Wound healing & Repair Explain whole topic as essay for 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed to write a comprehensive, well-structured 10-mark essay. Let me compose it.
Wound Healing and Repair
Introduction
Wound healing is the body's fundamental response to tissue injury - a complex, coordinated biological process aimed at restoring mechanical integrity, re-establishing barriers to fluid loss and infection, and re-establishing normal blood and lymphatic flow. Unlike true regeneration (which restores pre-existing tissue architecture perfectly, as seen in embryonic development, liver, or bone), repair in most tissues sacrifices perfect restoration in favor of a return to function, often resulting in a fibrous scar. The entire process is orchestrated through overlapping, sequential phases involving platelets, inflammatory cells, fibroblasts, endothelial cells, and the extracellular matrix (ECM).
Phases of Wound Healing
Wound healing proceeds through four overlapping phases: hemostasis, inflammation, proliferation (repair), and maturation (remodeling). All phases may occur simultaneously in different areas of a large wound, and disruption of any phase leads to impaired healing.
Phase 1 - Hemostasis (Minutes to Hours)
Immediately after injury, the body attempts to stop hemorrhage. Disrupted blood vessels cause local vasoconstriction, followed by platelet adhesion to exposed subendothelial collagen. This requires von Willebrand factor (vWF), and platelet binding is mediated through integrin receptors (GPIIb-IIIa/αIIbβ3 for fibrinogen; α2β1 for collagen; α6β1 for laminin). Platelet activation triggers intracellular signaling, releasing biologically active molecules including platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), vascular endothelial growth factor (VEGF), and fibronectin. A hemostatic plug forms, and the coagulation cascade is activated, culminating in a fibrin clot. This clot not only stops bleeding but also forms a provisional scaffold for the cellular migration that follows.
Phase 2 - Inflammation (6 Hours to ~3 Days)
The inflammatory phase is characterized by:
- Increased vascular permeability (vasodilatation after initial vasoconstriction)
- Chemotaxis and migration of leukocytes into the wound
- Secretion of cytokines and growth factors
- Activation of migrating cells
Neutrophils arrive first (within 6-48 hours), attracted by bacterial products, complement fragments, and cytokines such as IL-1, TNF, and IL-8. They are primarily responsible for phagocytosis of bacteria and debris.
Monocytes/Macrophages predominate by 48-72 hours and are the most critical cells in orchestrating repair. They eliminate offending agents, phagocytose necrotic tissue, and produce a rich array of growth factors (PDGF, FGF, VEGF, TGF-β) that drive the subsequent proliferative phase. Macrophages transition from classically activated (M1, pro-inflammatory) to alternatively activated (M2, anti-inflammatory, pro-repair) phenotypes, and this shift is essential for terminating inflammation and initiating repair.
Lymphocytes appear later (after ~72 hours) and help modulate the immune response.
This inflammatory phase, while protective, must resolve in a timely manner. Chronic inflammation (as in diabetic or pressure ulcers) stalls the wound in this phase and prevents progression.
Phase 3 - Proliferation / Repair (~3 to 21 Days)
As acute inflammation subsides, the scaffold is laid for tissue repair. Three key processes occur simultaneously:
a) Re-Epithelialization
Epithelial cells at the wound edges respond to locally produced growth factors (EGF, FGF, TGF-α) and migrate over the wound surface, covering it. This restores the epithelial barrier.
