Vestibular evoked myogenic potential
Reading File
Finding Sources
Searching PubMed
"vestibular evoked myogenic potential" VEMP
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Here is a thorough overview of Vestibular Evoked Myogenic Potentials (VEMP) based on Shambaugh's Surgery of the Ear:
Vestibular Evoked Myogenic Potential (VEMP)
What Is VEMP?
VEMP testing is the only commonly used electrophysiological test of the inferior vestibular nerve. It uses an intense sound stimulus (90-100 dB) to stimulate the sacculus - one of the otolith organs of the inner ear - which evokes a response via the inferior vestibular nerve. This produces a vestibulospinal response detected as a relaxation (inhibitory potential) in the ipsilateral sternocleidomastoid (SCM) muscle, recorded via surface EMG.
Evidence that the response is truly vestibular in origin:
- It disappears after vestibular neurectomy
- It is still present in patients with absent hearing but intact vestibular function
- VEMP responses were absent in most vestibular neuritis patients who did not develop posterior canal BPPV afterward
(Shambaugh Surgery of the Ear, p. 152)
Types of VEMP
| Type | Muscle Recorded | Otolith Tested | Nerve | Stimulus |
|---|---|---|---|---|
| cVEMP (cervical) | Sternocleidomastoid (SCM) | Saccule | Inferior vestibular nerve | Air-conducted sound (clicks/tone bursts) |
| oVEMP (ocular) | Periocular / extraocular muscles | Utricle | Superior vestibular nerve | Air-conducted sound or bone vibration |
oVEMP responses are particularly sensitive to superior canal dehiscence syndrome (SCDS), where responsiveness changes markedly.
Test Technique
Stimulus: Intense repeating click or tone burst at 90-100 dB, delivered to the test ear for 30 seconds.
Patient positioning (two protocols):
-
Head lift protocol (preferred): Patient lies supine and lifts the head ~2 inches off the table without sitting up or lifting the shoulders - this bilaterally activates the SCM muscles.
