Burning sensation in urine what it's cause
Reading File
Finding Sources
Searching PubMed
dysuria burning urination causes
Finding Sources
Searching PubMed
dysuria etiology urinary tract infection
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Now I have solid textbook information. Let me compile a thorough answer.
Burning Sensation During Urination (Dysuria) - Causes
Burning or pain during urination is called dysuria. The sensation is most often felt in the distal urethra in men, or localized to the urethra in women, and typically occurs only during voiding. Here is a complete breakdown of causes, organized by category.
Most Common Cause
Urinary Tract Infection (UTI)
This is by far the most frequent cause, especially in women. It includes:
- Cystitis (bladder infection) - burning throughout urination, often with urge and frequency
- Urethritis (urethral infection) - burning at the tip of the urethra
- Pyelonephritis (kidney infection) - burning plus fever, flank pain, nausea
- Prostatitis (prostate infection in men) - burning plus perineal discomfort
The most common bacteria causing UTI are E. coli, Klebsiella, Staphylococcus saprophyticus (in young women), and Enterococcus.
Sexually Transmitted Infections (STIs)
These frequently cause dysuria, especially in sexually active individuals:
| Pathogen | Notes |
|---|---|
| Chlamydia trachomatis | Most common STI; often silent but causes urethritis |
| Neisseria gonorrhoeae | Urethral discharge + burning |
| Herpes simplex virus (HSV) | Painful blisters + burning on urination |
| Trichomonas vaginalis | More common in women; burning + discharge |
| Mycoplasma spp. | Non-gonococcal urethritis |
Vaginal Causes (Women)
Vaginal inflammation can cause external burning as urine passes over irritated tissue:
- Bacterial vaginosis (BV)
- Vulvovaginal candidiasis (yeast infection) - itching + cottage cheese discharge
- Atrophic vaginitis (post-menopausal women, due to low estrogen)
- Allergic/chemical vaginitis (from soaps, douches, spermicides)
Urinary Stones (Calculi)
Kidney or bladder stones passing through the urethra cause intense burning and may also cause blood in the urine (hematuria).
Structural/Anatomical Causes
- Meatal stenosis - narrowing of the urethral opening
- Urethral stricture - scarring narrowing the urethra
- Benign prostatic hyperplasia (BPH) in older men - obstruction causing irritation
- Bladder or prostate neoplasm - tumor irritating the urinary lining
Irritant/Chemical Causes
- Bubble baths, soaps, spermicides, lubricants
- Certain medications (e.g., cyclophosphamide can cause hemorrhagic cystitis)
- Personal hygiene products with fragrances
Interstitial Cystitis (Painful Bladder Syndrome)
A chronic, non-infectious condition causing bladder pain and burning, more common in women. No bacteria are found on urine culture.
Other / Less Common Causes
- Trauma - from catheterization, foreign bodies, vigorous sexual activity
- Urethral syndrome - symptoms without identifiable infection
- Reactive arthritis / spondyloarthropathy - can cause sterile urethritis
- Radiation cystitis - from pelvic radiation therapy
- Referred pain from nearby pelvic structures
When to See a Doctor
Seek medical attention if you have:
- Burning lasting more than 2 days
- Fever, chills, or back/flank pain (may suggest kidney involvement)
- Blood in the urine
- Discharge from the urethra or vagina
- You are pregnant, diabetic, or immunocompromised
- Symptoms in a child or elderly person
Summary Table
| Category | Examples |
|---|---|
| Infection (UTI) | Cystitis, urethritis, pyelonephritis, prostatitis |
| STI | Chlamydia, gonorrhea, herpes, trichomonas |
| Vaginal causes | Candidiasis, BV, atrophic vaginitis |
| Stones | Kidney/bladder calculi |
| Structural | BPH, meatal stenosis, stricture, tumor |
| Irritants | Soaps, spermicides, medications |
| Chronic/other | Interstitial cystitis, radiation, trauma |
Sources: Textbook of Family Medicine 9e, Table 40-3; Smith and Tanagho's General Urology, 19th ed.
