steps of lichtenstein mesh hernioplasty
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have sufficient detail from two authoritative surgical textbooks (Schwartz's Principles of Surgery and Mulholland & Greenfield's Surgery). Here is the complete breakdown:
Lichtenstein Tension-Free Mesh Hernioplasty — Operative Steps
The Lichtenstein repair is the gold standard for open inguinal hernia repair, with a recurrence rate of 1–1.6%. It buttresses the inguinal floor with a flat polypropylene mesh rather than placing tissue under tension.
Anaesthesia & Patient Positioning
- Local anaesthesia with sedation (preferred), spinal, or general anaesthesia
- Patient supine; operative field prepared and draped
Step 1 — Skin Incision
- Oblique incision in the groin crease, approximately 4–6 cm, from 2 cm above and medial to the pubic tubercle toward the anterior superior iliac spine (ASIS)
- Subcutaneous fat and Scarpa's fascia divided
Step 2 — Opening the External Oblique Aponeurosis (EOA)
- EOA incised in the direction of its fibres, beginning just lateral to the external (superficial) inguinal ring and extending laterally through the ring
- Upper and lower flaps of the EOA are elevated off the underlying cord structures
- The shelving edge of the inguinal ligament is exposed inferiorly
Step 3 — Nerve Identification & Preservation
Three nerves are identified and preserved in situ:
- Ilioinguinal nerve — lies on the cord, most commonly encountered first
- Iliohypogastric nerve — runs along the internal oblique above the canal
- Genital branch of the genitofemoral nerve — runs within the cord
Step 4 — Mobilisation of the Spermatic Cord (male) / Round Ligament (female)
- Cord is encircled at the pubic tubercle using a Penrose drain
- Cremasteric fibres may be divided to expose the cord contents fully
- Cord lipomas are resected if present
Step 5 — Hernia Sac Identification & Management
Indirect hernia:
- Sac identified anteromedially on the cord, within the cremasteric fibres
- Dissected off the cord to the level of the internal ring
- Small sac: twisted and ligated at the neck, excess excised
- Large sac: divided, distal sac left open (prevents ischaemic orchitis), proximal sac ligated
Direct hernia:
- Sac/transversalis fascia defect in Hesselbach's triangle
- Sac reduced or inverted and held with a suture; no ligation required
Step 6 — Mesh Preparation
- A sheet of mid-weight polypropylene mesh (~15 × 7 cm) is used
- The medial end is rounded to match the contour of the medial inguinal canal
- A slit (keyhole) is cut laterally to create:
- A wider upper tail (two-thirds width)
- A narrower lower tail (one-third width)
- These tails will straddle the spermatic cord at the internal ring
Step 7 — Mesh Placement & Fixation (Key Step)
- Medial edge — mesh placed so it overlaps the pubic tubercle by 1.5–2 cm (reduces risk of medial recurrence); fixed to the anterior rectus sheath
- Inferior margin — using a continuous permanent monofilament suture (e.g., 1-0 Prolene), the inferior edge is sutured to the shelving edge of the inguinal ligament from medial to lateral, ending at the internal ring. Care is taken to avoid the periosteum of the pubic tubercle (prevents osteitis pubis) and femoral vessels laterally
- Superior margin — upper edge fixed to the internal oblique aponeurosis/conjoined tendon using an absorbable synthetic suture
- Internal ring — the two tails are brought around the cord so the wider upper tail crosses over the narrower lower tail; a "shutter valve" stitch is placed just lateral to the cord, incorporating the inferior surface of both tails and the inguinal ligament, to reconstruct the internal ring snugly without constricting the cord
For femoral hernia present: A triangular extension of the inferior mesh is sutured to Cooper's ligament medially and the inguinal ligament laterally, closing the femoral canal.