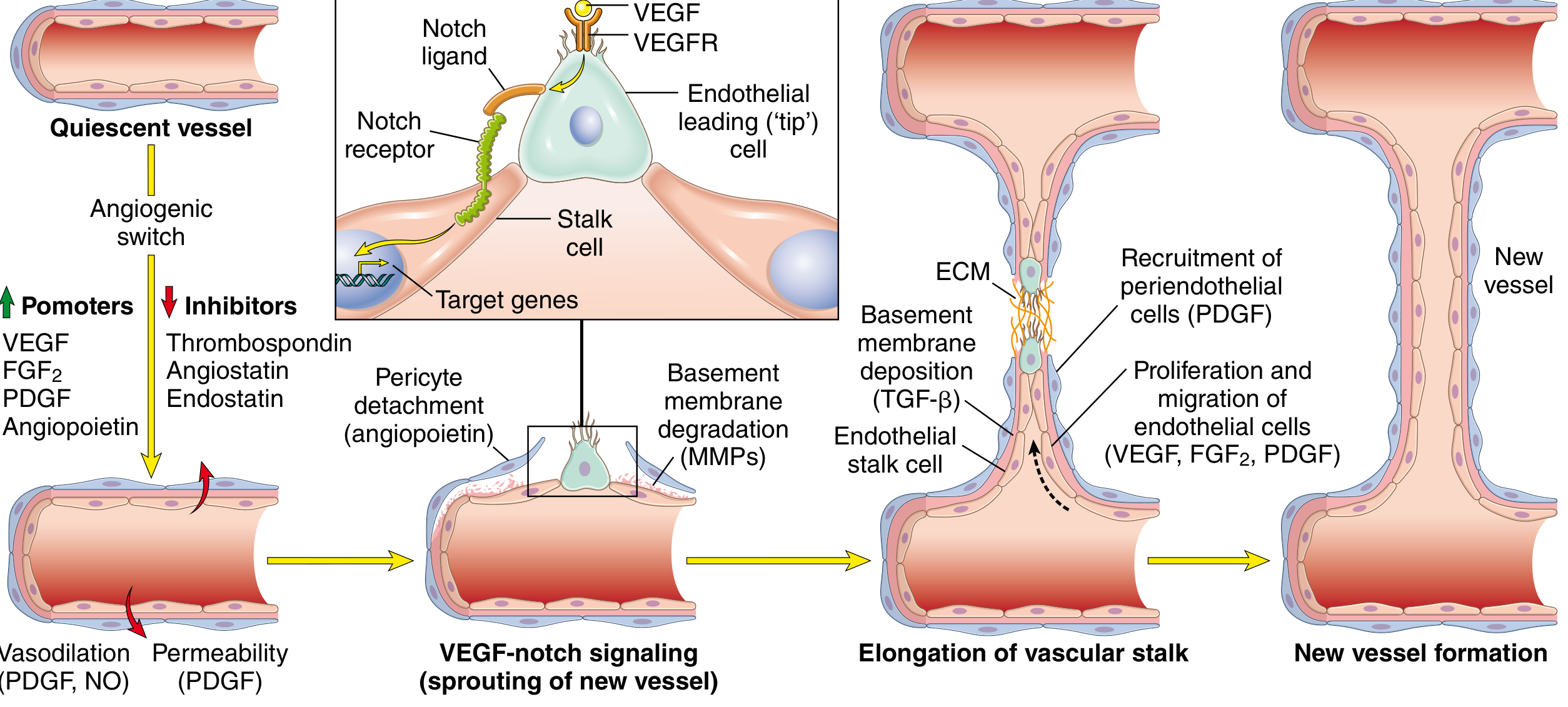
b) Angiogenesis (Neovascularization)
New blood vessels form by sprouting from existing vessels - a process driven primarily by VEGF (stimulates endothelial cell migration and proliferation, promotes NO-mediated vasodilation) and FGF-2. The steps include:
- Vasodilation in response to NO and increased permeability from VEGF
- Pericyte detachment from the abluminal vessel surface
- Basement membrane degradation by matrix metalloproteinases (MMPs)
- Migration and proliferation of endothelial "tip" cells toward the injury
- Remodeling into capillary tubes
- Recruitment of pericytes (via PDGF) to stabilize new vessels
- Deposition of new basement membrane
c) Granulation Tissue Formation
The hallmark of the proliferative phase is the formation of granulation tissue - named for its pink, granular gross appearance. Histologically, it is characterized by:
- Proliferation of fibroblasts
- New thin-walled capillaries (angiogenesis)
- Loose ECM with scattered inflammatory cells (macrophages, lymphocytes)
- Minimal mature collagen at this stage
Fibroblasts proliferate and migrate into the wound, stimulated by PDGF and FGF. They synthesize collagen (initially type III, later replaced by type I) and glycosaminoglycans. TGF-β is the most potent fibrogenic stimulus and is the master regulator of ECM deposition.
