Spina Bifida
Reading File
Finding Sources
Searching PubMed
"spina bifida" OR "myelomeningocele"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Now I have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Spina Bifida
Definition & Embryology
Spina bifida is the most common neural tube defect (NTD), resulting from failure of the posterior vertebral arches (and often the underlying neural tube) to close during embryogenesis. Neural tube closure is normally complete by day 26-28 of embryonic development - before most pregnancies are even recognized. Failure of posterior neuropore closure by day 26 results in the open forms of the condition.
The vertebral defect incidence ranges from 0.04% to 0.15%, occurring more often in females than males. Globally it occurs at a rate of ~1 per 1,000 births; in the United States, ~0.6 per 1,000 births.
Classification
Spina bifida represents a spectrum:
| Type | Description | Key Features |
|---|---|---|
| Spina bifida occulta | Bony vertebral arch defect only; neural tissue not involved | Typically asymptomatic; incidental finding on imaging. May have overlying cutaneous stigmata (dimple, hairy patch, naevus) |
| Meningocele | Meninges + CSF herniate through the defect, covered by skin | No neural tissue in the sac; better prognosis |
| Myelomeningocele | Spinal cord + meninges herniate; neural tissue exposed | Most severe form; ~75% develop hydrocephalus |
| Myelocele | Open midline lesion with neural tissue flush with adjacent skin surface | Visible at birth as a midline back lesion |
About 80% of spina bifida cases are the open type (myelomeningocele/myelocele), covered only by a thin membrane of exposed neural tissue.
MRI appearance - myelocele vs. myelomeningocele:
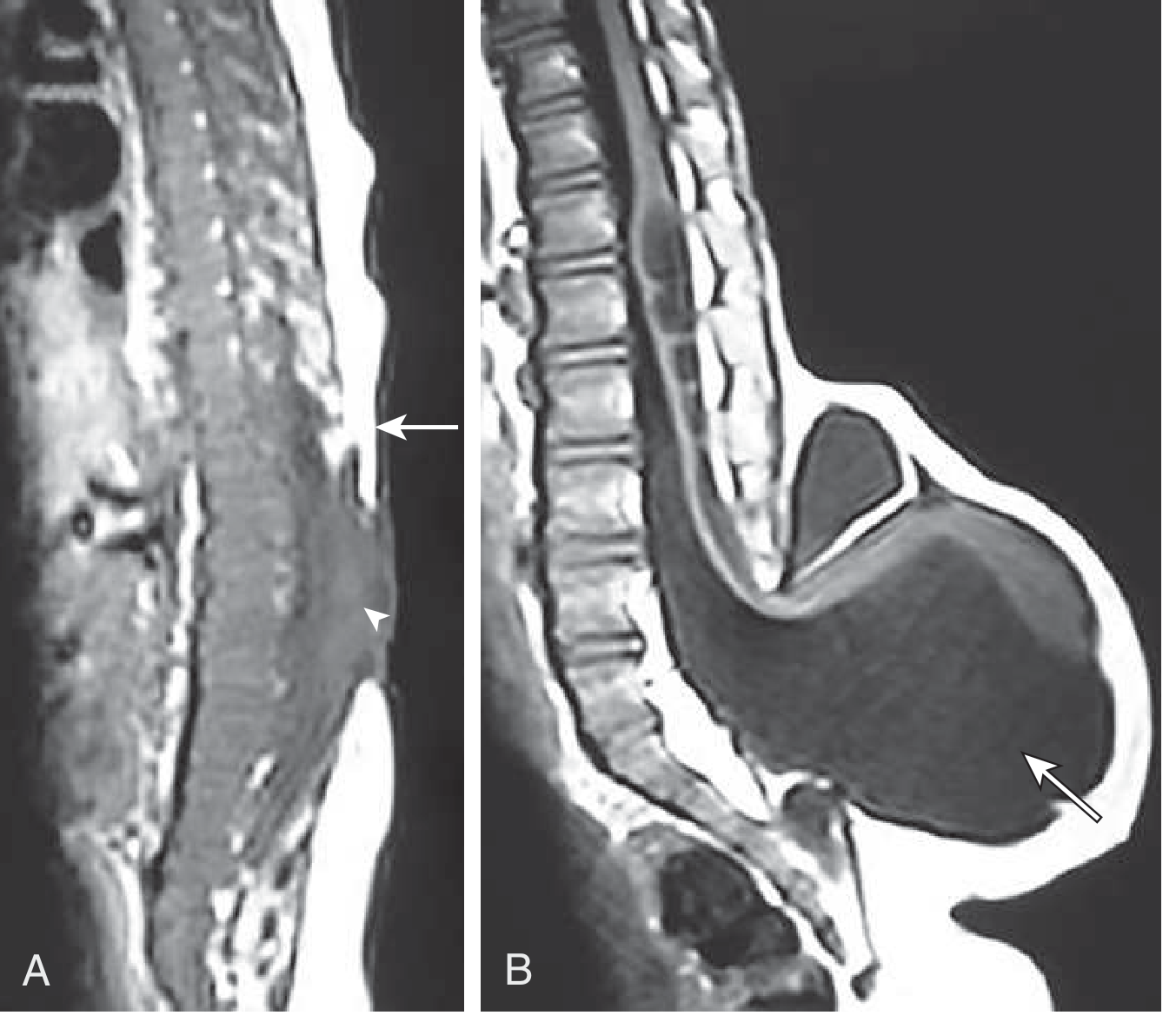
Sagittal T1 MRI: (A) Myelocele - neural tissue (arrowhead) is level with adjacent skin surface (arrow). (B) Myelomeningocele - lesion extends beyond the skin surface, containing nerve tissue and CSF (arrow). - Goldman-Cecil Medicine
Clinical photo - myelomeningocele at birth:

Myelomeningocele: Both meninges and spinal cord parenchyma are included in the cyst-like structure visible just above the buttocks. - Robbins Pathology
Etiology & Risk Factors
- Folic acid deficiency - the primary modifiable risk factor. Folate deficiency in the first few weeks of gestation (before most pregnancies are detected) disrupts neural tube closure; precise mechanism is uncertain but effects on DNA methylation are suspected.