Step 8 — Tail Tuck Under EOA
- Lateral tails are tucked beneath the external oblique aponeurosis, extending to the level of the ASIS
- No excess mesh should bunch or fold
Step 9 — Wound Closure
- EOA closed with a continuous absorbable suture, recreating the superficial inguinal ring (ensuring the ring is not too tight around the cord)
- Subcutaneous fat approximated (Scarpa's fascia sutured)
- Skin closed with subcuticular absorbable suture or staples
Surgical Diagram
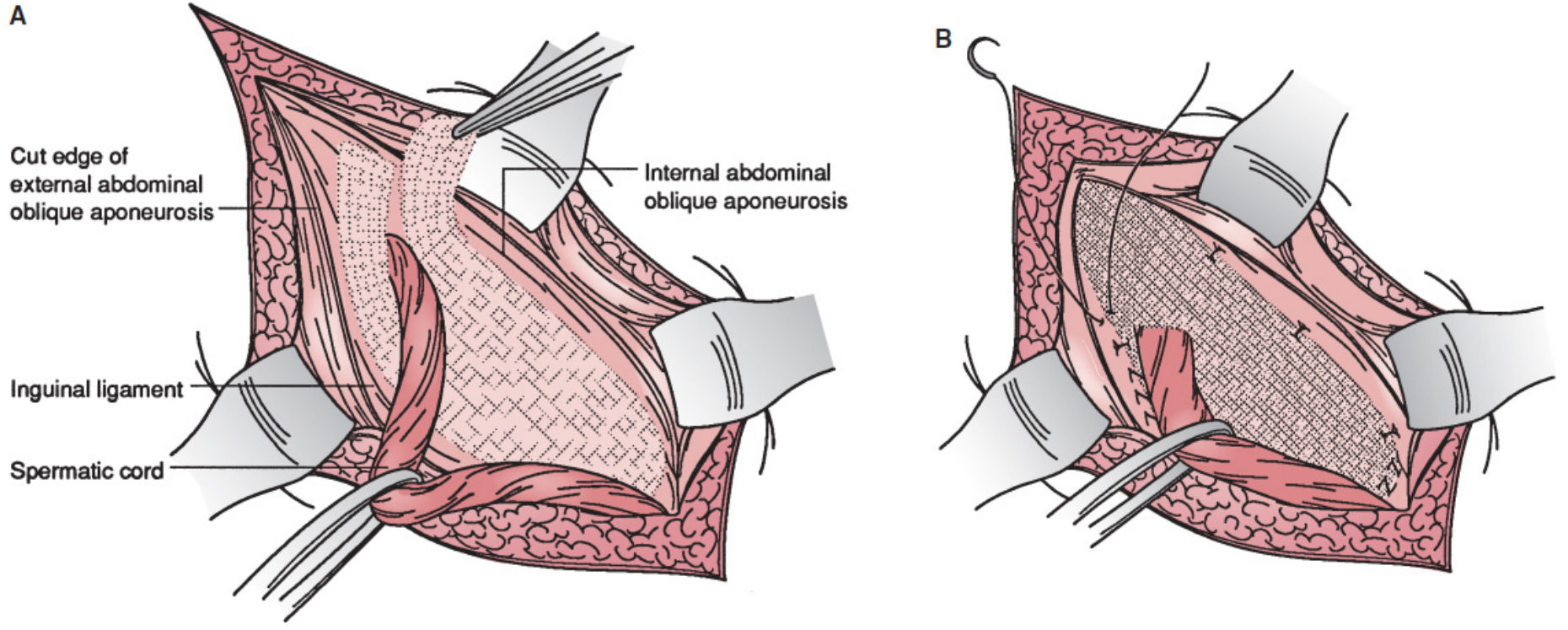
A: mesh laid flat over the inguinal floor; B: mesh sutured in place with tails fashioned around the spermatic cord at the internal ring
Key Principles to Remember
| Feature | Detail |
|---|---|
| Mesh overlap at pubic tubercle | ≥1.5–2 cm medially |
| Inferior fixation suture | Permanent monofilament (Prolene) |
| Superior fixation suture | Absorbable synthetic |
| Tails ratio | Upper 2/3, lower 1/3 |
| Shutter valve stitch | Prevents cord herniation through keyhole |
| Avoid | Periosteum of pubic tubercle (osteitis pubis), direct suture into inguinal ligament periosteum |
| Recurrence rate | ~1–1.6% |
Sources: Schwartz's Principles of Surgery, 11th ed., Ch. 37; Mulholland & Greenfield's Surgery, 7th ed., Ch. 72
Steps of TAPP/TEP operation for inguinal hernia repair
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from three authoritative textbooks. Here is the full breakdown of both procedures:
Laparoscopic Inguinal Hernia Repair: TAPP & TEP
Both TAPP and TEP access the preperitoneal space to place a mesh over the myopectineal orifice (MPO) — the difference is how that space is reached.