Some fibroblasts differentiate into myofibroblasts (containing actin microfilaments), which mediate wound contraction - a major feature of healing by secondary intention. Contraction can reduce wound size by up to 80% in some wounds.
Phase 4 - Maturation / Remodeling (3 Weeks to ~1 Year)
In this final phase, the granulation tissue is gradually replaced by a relatively avascular scar. The key events are:
- Collagen remodeling: Type III collagen is replaced by stronger type I collagen
- MMP activity: MMPs (collagenases, gelatinases, stromelysins) degrade the existing ECM. They are produced as inactive zymogens and activated by plasmin at wound sites. Their activity is then shut off by TIMPs (tissue inhibitors of metalloproteinases)
- The balance between ECM synthesis (driven by TGF-β) and degradation (by MMPs inhibited by TIMPs) determines the final character of the scar
- Wound tensile strength increases progressively - reaching ~70-80% of normal skin strength by 3 months, but never returning to 100%
- The vasculature and cellularity of granulation tissue diminish progressively
Types of Wound Healing
Healing by Primary Intention (First Intention / Primary Union)
Occurs when wound edges are cleanly approximated (e.g., a sutured surgical incision). There is:
- Minimal tissue loss and destruction
- Narrow clot formation
- Limited inflammation
- Rapid re-epithelialization (within 24-48 hours)
- Minimal granulation tissue
- A small, neat hairline scar
Healing by Secondary Intention (Second Intention / Secondary Union)
Occurs in larger, infected, or gaping wounds where edges cannot be approximated. The process involves:
- A large clot fills the defect
- More intense inflammatory response
- Large amounts of granulation tissue
- Prominent wound contraction by myofibroblasts
- Re-epithelialization from wound edges over a wider area
- A broader, more prominent scar
Healing by Tertiary Intention (Delayed Primary Closure)
The wound is first cleaned and debrided, then closed later (after 4-5 days) once the infection is controlled. It combines features of both primary and secondary intention.
Repair by Regeneration vs. Scarring
The capacity for repair depends on cell type:
- Labile cells (continuously dividing - epithelium, hematopoietic cells): high regenerative capacity; contain stem cells that continuously replace lost cells
- Stable cells (quiescent but capable of division - hepatocytes, renal tubular cells, osteoblasts): can regenerate if the structural framework is intact
- Permanent cells (non-dividing - neurons, cardiac muscle, skeletal muscle): cannot regenerate; injury leads inevitably to scarring
Repair by scarring occurs when: the injured tissue cannot proliferate, or the connective tissue framework is damaged. It "patches" rather than restores tissue. The classic example is myocardial infarction, where cardiomyocytes (permanent cells) are replaced by collagen scar.
Factors Affecting Wound Healing
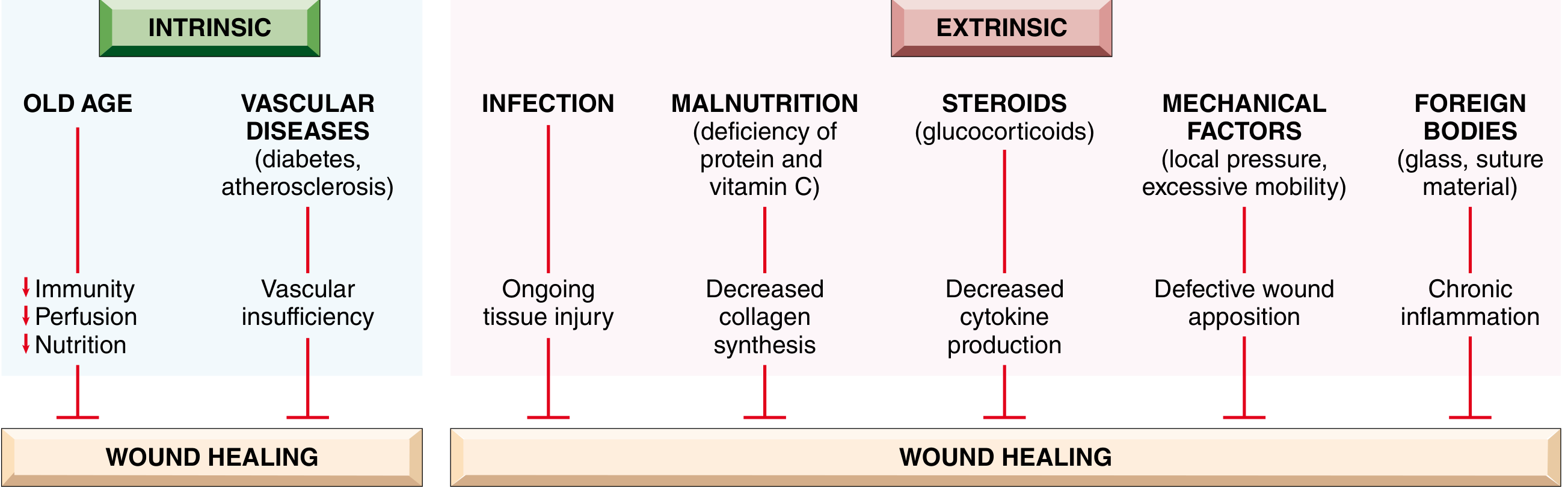