-
Head turn protocol (for patients who cannot perform head lift): Patient is seated and turns the head sharply to one side, activating the SCM on the contralateral side.
The response can only be recorded when the SCM muscle is under active contraction - the inhibitory potential (relaxation) is superimposed on the tonic EMG activity.
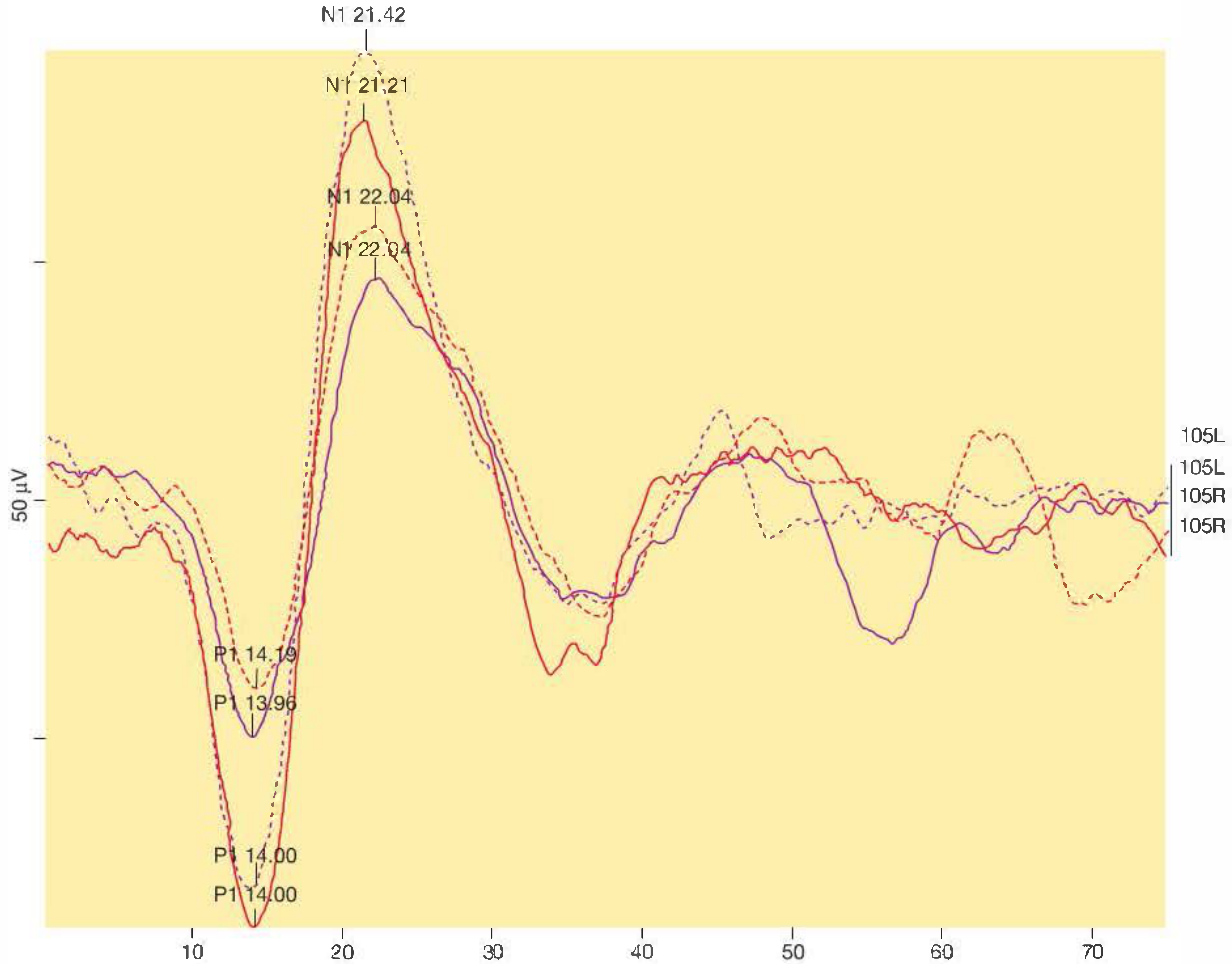
Normal VEMP Waveform
The response is a biphasic deflection on EMG:
- P1 (positive deflection): peak at 12-16 ms after stimulus onset (typically ~13-14 ms)
- N1 (negative deflection): peak at 22-24 ms after stimulus onset (typically ~21-23 ms)
Normal VEMP tracing showing P1 at ~14 ms and N1 at ~21 ms bilaterally:
Interpretation Parameters
1. Amplitude / Interaural Asymmetry Ratio (AR)
Because absolute amplitude varies widely between individuals, the left and right sides are compared using the asymmetry ratio:
AR = (A_L - A_R) / (A_L + A_R) × 100
This is analogous to Jongkees' formula in caloric testing. Each lab should establish its own normative data. A common cutoff is >30% difference as significant.
2. Threshold
- The threshold for eliciting a VEMP response can be determined (though more time-consuming)
- Reduced threshold = seen in irritative or third-window lesions
3. Latency
- Increased P1 latency (>17 ms) is suggestive of central vestibular dysfunction
Clinical Significance
| Finding | Interpretation |
|---|---|
| Absent VEMP / low amplitude (AR > 2 SD) | Peripheral vestibular hypofunction (paretic lesion): vestibular neuritis, Meniere's disease (acute), acoustic neuroma, intratympanic gentamicin |
| Increased amplitude | Irritative lesion: Meniere's disease (recovery phase), Superior Canal Dehiscence Syndrome (SCDS) |
| Reduced threshold + elevated amplitude | Classic pattern of SCDS |
| Increased latency | Central vestibular dysfunction |
| Absent response with intact hearing | Inferior vestibular nerve lesion, saccular damage |