Important: Dysuria is a symptom, not a diagnosis. A urine test (urinalysis + culture) is the standard first step to identify the cause and guide appropriate treatment. Do not self-treat with antibiotics without a proper diagnosis, as overuse leads to resistance.
How are UTIs diagnosed and treated?
Finding Sources
Searching PubMed
\"urinary tract infection\" diagnosis treatment guidelines
Treatment
Finding Sources
Searching PubMed
\"urinary tract infection\" antibiotic treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Excellent - I now have comprehensive, authoritative data. Here is the full treatment guide:
UTI Treatment
Treatment depends on where the infection is (bladder vs. kidney), how severe it is (uncomplicated vs. complicated), and who the patient is (age, sex, pregnancy, immune status).
1. Uncomplicated Cystitis (Bladder Infection)
This is the most common form - typically a young, healthy, non-pregnant woman with lower urinary symptoms (burning, frequency, urgency) and no fever.
First-Line Antibiotics (Oral)
| Antibiotic | Dose | Duration | Notes |
|---|---|---|---|
| Nitrofurantoin (macrocrystals) | 100 mg twice daily | 5 days | Best clinical/microbiologic cure at 28 days; avoid if GFR is reduced |
| Trimethoprim-sulfamethoxazole (TMP-SMX) | 160/800 mg twice daily | 3 days | Only use if local E. coli resistance is <20% |
| Fosfomycin | 3 g single dose | 1 day | Convenient single dose; reserve when other options fail |
| Pivmecillinam | varies | 3-7 days | Used in Europe; limited availability elsewhere |
Fluoroquinolones (e.g., ciprofloxacin) are NOT recommended as first-line for uncomplicated cystitis due to toxicity concerns and resistance promotion. Beta-lactams (amoxicillin, cephalexin) are about 10% less effective than first-line agents but are preferred in pregnancy.
Symptomatic Relief (Adjunct Only)
- Phenazopyridine (Pyridium) 100-200 mg up to 3x/day for up to 2 days - provides topical urinary analgesia and relieves burning. Use alongside antibiotics, not instead of them. Turns urine/secretions orange - will stain contact lenses.
2. Pyelonephritis (Kidney Infection)
Presents with fever, chills, flank pain, nausea/vomiting, plus urinary symptoms.
Decision: Oral vs. IV?
| Oral (mild-moderate, no vomiting) | IV/Parenteral (severe, vomiting, sepsis) |
|---|---|
| Can treat outpatient | Hospital admission needed |
| Ciprofloxacin 500 mg bid x 5-7 days | Gentamicin (aminoglycoside) IV - best outcomes in high-resistance areas |
| Levofloxacin 750 mg once daily x 5 days | Step down to oral at 24-48 hours if improving |
| TMP-SMX or cefixime x 14 days | Total duration: 7-14 days (5-7 days if fluoroquinolone used) |
Important: Nitrofurantoin and fosfomycin do NOT achieve adequate tissue/renal levels - they must NOT be used for pyelonephritis.
3. Complicated UTI
A UTI is "complicated" when it occurs with:
- Structural/functional urinary tract abnormalities
- Urinary catheter in place
- Men, pregnant women, elderly, immunocompromised patients
- Diabetes, renal failure, recent hospitalization
- Known resistant organisms
Treatment is individualized based on:
- Culture and sensitivity results
- Site and severity of infection
- Likelihood of resistant organisms
Severe complicated UTI options (IV):
- Meropenem 1 g every 8 hours
- Piperacillin-tazobactam 4.5 g every 8 hours
- Plazomicin 15 mg/kg once daily (for highly resistant organisms)
- Meropenem-vaborbactam (for carbapenem-resistant bacteria)
Total duration: typically 10-14 days (IV x 4-5 days, then oral guided by culture).
4. Asymptomatic Bacteriuria
Bacteria in urine without symptoms - treat ONLY in:
- Pregnant women (risk of pyelonephritis and preterm birth)
- Before urologic procedures with expected mucosal trauma
For all other groups (elderly, catheterized patients, diabetics) - do NOT treat asymptomatic bacteriuria. It leads to no better outcomes and drives antimicrobial resistance.