Systemic (Intrinsic) Factors:
- Old age: reduced immunity, perfusion, and nutrition
- Diabetes mellitus and vascular disease: impaired perfusion, neuropathy, ischemia
- Malnutrition: protein deficiency impairs collagen synthesis; Vitamin C deficiency inhibits collagen cross-linking and hydroxylation (scurvy)
- Glucocorticoids: decrease cytokine production, inhibit fibroblast proliferation and collagen synthesis, suppress inflammation (anti-fibrotic effect)
Local (Extrinsic) Factors:
- Infection: the single most important local factor; perpetuates inflammation and prevents healing
- Mechanical factors: excessive mobility, torsion, or pressure prevent wound edge apposition
- Foreign bodies: fragments of glass, steel, or suture material perpetuate chronic inflammation
- Poor perfusion: arterial disease, venous insufficiency, local ischemia
Abnormalities in Wound Healing
Deficient Scar Formation / Chronic Wounds
- Wound dehiscence: wound reopening; risk factors include obesity, malnutrition, infection, vascular insufficiency
- Chronic ulcers: venous leg ulcers (from venous hypertension/poor O₂ delivery), arterial ulcers (ischemia from atherosclerosis), diabetic ulcers (neuropathy + ischemia + infection), pressure sores (prolonged compression)
Excessive Scarring
- Hypertrophic scar: raised scar confined within wound boundaries; contains abundant myofibroblasts; may regress over time; common after thermal or traumatic injury
- Keloid: scar tissue that grows beyond the original wound boundary and does not regress; represents an individual predisposition; more common in darkly pigmented individuals
- Exuberant/proud flesh (Excessive granulation): excess granulation tissue protrudes above skin level, blocking re-epithelialization; must be removed by cautery or excision
Contractures
Exaggerated contraction of the wound leading to deformity; common after serious burns or extensive wounds.
Summary
Wound healing is a finely orchestrated, overlapping sequence of hemostasis, inflammation, proliferation, and remodeling. It involves a complex interplay of cells (platelets, neutrophils, macrophages, fibroblasts, endothelial cells), growth factors (VEGF, PDGF, TGF-β, FGF, EGF), the extracellular matrix, and MMPs/TIMPs. The type of healing (primary vs. secondary intention) depends on wound characteristics. The capacity for complete regeneration is limited to labile and stable cells; permanent cells undergo repair by scarring. Disruption of any phase - by local factors (infection, poor perfusion, foreign bodies) or systemic factors (diabetes, malnutrition, steroids, old age) - leads to impaired, delayed, or aberrant healing. Understanding these mechanisms is the foundation for all wound management in clinical surgery and medicine.
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th ed.), Ch. 3, pp. 103-115 | Sabiston Textbook of Surgery, Ch. 23 | Schwartz's Principles of Surgery, 11th ed.
This is a shared conversation. Sign in to Orris to start your own chat.