plateaus or falls slightly) - this shift increases myometrial sensitivity |
| Oxytocin | Released from the neurohypophysis; myometrial oxytocin receptors increase dramatically near term |
| Prostaglandins (PGE2, PGF2α) | Released by fetal membranes and decidual tissue; powerful stimulants of uterine contraction |
| Fetal cortisol | Adrenal glands of the fetus secrete cortisol, which is a uterine stimulant |
Key concept: Circulating oxytocin levels do NOT always rise at the onset of labor - but the NUMBER of myometrial oxytocin receptors rapidly increases, making the uterus more sensitive.
B. Mechanical Factors
- Uterine stretch - As the fetus grows, stretching smooth muscle increases contractility. Twins are born ~19 days earlier than singletons, proving stretch plays a role
- Cervical stretch/irritation - Stretching the cervix triggers reflex oxytocin release (the Ferguson reflex) and myogenic signal transmission to the uterine body
- Rupture of membranes causes direct head pressure on the cervix, amplifying this effect
3. PRODROMAL (PRE-LABOR) EVENTS
These occur 2-4 weeks before true labor:
- Lightening - The fetal presenting part settles into the pelvis; the fundal height drops; the woman notices reduced upper abdominal pressure but increased pelvic pressure
- Braxton Hicks contractions - Sporadic, irregular contractions that are characteristically irregular in frequency, duration, and intensity ("false labor"). They help with cervical effacement
- Cervical effacement - Cervix softens, thins, and moves anteriorly
- Bloody show - Cervical mucous plug (often blood-tinged) is expelled. Most women enter true labor within 3 days of bloody show
Bloody show vs. pathological bleeding: Bloody show is mucoid and lightly blood-tinged. Heavy bleeding (like the start of a menstrual period) is pathological - consider placenta previa or abruptio placentae.