Common Prerequisites for Both
| Feature | Detail |
|---|---|
| Anaesthesia | General (mandatory for both) |
| Position | Supine, arms tucked, Trendelenburg ~15–20° |
| Surgeon | Stands contralateral to the hernia |
| Video screen | At the foot of the table |
| Mesh size | ≥10 × 15 cm to fully cover the MPO |
| Grade A indication | Recurrent hernia after prior open anterior repair; bilateral hernias |
TAPP — Transabdominal Preperitoneal Repair
The peritoneal cavity is entered first, then the peritoneum is incised to reach the preperitoneal space from inside.
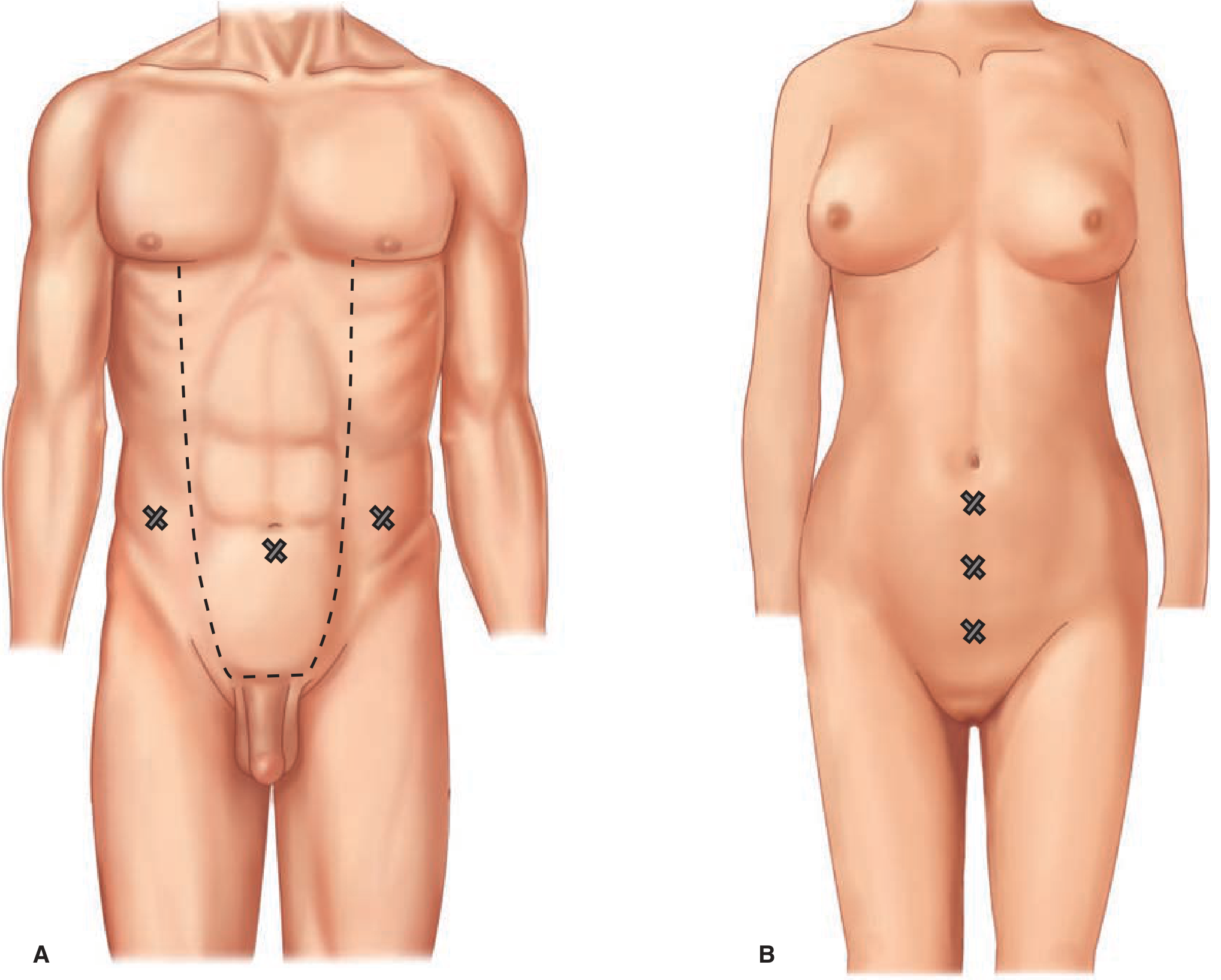
Trocar Placement (TAPP)
- 12-mm camera port — infraumbilical midline (at least 15 cm from pubis)
- Two 5-mm working ports — placed lateral to the camera port, one on each side, avoiding the inferior epigastric vessels
Step-by-Step TAPP
Step 1 — Establish pneumoperitoneum
- Abdominal cavity accessed via dissecting trocar or open Hasson technique
- Pneumoperitoneum to 15 mmHg
Step 2 — Peritoneal inspection
- Patient placed in Trendelenburg
- Identify: bladder, median and medial umbilical ligaments, external iliac vessels, inferior epigastric vessels
- Type and location of hernia confirmed: direct (Hesselbach's triangle), indirect (lateral to inferior epigastrics), or femoral
Step 3 — Peritoneal incision
- Incise peritoneum at the medial umbilical ligament, 3–4 cm superior to the hernia defect
- Carry the incision laterally to the ASIS
- For bilateral repair: bilateral peritoneal incisions with a midline bridge of tissue preserved to avoid injuring a patent urachus
Step 4 — Preperitoneal dissection (Critical View of MPO)
The following must all be achieved:
- Identify and dissect past the pubic tubercle to the midline
- Expose Cooper's ligament ipsilaterally (and contralateral for large direct hernias)