- Chromosomal deletions, duplications, and trisomies can cause NTDs; single gene mutations are uncommon.
- Valproic acid use during pregnancy significantly increases the risk.
- Vitamin A deficiency may play a role.
- Polymorphisms in enzymes involved in folic acid metabolism (e.g., MTHFR) contribute to population differences.
Clinical Manifestations
The clinical picture depends on the level of the lesion and extent of spinal cord involvement:
- Lumbosacral lesions (most common site): Motor weakness and sensory loss below the lesion level; less devastating than thoracic or cervical lesions.
- Bowel and bladder dysfunction: Almost universal regardless of the level; leads to neurogenic bladder, recurrent urinary tract infections, and risk of renal failure.
- Hydrocephalus: ~75% of myelomeningocele patients; usually Chiari II malformation is also present.
- Chiari II malformation: Downward displacement of cerebellar vermis, tonsils, fourth ventricle, and medulla through the foramen magnum. Almost always associated with lumbosacral myelomeningocele.
- Tethered cord: Progressive neurological deterioration from spinal cord traction.
- Seizures/epilepsy: Common when associated brain malformations or hydrocephalus are present.
- Skeletal deformities: Kyphosis, clubfoot, extremity contractures, neuromuscular scoliosis.
- Pressure ulcers: Caused by sensory loss below the lesion.
- Latex allergy: Frequency increases with age; mechanism unclear.
- Cognitive and developmental delays: Especially in those with hydrocephalus.
Prenatal Diagnosis
- Maternal serum AFP (alpha-fetoprotein): Elevated due to leakage from the exposed neural tube.
- Amniotic fluid acetylcholinesterase: Normally found in CSF but not amniotic fluid - its presence strongly suggests an open NTD.
- Prenatal ultrasound: Often detects the defect; characteristic signs include the "lemon sign" (frontal bone scalloping) and "banana sign" (Chiari II). MRI can further define extent.
Treatment & Management
Postnatal:
- Antibiotics should be started immediately after birth.
- Surgical closure within 3 days of birth is standard.
- Ventriculoperitoneal (VP) shunt is usually required for hydrocephalus (a 2024 meta-analysis [PMID 39126714] examined whether simultaneous vs. delayed shunt placement at time of closure is preferable - this remains a debated clinical question).
- Conservative management for meningocele with intact skin; more complex defects require early closure.
- Long-term management includes skin care, bladder training (clean intermittent catheterization), orthopedic management of deformity, and neuropsychological support.
Fetal (prenatal) surgery:
- Prenatal closure of the spinal lesion can reduce the incidence of hydrocephalus and may improve motor outcomes. A 2025 systematic review and meta-analysis [PMID 40492626] evaluated benefits and complications of fetal vs. postnatal surgical repair of open spina bifida.
Any neurological deterioration in a patient with myelomeningocele should prompt evaluation for worsening hydrocephalus, tethered cord, or syrinx formation - as myelomeningocele itself is a static lesion.
Prevention
- Periconceptional folic acid supplementation is the cornerstone of prevention:
- Low-risk women: 0.4 mg/day
- High-risk women (prior affected pregnancy): 4 mg/day
- Supplementation must begin before conception, as the neural tube closes before most pregnancies are recognized.
- Food fortification with folic acid (e.g., in flour/bread) has contributed to declining incidence worldwide.
- The incidence of spina bifida cystica is decreasing as a result of folic acid supplementation, antenatal ultrasound surveillance, and measurement of AFP levels.
Associated Conditions
- Chiari II malformation - nearly always present with myelomeningocele
- Spinal dysraphism (includes tethered cord, diastematomyelia, lipomeningocele)
- Syringomyelia
- Agenesis of the corpus callosum
- Neuropathic bladder (congenital neuropathic bladder)
Sources: Goldman-Cecil Medicine | Robbins & Cotran Pathologic Basis of Disease | Bailey and Love's Short Practice of Surgery 28th Ed. | The Developing Human: Clinically Oriented Embryology | Campbell-Walsh-Wein Urology | Gray's Anatomy for Students
Recent evidence note:
- PMID 40492626 (2025, Meta-Analysis): Fetal vs. postnatal surgery for open spina bifida - systematic review showing distinct benefit/complication profiles for prenatal repair.
- PMID 39126714 (2024, Meta-Analysis): Simultaneous vs. delayed VP shunt placement at myelomeningocele closure - no definitive consensus yet established.
This is a shared conversation. Sign in to Orris to start your own chat.