Awake craniotomy and SCALP BLOCK ( in detail ) for MD ANAESTHESIA PG EXAM - 30 marks major answer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"awake craniotomy" anaesthesia technique
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
I now have all the information needed for a comprehensive 30-mark answer. Let me compose it.
AWAKE CRANIOTOMY AND SCALP BLOCK
MD Anaesthesia PG Examination - Major Answer (30 Marks)
PART I: AWAKE CRANIOTOMY
1. Definition and Concept
Awake craniotomy is a neurosurgical procedure performed under monitored anaesthesia care (MAC) in which the patient remains conscious and responsive during the critical phase of cortical mapping, while being comfortable (sedated or anaesthetised) during painful non-mapping phases. It permits real-time neurophysiological assessment - speech, motor, sensory, and memory testing - while the surgeon resects the lesion.
2. Indications
- Tumour surgery near eloquent cortex: lesions adjacent to motor strip, speech areas (Broca's/Wernicke's), or sensory cortex
- Low-grade gliomas in or near language areas (dominant hemisphere) - evidence confirms awake mapping improves extent of resection with better neurological outcomes [PMID: 41398134, Systematic Review, 2025]
- Epilepsy surgery - resection of epileptic foci close to eloquent cortex; temporal lobe epilepsy with mesial involvement
- Deep brain stimulator placement (electrode testing)
- Resection of arteriovenous malformations near eloquent cortex
3. Contraindications
Absolute:
- Patient refusal
- Inability to cooperate (intellectual disability, severe anxiety, claustrophobia, psychosis)
- Paediatric age (generally not suitable below 10-12 years)
- Severe obstructive sleep apnoea (airway management impossible in fixed head)
- Language barrier (inability to communicate effectively)
Relative:
- Obesity (compromised airway, position intolerance)
- Chronic pain requiring high opioid doses
- Raised ICP with impending herniation
- Severe hearing/visual impairment (prevents testing)
- Uncontrolled seizures
4. Patient Selection and Preoperative Preparation
A motivated, cooperative patient is the single most critical factor for success.
Preoperative Assessment:
- Detailed psychological evaluation: assess anxiety levels, claustrophobia, cooperation ability
- Neuropsychological baseline: speech, motor, and cognitive assessment by a neuropsychologist
- Explanation of procedure: step-by-step description of what the patient will experience - this is the cornerstone of patient cooperation
- Practice runs: have the patient perform the tasks they will be asked to do intraoperatively (name objects, move hand, count)
- Optimise analgesia: address any pre-existing pain
- Anticonvulsants: if electrocorticography (ECoG) is planned, reduce or discontinue anticonvulsants as benzodiazepine premedication is avoided (interferes with EEG localisation)
- Antiemetic prophylaxis planning
Premedication:
- Anxiolytics used cautiously (benzodiazepines avoided if ECoG planned)
- Anticonvulsants adjusted per surgical plan
- Dexamethasone for brain oedema prophylaxis
5. Anaesthetic Techniques
Three principal approaches are used:
A. Monitored Anaesthesia Care (MAC) / Sedation-Only Technique
- Patient sedated throughout with spontaneous ventilation and unprotected airway
- Sedation depth titrated: deeper during painful phases (pin placement, skin incision, craniotomy), lighter during mapping
- Most popular for less invasive approaches
B. Asleep-Awake-Asleep (AAA) Technique
- Patient anaesthetised with LMA or ETT for initial craniotomy phase
- Airway device removed when brain is exposed (after dural opening)
- Patient awakens for cortical mapping
- Reanaesthetised and airway re-established for dural closure and skin closure
- LMA (particularly ProSeal or i-gel) preferred over ETT due to ease of insertion and removal
C. Conscious Sedation (Awake Throughout)
- Patient mildly sedated for all phases; no deep anaesthesia
- Scalp block is the primary analgesic technique
6. Drug Regimens for Sedation
The golden rule (Miller's Anesthesia, 10e): "The essential element of an anaesthetic for awake craniotomy is the local anaesthetic technique. Sedation cannot compensate for inadequate analgesia of the scalp."