- Visualise Hesselbach's triangle and clear any fat obscuring a direct defect
- Develop space of Retzius (≥2 cm between Cooper's ligament and bladder — prevents mesh "clamshelling" with bladder distension)
- Dissect femoral orifice between external iliac vein and Cooper's ligament
- Parietalize the cord structures: dissect indirect sac and peritoneum off gonadal vessels/vas deferens until cord elements lie flat
- Extend dissection lateral to ASIS so peritoneal reflection will lie inferior to mesh
- Identify and reduce/excise cord lipomas
Step 5 — Hernia sac management
- Direct hernia: sac inverted and fixed to Cooper's ligament with a tack (prevents haematoma/seroma)
- Indirect hernia: sac grasped, elevated superiorly from cord; space below developed bluntly; sac dissected free and cord skeletonised
Step 6 — Mesh placement
- Mesh (10 × 15 cm or larger) rolled lengthwise, placed through the 12-mm trocar
- Unrolled in the preperitoneal space to completely cover the MPO
- Medial fixation: tacked to Cooper's ligament (surgeon palpates tacker tip externally for proper angle)
- Lateral fixation: fixed to the anterior superior iliac spine
- ⚠️ All tacks/fixation placed above the iliopubic tract (to avoid lateral cutaneous nerve of thigh and femoral branch of genitofemoral nerve)
- Mesh should NOT be split for cord pass-through
Step 7 — Peritoneal closure
- Peritoneal edges reapproximated using tacks or intracorporeal sutures — must be completely closed to exclude mesh from bowel contact and prevent adhesions
- Confirm mesh lies flat without folds during closure
Step 8 — Closure
- Abdomen desufflated
- Trocars removed
- 12-mm port fascia closed with suture
- Skin closed
TEP — Totally Extraperitoneal Repair
The peritoneal cavity is never entered. The preperitoneal space is created anterior to the peritoneum using balloon dissection.