4. TRUE vs. FALSE LABOR
| Feature | True Labor | False Labor (Braxton Hicks) |
|---|---|---|
| Contraction regularity | Regular, increasing frequency | Irregular |
| Contraction intensity | Progressive increase (25-60 mmHg) | Variable, no progression |
| Effect on cervix | Progressive dilation & effacement | No change |
| Pain location | Back + abdomen | Mostly lower abdomen |
| Response to walking | Increases with activity | May diminish with rest |
5. STAGES OF LABOR
Overview Table
| Stage | Onset | Completion |
|---|---|---|
| First (latent + active phases) | Active labor begins | Complete cervical dilation (10 cm) |
| Second | Complete dilation | Delivery of baby |
| Third | Delivery of baby | Delivery of placenta |
| Fourth* | Delivery of placenta | Uterine contraction/hemostasis |
*Not always formally counted as a stage
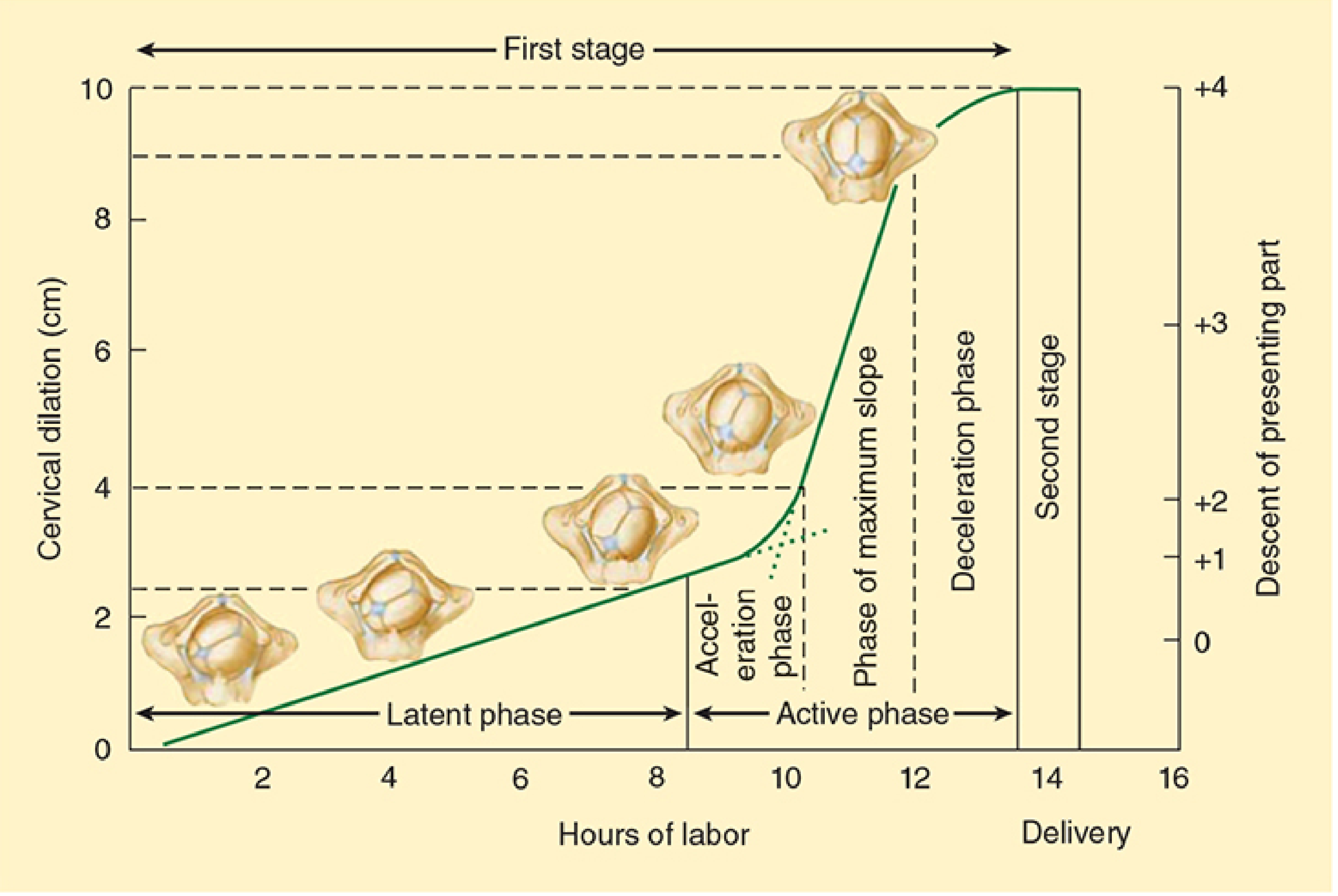
FIRST STAGE - Cervical Dilation
This is the longest stage. It is subdivided into:
Latent Phase
- Onset of regular contractions to ~4 cm dilation
- Slow cervical dilation but major effacement occurs
- Duration: up to 20 hours in nulliparas, 14 hours in multiparas
- Contractions: irregular at first, becoming more regular
- Best managed at home with clear liquids
Active Phase
- From ~4 cm to full dilation (10 cm)
- Expected dilation rate:
- Nulliparas: ≥1.2 cm/hr
- Multiparas: ≥1.5 cm/hr
- Contractions: every 3-5 minutes, lasting ~1 minute, intensity ~40 mmHg
- Progress depends on: uterine contraction strength, fetal head size/position, and pelvic dimensions (the 3 Ps: Powers, Passenger, Passage)
Active phase sub-phases (Friedman curve):
- Acceleration phase
- Phase of maximum slope
- Deceleration phase
First Stage Duration:
- Nulliparas: 8-12 hours