Propofol (most commonly used)
- Target-controlled infusion (TCI) or manual infusion 25-75 mcg/kg/min
- Provides rapid titration, fast recovery
- Must be discontinued at least 15 minutes before EEG recording - it leaves a residual high-frequency beta activity that obscures abnormal EEG activity
Remifentanil
- Infusion at 0.02-0.05 mcg/kg/min, often combined with propofol
- Ultra-short-acting; provides analgesia during painful phases
- Risk: respiratory depression (synergistic with propofol) - requires vigilant monitoring
Dexmedetomidine (DEX) - increasingly preferred
- Alpha-2 agonist: sedation + anxiolysis + analgesia with minimal respiratory depression - key advantage
- Infusion: 0.1-0.5 mcg/kg/h during neurocognitive testing; loading dose 0.5-1 mcg/kg over 10 min
- Satisfactory conditions for speech mapping and ECoG reported at 0.1-0.2 mcg/kg/h during testing
- [PMID: 39079421, Meta-Analysis 2024]: DEX for awake craniotomy - lower respiratory depression vs propofol-remifentanil with comparable mapping efficacy
- Disadvantage: delayed recovery of responsiveness at higher doses
Propofol + Dexmedetomidine combination
- Dexmedetomidine as background infusion reduces propofol requirements
- Beneficial combination for longer procedures
Ketamine
- Low-dose ketamine (0.1-0.3 mg/kg IV) can be used as analgesic adjuvant
- Maintains airway reflexes; risk of dysphoria and hallucinations at higher doses
7. Intraoperative Monitoring
- Standard ASA monitors: ECG, SpO2, NIBP, temperature
- Arterial line (mandatory): continuous BP monitoring; arterial blood gases to detect hypercapnia
- Capnography: essential if deep sedation planned - confirms airway patency and respiratory drive breath by breath; end-tidal CO2 via nasal prongs
- Urinary catheter for long procedures
- EEG/electrocorticography (ECoG) setup
- Neuropsychological testing team presence
8. Painful Phases of Awake Craniotomy
Understanding the painful phases guides anaesthetic management:
| Phase | Pain Source | Intervention |
|---|---|---|
| Pin head holder placement | Periosteum, scalp | Scalp block + local infiltration at pin sites |
| Skin incision | Scalp | Scalp block |
| Bone flap elevation | Periosteum | Local infiltration + deeper sedation |
| Dural manipulation | Dura (pain-sensitive) | Surgeon infiltrates dura with LA; subtemporal dura especially painful |
| Brain parenchyma manipulation | Painless | - |
| Dural/skin closure | Scalp, dura | Re-sedation |
The brain itself is insensate. Pain comes from scalp, periosteum, and dura.
9. Intraoperative Management Pearls
- Head positioning: maximise neck flexion and atlanto-occipital extension before final head holder lockdown - this widens the margin for safe sedation with spontaneous ventilation. Once fixed, airway access is severely restricted
- Surgical drape: positioned to maintain direct, constant visual access to the patient's face (for speech testing, motor observation, and patient communication)
- Temperature management and pressure area padding: critical for long procedures; patient comfort = patient cooperation
- Communication: constant verbal reassurance throughout; explain each step
10. Cortical Mapping
- Surgeon applies bipolar electrical stimulation probe to the cortical surface
- Patient performs real-time neuropsychological tasks: naming objects, counting, moving limbs
- Positive mapping: stimulation causes interruption/abnormal response = eloquent cortex = no-resection zone
- Negative mapping: no response = safe to resect
- Speech (language) areas: predominantly left hemisphere (posterolateral temporal cortex, inferior frontal gyrus - Broca's area)
- Motor strip: pre-central gyrus; sensory strip: post-central gyrus
11. Complications of Awake Craniotomy
Intraoperative
- Intraoperative seizures - most common intraoperative complication
- Treatment: surgeon irrigates cortex with cold (ice-cold) saline first
- Propofol bolus 20 mg IV (Barash) or increments of 0.5-1.0 mg/kg (Miller)
- If persistent: phenytoin/levetiracetam IV
- Airway obstruction / respiratory depression - particularly dangerous in fixed head position
- Uncooperative or disinhibited patient ("awake patient failure") - anxiolysis, reassurance, may need conversion to GA
- Oversedation prohibiting neuropsychological testing
- Brain swelling / intractable oedema - poor surgical conditions
- Local anaesthetic systemic toxicity (LAST) - cumulative from scalp block + dural infiltration + surgeon's field block
- Pain - inadequate scalp block, surgical stimulation of dura
- Nausea and vomiting - routine antiemetics (ondansetron, dexamethasone) recommended
Postoperative
- Neurological deficit (transient or permanent)
- Cerebral oedema
- Haematoma
- Infection
- Post-procedure anxiety/PTSD
PART II: SCALP BLOCK
1. Concept and Importance
The scalp block is a regional anaesthesia technique that provides complete anaesthesia to the scalp by blocking the six to seven sensory nerves supplying it. It is the cornerstone of awake craniotomy analgesia - no amount of sedation can substitute for an adequate scalp block.