Trocar Placement (TEP)
- 12-mm port — infraumbilical (camera port, placed through the anterior rectus sheath)
- 5-mm port — suprapubic midline
- 5-mm port — inferior to the camera port (all ports in the midline)
Step-by-Step TEP
Step 1 — Infraumbilical incision and anterior rectus sheath access
- Small horizontal incision inferior to the umbilicus
- Dissect subcutaneous tissue to the anterior rectus sheath
- Incise the anterior rectus sheath lateral to the linea alba
- Place stay sutures on the sheath edges
- Retract the rectus muscle superolaterally, revealing the posterior rectus sheath beneath
Step 2 — Initial development of retrorectus/preperitoneal space
- Manually develop the retromuscular/preperitoneal space from the incision down to the pubic tubercle using finger/blunt dissection
Step 3 — Balloon dissection of preperitoneal space
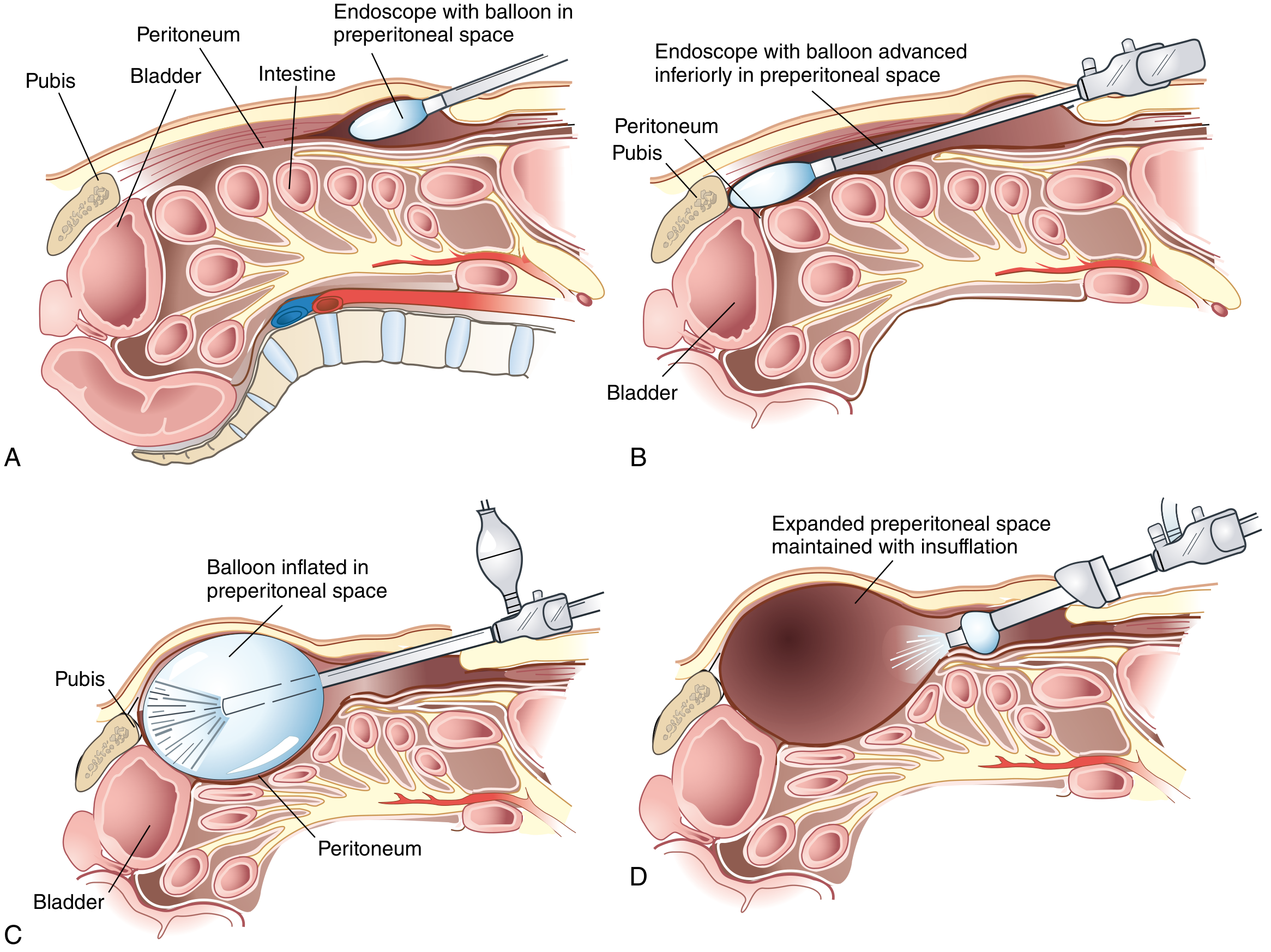
- Insert dissecting balloon directed toward the pubic symphysis
- Under direct vision with a 30° laparoscope, slowly inflate the balloon to bluntly dissect the preperitoneal space (Space of Retzius)
- Balloon is then deflated and removed
Step 4 — Establish pneumopreperitoneum
- 12-mm balloon trocar placed at the infraumbilical incision
- Pneumopreperitoneum to 15 mmHg achieved by CO₂ insufflation
- Two 5-mm trocars placed: one suprapubic midline, one inferior to the camera port