- Multiparas: 5-8 hours
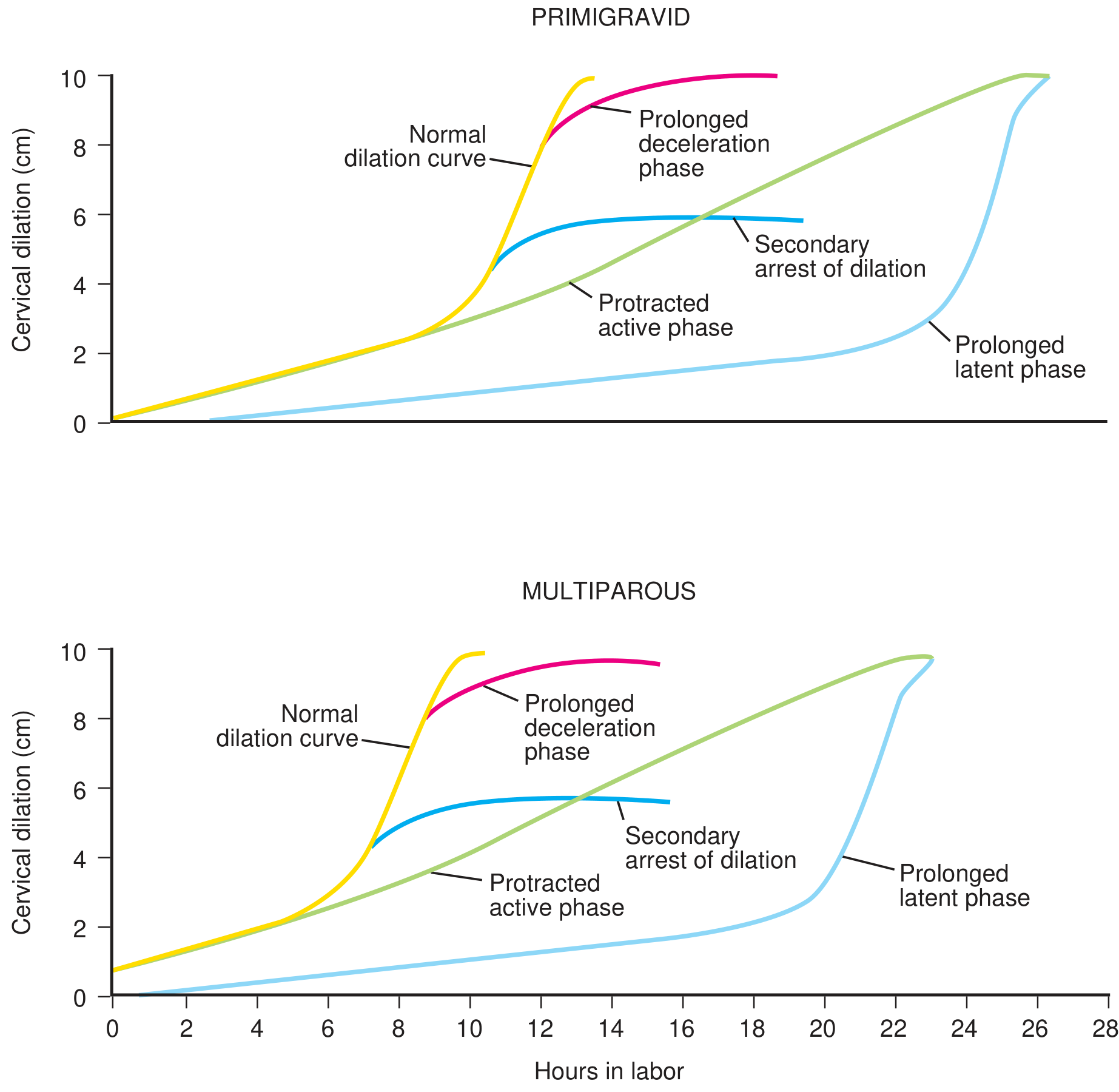
LABOR PROGRESS CURVES
SECOND STAGE - Expulsion of the Fetus
- From complete dilation to delivery of the baby
- Contractions: every 1.5-2 minutes, lasting 1-1.5 minutes
- The patient actively bears down (pushes), greatly augmenting intrauterine pressure
- Duration:
- Multiparas: ~20 minutes (up to 120 min)
- Nulliparas: ~50 minutes (up to 120 min without epidural, 3 hours with epidural)
THIRD STAGE - Placental Delivery
- From delivery of the baby to delivery of the placenta
- Duration: 15-30 minutes (up to 45 min)
- Uterus continues contracting, shearing the placenta from its implantation site
- Signs of placental separation: gush of blood, cord lengthening, uterus rises and becomes globular
- Average blood loss: ~350 mL
How bleeding is controlled after placental delivery:
- Uterine smooth muscle fibers are arranged in figure-of-eight patterns around blood vessels
- Uterine contraction mechanically constricts the vessels (living ligature mechanism)
- Vasospasm from local prostaglandins and other mediators
6. MECHANICS OF PARTURITION - UTERINE CONTRACTIONS
- Contractions begin at the uterine fundus and spread downward
- Strongest at the top and body; weakest at the lower uterine segment near the cervix
- This polarity means each contraction pushes the fetus toward and through the cervix
- Early labor: contractions every 30 minutes
- Late labor: contractions every 1-3 minutes
- Combined uterine + abdominal force: approximately 25 pounds per contraction
Warning: Strong uterine contractions impede blood flow through the placenta. Continuous contractions (e.g., from oxytocin overuse causing uterine spasm) can cause fetal death from hypoxia. This is why intermittent contractions are physiologically protective.