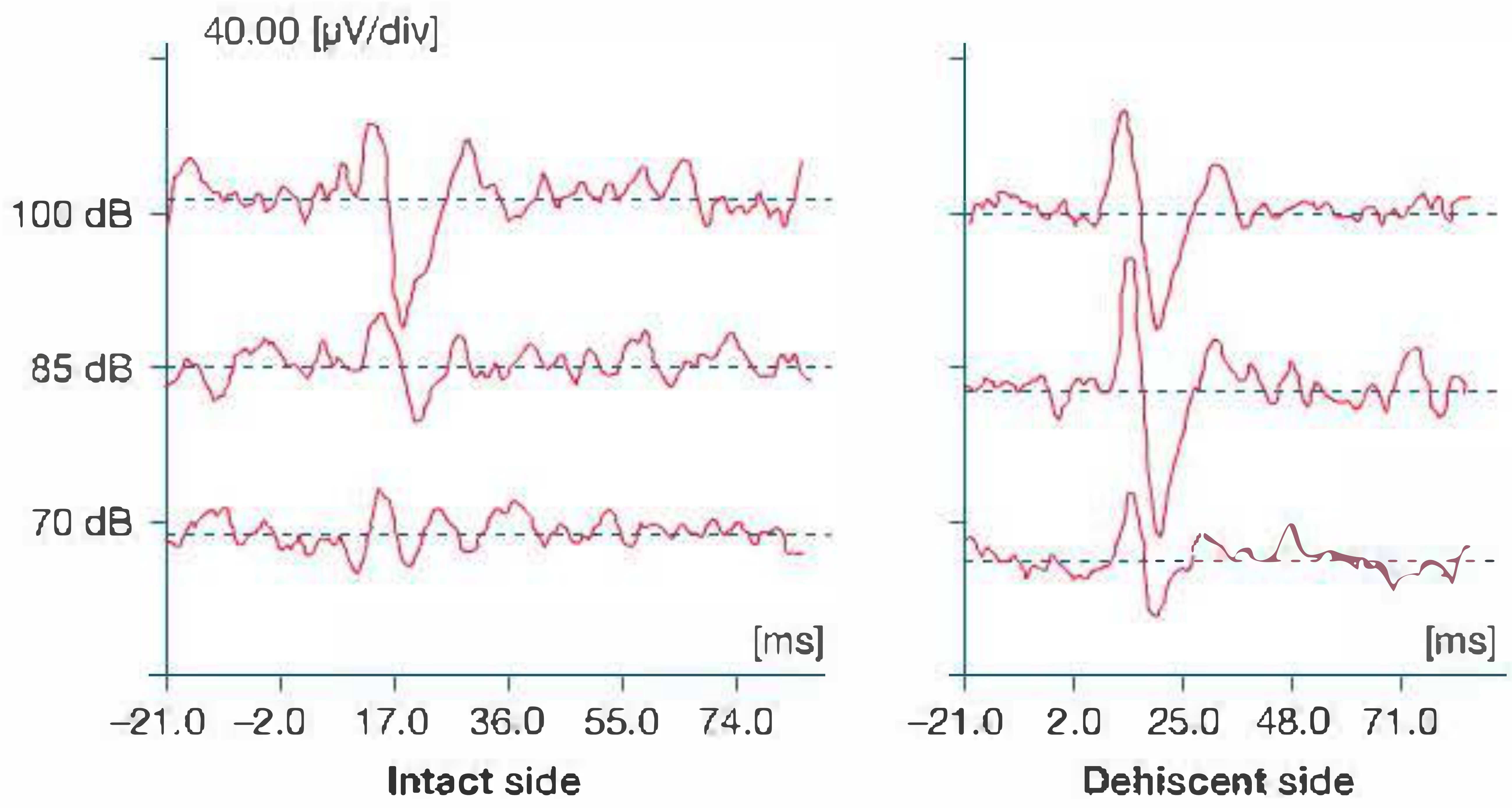
The image below (from Shambaugh, p. 152) shows VEMP thresholds comparing the intact side (left) vs. the dehiscent side (right) in SCDS - note the dramatically lower threshold and larger amplitude on the dehiscent side even at 70 dB:
Key Clinical Applications
-
Superior Canal Dehiscence Syndrome (SCDS): VEMP is particularly useful - low threshold and elevated amplitude in the affected ear. Also look for Tullio phenomenon and Hennebert's sign.
-
Meniere's Disease: Amplitude may be decreased (during attacks/paretic phase) or increased (recovery phase).
-
Vestibular Neuritis: VEMP responses absent in most cases that do not subsequently develop BPPV (as the inferior nerve is spared in vestibular neuritis affecting primarily the superior nerve, but the inferior nerve is affected in complete neuritis).
-
Acoustic Neuroma / Vestibular Schwannoma: Reduced or absent cVEMP.
-
Otosclerosis: Recent systematic review (Pinto et al., 2025; PMID 39297597) has evaluated VEMP changes in otosclerosis.
-
Third mobile window syndrome (general): Electrophysiological roles reviewed in a 2025 systematic review (Legois et al., PMID 40603203).
-
Galvanic VEMP: A 2026 systematic review (Young et al., PMID 41566896) covers clinical applications of galvanic vestibular-evoked myogenic potentials in audiovestibular disorders.
Summary Table
| Parameter | Normal Value | Abnormal Finding | Likely Cause |
|---|---|---|---|
| P1 latency | 12-16 ms | >17 ms | Central vestibular pathology |
| N1 latency | 22-24 ms | Prolonged | Central pathology |
| Asymmetry ratio | <30% | >30% | Peripheral dysfunction |
| Threshold | High (>90 dB) | Low (<85 dB) | SCDS, third window |
| Amplitude | Symmetric | Increased unilaterally | SCDS, irritative lesion |
| Response present? | Yes | Absent | Paretic lesion, inferior VN damage |
- Shambaugh's Surgery of the Ear, pp. 152, 266-268
This is a shared conversation. Sign in to Orris to start your own chat.