Step 5 — Preperitoneal dissection (Critical View of MPO)
- Identical dissection goals as TAPP (see above)
- Identify: pubic tubercle, Cooper's ligament, direct/indirect/femoral spaces, cord structures, inferior epigastric vessels
- Parietalize cord, reduce hernia sac, excise cord lipomas
- Extend laterally beyond ASIS
Step 6 — Hernia sac management
- Direct hernia: sac/transversalis fascia reduced into the preperitoneal space
- Indirect hernia: sac carefully dissected off cord; if sac is large, divide it, close the peritoneal defect, leave the distal sac in situ
- ⚠️ Any peritoneal rents must be repaired before desufflation to prevent mesh contact with bowel
Step 7 — Mesh placement
- Identical to TAPP: ≥10 × 15 cm mesh placed to cover entire MPO
- Fixed medially to Cooper's ligament; laterally to ASIS
- All fixation above the iliopubic tract
- Mesh lies flat without creases; do NOT split the mesh
Step 8 — Desufflation and closure
- Preperitoneal space desufflated slowly under direct vision to confirm mesh does not fold or migrate
- Reposition mesh if folding occurs
- Trocars removed
- Anterior rectus sheath closed with an interrupted suture
- Skin closed
TAPP vs TEP — Key Differences
| Feature | TAPP | TEP |
|---|---|---|
| Peritoneal cavity entered? | Yes | No |
| Space created by | Peritoneal incision + dissection | Balloon dissection of preperitoneal space |