5. UTI in Special Populations
| Group | Key Points |
|---|---|
| Pregnant women | Nitrofurantoin and oral cephalosporins preferred (safe for fetus); avoid TMP-SMX in 1st trimester and near term |
| Men | Often indicates complication (prostatitis, structural problem); treat for 7-14 days |
| Elderly | Symptoms are often atypical (confusion, falls); avoid over-diagnosing and over-treating |
| Recurrent UTI (women) | Options: patient-initiated self-treatment, continuous low-dose prophylaxis, or postcoital prophylaxis |
6. Prevention of Recurrent UTIs
For women with frequent recurrences (≥2/6 months or ≥3/year):
- Continuous low-dose prophylaxis - nitrofurantoin 50 mg nightly (most evidence)
- Postcoital prophylaxis - single dose after intercourse (if sexually triggered)
- Patient-initiated self-treatment - start antibiotics at first symptoms with pre-supplied prescription
- Behavioral measures - adequate hydration, urinate after intercourse, avoid spermicides
- Cranberry products - some evidence for prevention in women (not treatment)
- Vaginal estrogen - for post-menopausal women with atrophic vaginitis
Antibiotic Resistance Warning
Resistance rates to TMP-SMX and fluoroquinolones exceed 20% in many regions of the US and globally. Always consult local antibiogram data when selecting empiric therapy, and de-escalate based on culture results once available.
Sources: Goldman-Cecil Medicine, Table 263-6 & 263-7; Rosen's Emergency Medicine, Table 85.2; Harrison's Principles of Internal Medicine 22E (2025)
How to diagnose examine
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - here is the complete, textbook-backed guide on UTI diagnosis and examination.
How to Diagnose a UTI - Full Guide
Step 1: Clinical History (Most Important First Step)
A good history alone can establish the diagnosis in straightforward cases. Ask about:
Core urinary symptoms:
- Dysuria (burning on urination)
- Urinary frequency and urgency
- Voiding small volumes
- Suprapubic pain or pressure
- Hematuria (blood in urine)
Upper tract / systemic symptoms (suggest kidney involvement):
- Fever and chills
- Flank or back pain
- Nausea and vomiting
- Altered mental status (especially in the elderly)
Key differentiating questions:
- Vaginal discharge or odor? (suggests vaginitis)
- New/multiple sexual partners? (suggests STI)
- Onset sudden or gradual? (UTI = abrupt; STI = gradual)
- Pregnancy status?
- Any previous UTIs or recent antibiotic use?
Clinical Rule: In an otherwise healthy, non-pregnant adult woman with at least one urinary symptom (dysuria, frequency, hematuria) and no vaginal discharge, the probability of UTI is ~90%. No further testing is needed before empiric treatment in these cases.
Step 2: Physical Examination
| Finding | What It Suggests |
|---|---|
| Suprapubic tenderness | Cystitis (bladder infection) |
| Costovertebral angle (CVA) tenderness | Pyelonephritis (kidney infection) - key sign |
| Fever (>38°C) | Upper UTI or systemic infection |
| Vaginal discharge / cervical motion tenderness | STI, PID, vaginitis - not UTI |
| Urethral discharge in men | Urethritis (STI) |
| Enlarged, tender prostate on DRE | Prostatitis |
How to test for CVA tenderness: Firmly percuss (tap) the posterior flank just below the 12th rib on each side. Pain on the affected side = pyelonephritis until proven otherwise.
Step 3: Urine Dipstick (Point-of-Care, Fast)
The dipstick tests for two key markers:
| Test | What it Detects | Notes |
|---|---|---|
| Leukocyte esterase | Enzyme from white blood cells (neutrophils) = pyuria | Sensitive surrogate for pus in urine |
| Nitrite | Produced by gram-negative bacteria (e.g., E. coli) reducing nitrate | Highly specific (~95%+) when positive; can be false negative if non-gram-negative bacteria |
Interpreting results:
- Both positive → specificity ~100% for UTI - treat
- Both negative → UTI unlikely; consider other diagnoses
- Nitrite only negative → may still be UTI if organism is gram-positive (e.g., Enterococcus, Staph. saprophyticus)
- Negative dipstick does NOT rule out UTI in pregnant women - urine culture is required for them
Pitfall: Patients with urinary catheters almost always have both pyuria and bacteriuria - this alone does NOT diagnose UTI without symptoms.