7. CARDINAL MOVEMENTS OF LABOR (Vertex/Cephalic Presentation)
The fetus follows the path of least resistance, adapting its smallest diameter to the most favorable dimension of the birth canal at each level of the pelvis.
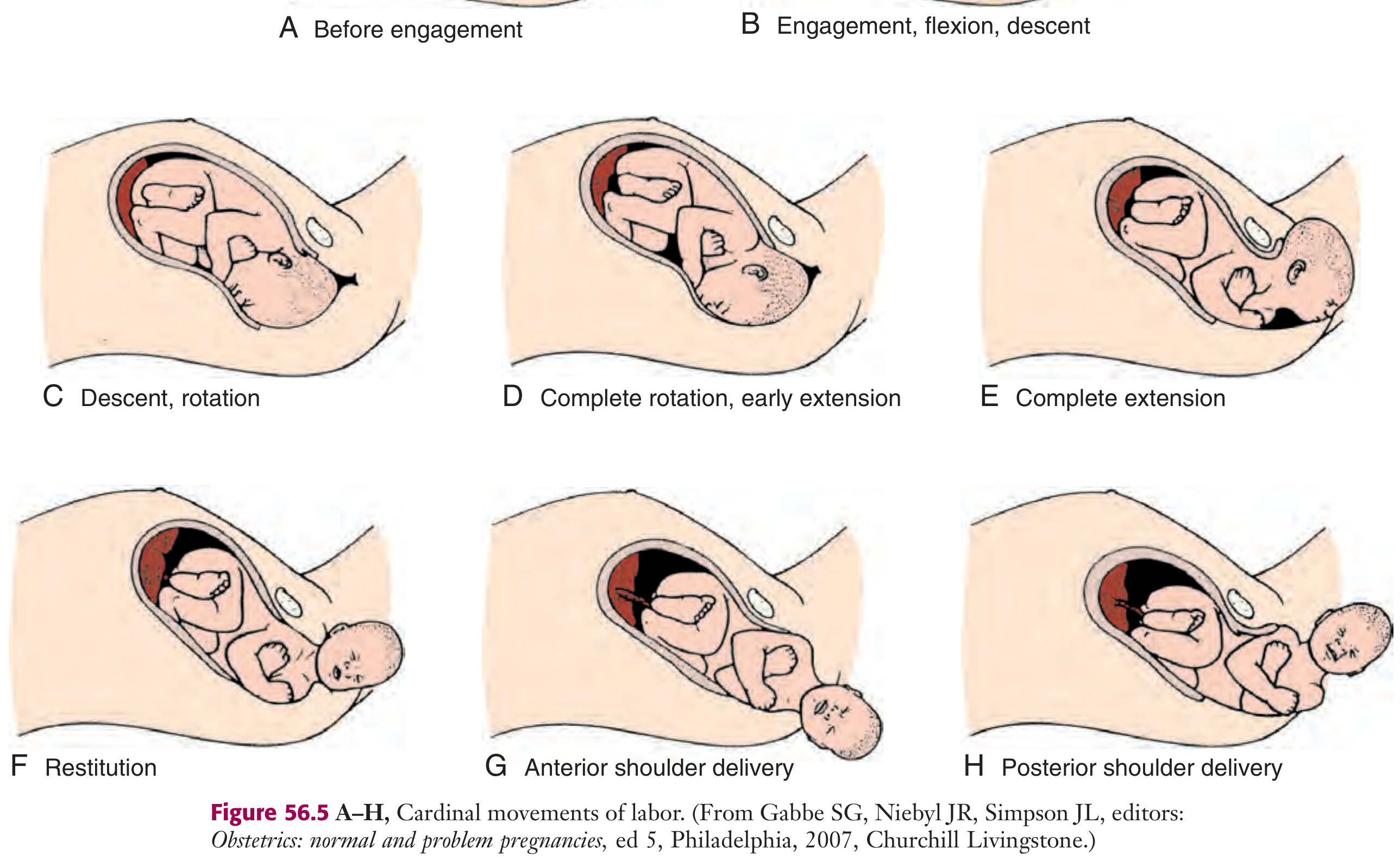
The 7 Cardinal Movements:
| # | Movement | Description |
|---|---|---|
| 1 | Engagement | Biparietal diameter (BPD) passes through the pelvic inlet. Presenting part at 0 station. Occurs in last 2 weeks in nulliparas; at onset of labor in multiparas |
| 2 | Flexion | Head flexes to minimize presenting diameter (suboccipitobregmatic replaces occipitofrontal). Occurs passively |
| 3 | Descent | Downward passage of the presenting part. Gradual and progressive - driven by uterine + abdominal contractions |
| 4 | Internal rotation | Occiput rotates from transverse toward anterior (toward symphysis pubis) = occiput anterior (OA). Less commonly rotates posteriorly = occiput posterior (OP) |
| 5 | Extension | Head reaches the vaginal introitus. Occiput rests under the pubic symphysis. Head is born by extension - occiput, bregma, forehead, nose, mouth, chin pass over the perineum |
| 6 | External rotation (Restitution) | Head rotates back to correct anatomic alignment with the fetal shoulders (transverse position) |
| 7 | Expulsion | Anterior shoulder delivers under the symphysis pubis, then posterior shoulder, then the rest of the body |
8. FETAL MONITORING DURING LABOR
| Stage | Monitoring Frequency (Low-risk) | High-risk |
|---|---|---|
| Active phase | FHR auscultation every 30 minutes after contraction | Every 15 minutes |
| Second stage | Every 15 minutes | Every 10 minutes |
- Tocodynamometer (external) or intrauterine pressure catheter (IUPC, internal) measures uterine contractions
- Fetal station = level of descent of presenting part relative to the ischial spines in cm (e.g., -3 to +3, or -5 to +5)
- Electronic Fetal Monitoring (EFM) looks at baseline FHR, variability, accelerations, and decelerations
9. DYSTOCIA - ABNORMAL LABOR (High-Yield)