| Camera port size | 12 mm umbilical | 12 mm infraumbilical (retrorectus) |
| Working ports | 2 × 5 mm lateral | 2 × 5 mm midline/inferior |
| End step | Close peritoneal flap | Slowly desufflate under vision |
| Advantage | Better view; good for bilateral, large, recurrent hernias | No peritoneal entry; lower risk of bowel injury/port site hernia |
| Disadvantage | Peritoneal closure required; intra-abdominal adhesion risk | Narrower working space; peritoneal tear = CO₂ leaks into abdomen |
| Preferred for robotic? | Yes (TAPP) | TEP also used |
Mesh Coverage: The Myopectineal Orifice
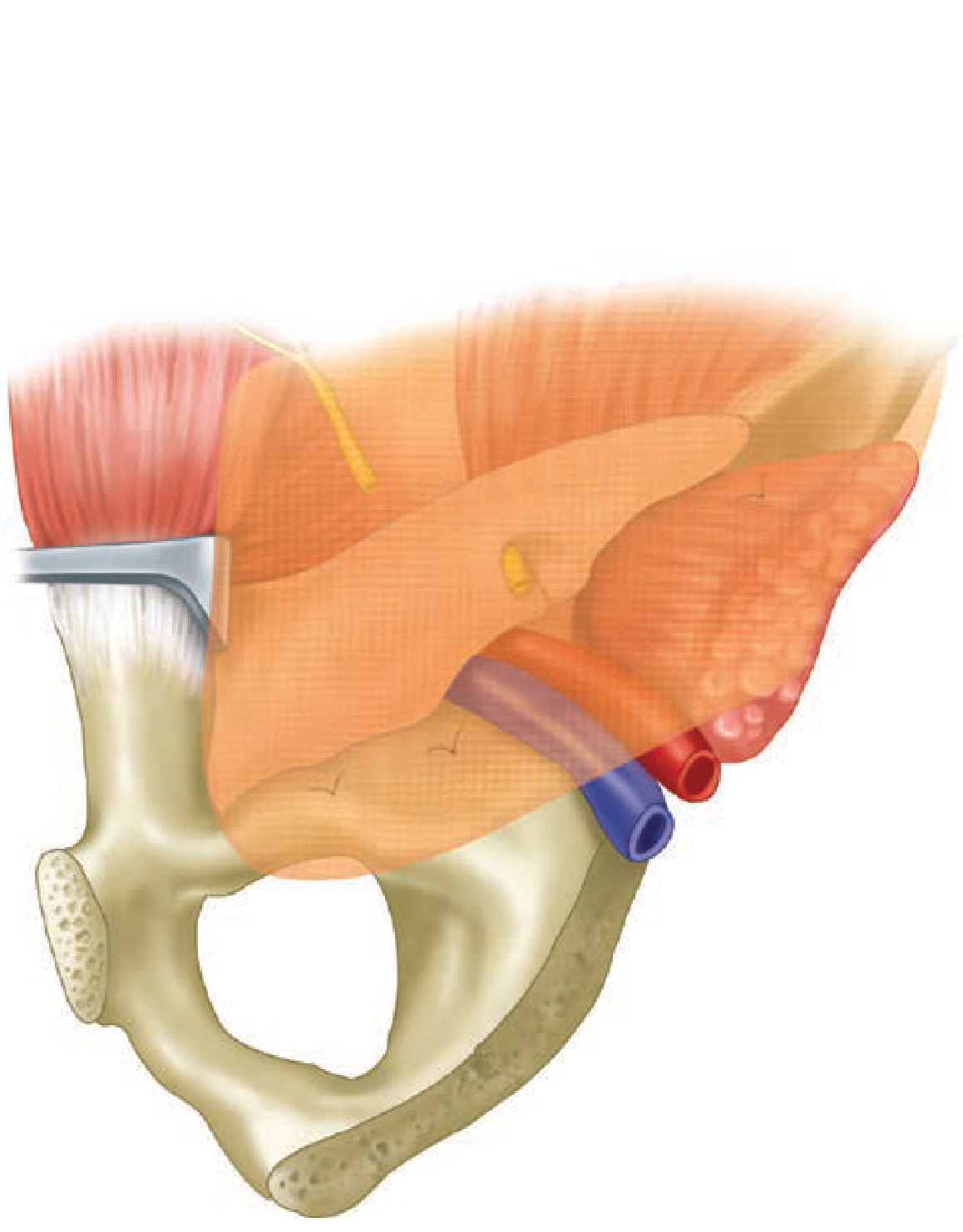
A single large mesh covers all three potential hernia sites simultaneously: indirect, direct, and femoral.
Danger Zones ("Triangle of Doom / Triangle of Pain")
- Triangle of Doom (medial): bounded by vas deferens and gonadal vessels — contains external iliac artery and vein → no tacks here
- Triangle of Pain (lateral): bounded by iliopubic tract and gonadal vessels — contains lateral cutaneous nerve, genitofemoral nerve → no tacks below iliopubic tract laterally
Sources: Schwartz's Principles of Surgery, 11th ed., Ch. 37; Mulholland & Greenfield's Surgery, 7th ed., Ch. 72; Sabiston Textbook of Surgery, Ch. 82
steps of open appendectomy
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.