Step 4: Urine Microscopy (Urinalysis)
Examined under microscope after centrifugation:
| Finding | Significance |
|---|---|
| Pyuria (WBCs) | >10 WBCs/high-power field = abnormal; present in nearly all UTIs |
| Bacteriuria | Bacteria visible on microscopy - most reliable lab sign of UTI |
| Hematuria (RBCs) | Present in ~30-50% of cystitis cases |
| Epithelial cells | Many squamous cells = specimen contamination |
| Casts | WBC casts suggest pyelonephritis/renal infection |
Step 5: Urine Culture (Gold Standard)
How to collect: Clean-catch midstream urine specimen. Patient cleans the urethral area first, begins urinating, then catches mid-stream in the sterile container. For catheterized patients - collect from the catheter port, never the drainage bag.
Interpretation:
| Colony Count | Significance |
|---|---|
| ≥10⁵ CFU/mL | Significant bacteriuria (95% likelihood of infection) |
| ≥10² CFU/mL | Significant in symptomatic women (more sensitive threshold) |
| 10⁴ CFU/mL | ~50% likelihood of infection |
| Mixed organisms | Usually contamination |
When is urine culture mandatory?
- Children
- Adult men (UTI in men is always considered complicated)
- Pregnant women
- Pyelonephritis or urosepsis
- Immunocompromised patients
- Treatment failure or recurrent infections
- Known or suspected resistant organisms
- Patients recently hospitalized or on antibiotics
- Suspected urinary obstruction
When is culture NOT needed?
- Healthy, non-pregnant adult woman with straightforward, uncomplicated cystitis - treat empirically, culture not required
Step 6: Blood Tests (Selected Cases)
| Test | When to Order |
|---|---|
| Blood cultures x2 | Suspected urosepsis, pyelonephritis with fever |