| Disorder | Definition |
|---|---|
| Prolonged latent phase | >20 hrs nullipara, >14 hrs multipara |
| Protracted active phase | Dilation <1.2 cm/hr nullipara, <1.5 cm/hr multipara |
| Secondary arrest of dilation | No progress for >2 hours in active phase |
| Arrest of descent | No descent for >1 hour in second stage |
| Prolonged second stage | >2 hrs nullipara (>3 hrs with epidural), >1 hr multipara |
Causes follow the 3 Ps framework:
- Powers - inadequate uterine contractions
- Passenger - fetal malpresentation, macrosomia, deflexion
- Passage - cephalopelvic disproportion (CPD), pelvic abnormality
10. APGAR SCORE (assessed at 1 and 5 minutes)
| Sign | 0 | 1 | 2 |
|---|---|---|---|
| Appearance (color) | Blue/pale all over | Blue extremities, pink body | Pink all over |
| Pulse (heart rate) | Absent | <100 bpm | ≥100 bpm |
| Grimace (reflex) | No response | Grimace | Cry/cough/sneeze |
| Activity (muscle tone) | Limp | Some flexion | Active motion |
| Respiration | Absent | Weak/irregular | Strong cry |
- Score 7-10: Normal
- Score 4-6: Moderate depression - stimulate, supplemental O2
- Score 0-3: Severe - resuscitation required
11. QUICK CLINICAL PEARLS
- Rupture of membranes before onset of labor = PROM (Premature Rupture of Membranes). If before 37 weeks = PPROM
- Induction of labor uses cervical ripening agents (PGE2, misoprostol) and oxytocin (Pitocin)
- Epidural analgesia given in latent phase may slow progress; does not affect active phase
- Episiotomy is NOT routine - only for fetal distress, shoulder dystocia, or operative delivery
- Crowning = fetal head visible and no longer retracts between contractions
- The Ferguson reflex = cervical stretch → reflex oxytocin release → stronger contractions (positive feedback loop that drives labor to completion)
References: Guyton & Hall Textbook of Medical Physiology | Textbook of Family Medicine 9e | Morgan & Mikhail's Clinical Anesthesiology 7e | Tintinalli's Emergency Medicine | Roberts & Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.