| C-reactive protein (CRP) | Elevated in pyelonephritis (normal in cystitis) |
| WBC count | Leukocytosis supports upper tract / systemic infection |
| Serum creatinine/BUN | Baseline renal function in complicated UTI |
Step 7: Imaging (Not Routine)
Most UTIs do not need imaging. Use only when:
| Imaging | Indication |
|---|---|
| Ultrasound (US) | First-line when structural abnormality or obstruction suspected; detects hydronephrosis, abscess, stones |
| CT scan (non-contrast) | Kidney stones (best test for calculi) |
| CT scan (with contrast) | Pyelonephritis not improving after 48-72 hours of antibiotics; look for abscess, obstruction, emphysematous pyelonephritis |
| MRI | Pregnancy (avoid radiation); poor at detecting gas or small stones |
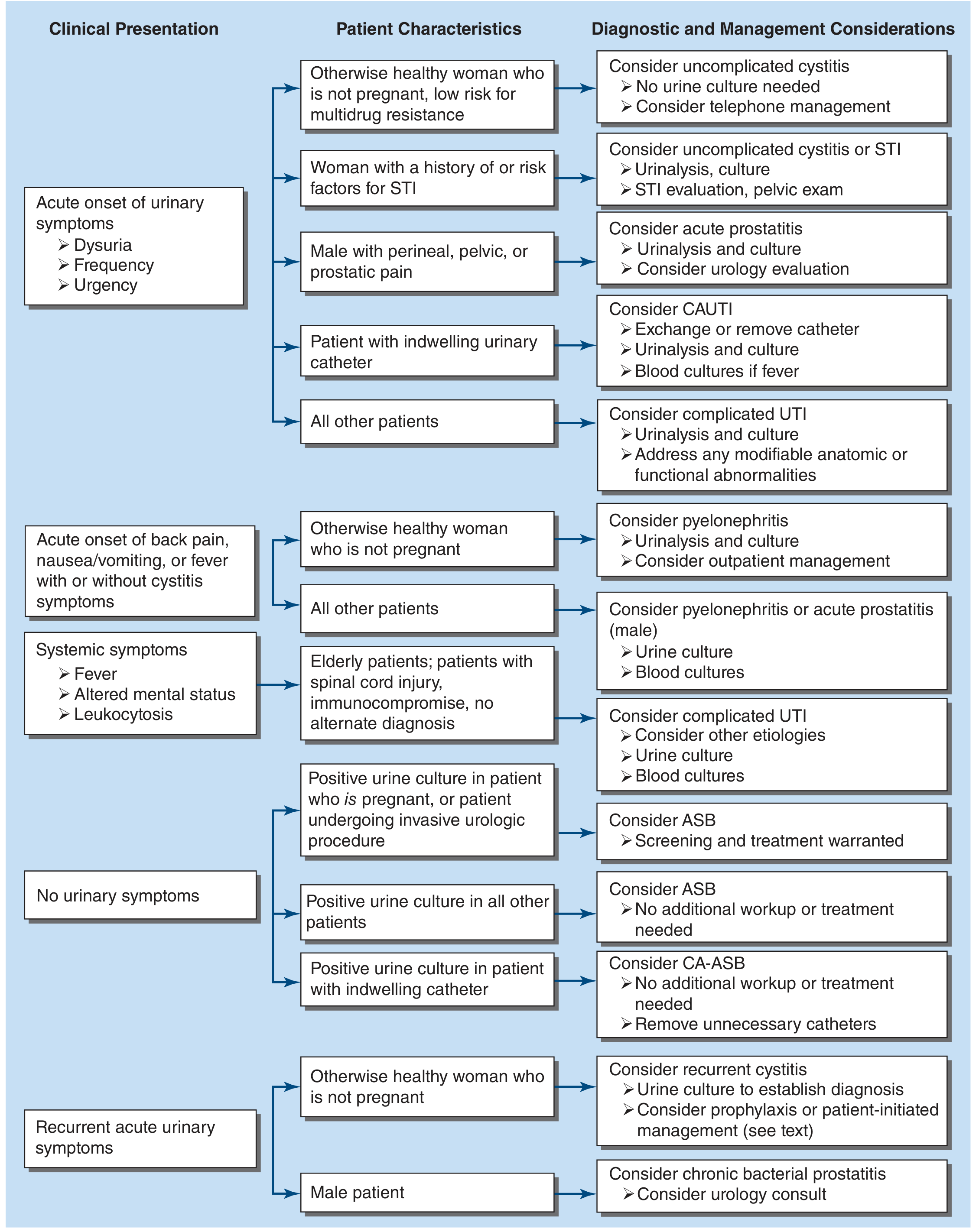
Diagnostic Flowchart (Harrison's, 2025)
Differentiating UTI vs. STI vs. Vaginitis at a Glance
| Feature | UTI | STI (Chlamydia/Gonorrhea) | Vaginitis |
|---|---|---|---|
| Type of dysuria | Internal (inside) | Internal (inside) | External (urine on skin) |
| Onset | Abrupt | Gradual | Gradual |
| Frequency/urgency | Yes | Occasional | No |
| Discharge | No | Yes (urethral/cervical) | Yes (vaginal) |
| New sexual partner | Not necessarily | Often | Sometimes |
| Pyuria | Yes | Yes (sterile pyuria possible) | No |
| Hematuria | Yes (50%) | Rare | No |
Causes of Sterile Pyuria (WBCs but no bacteria on culture)
When culture is negative but WBCs are present, consider:
- Tuberculosis (renal TB)
- Chlamydia, Gonorrhea, Mycoplasma
- Genital herpes, Trichomonas
- Fungal infections
- Schistosomiasis
Sources: Harrison's Principles of Internal Medicine 22E (2025); Rosen's Emergency Medicine; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.