2. Anatomy of Scalp Innervation
The scalp receives sensory supply from two groups of nerves:
A. Branches of the Trigeminal Nerve (CN V) - Anterior/Lateral Scalp
| Nerve | Division | Area Supplied |
|---|---|---|
| Supratrochlear nerve | V1 (Ophthalmic) | Forehead medially, glabella to vertex |
| Supraorbital nerve | V1 (Ophthalmic) | Forehead laterally to lambdoid suture, central vertex |
| Zygomaticotemporal nerve | V2 (Maxillary) | Small area: temple, anterior temporal region |
| Auriculotemporal nerve | V3 (Mandibular) | Posterior temporal region, upper ear |
B. Cervical Spinal Nerves (C2-C3) - Posterior Scalp
| Nerve | Origin | Area Supplied |
|---|---|---|
| Greater occipital nerve | Dorsal ramus C2 | Posterior scalp from occiput to vertex (dominant supply) |
| Lesser occipital nerve | Ventral ramus C2 | Scalp behind the ear, lateral occiput |
| Great auricular nerve | Ventral rami C2-C3 | Lower ear, mastoid region, angle of jaw |
Mnemonic: "SCALP" / "Six Nerves" = Supratrochlear, Supraorbital, Auriculotemporal, Zygomaticotemporal, Greater occipital + Lesser occipital (+ Great auricular = 7th)
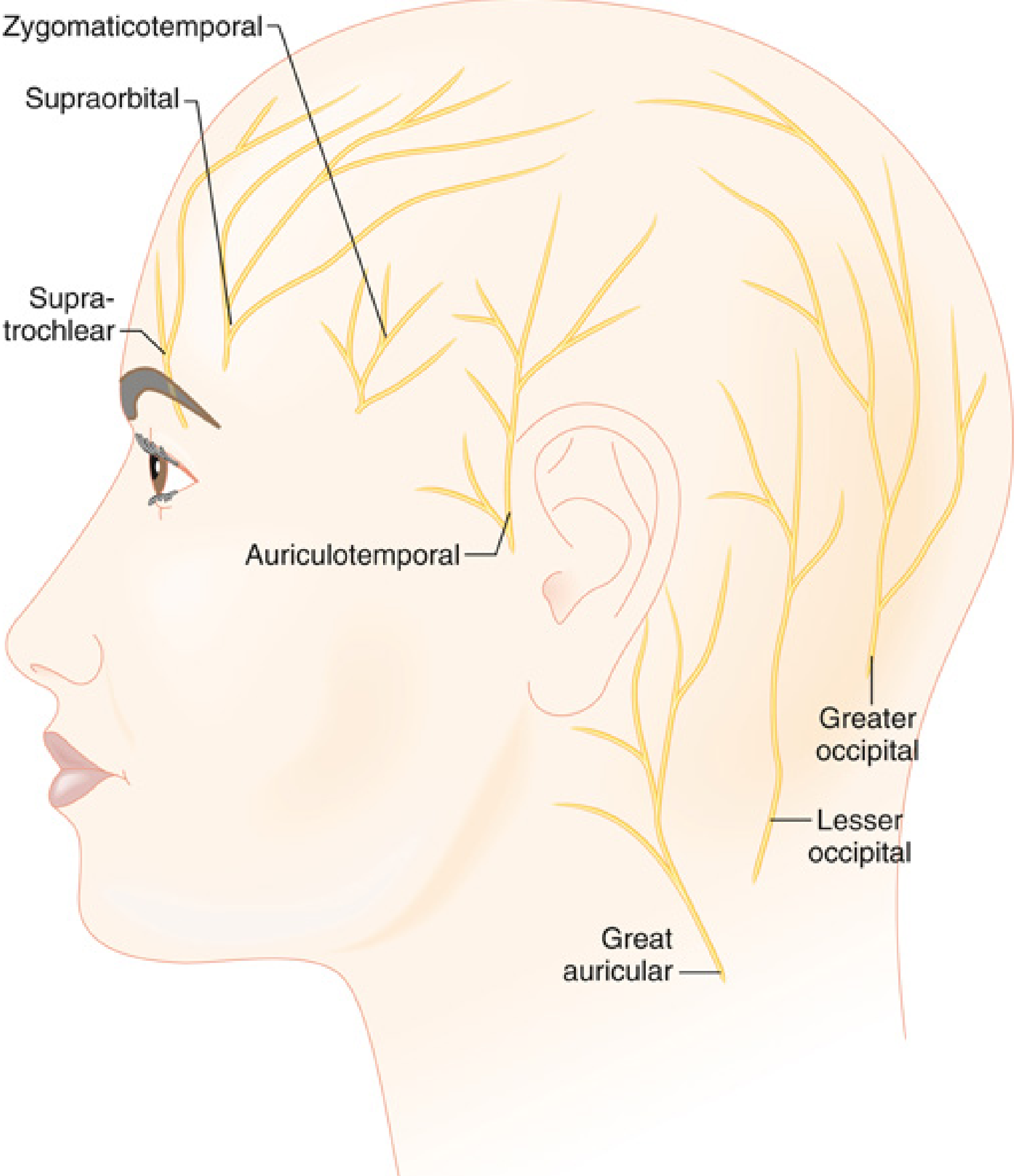
Fig: Cutaneous nerves of the scalp showing supratrochlear, supraorbital, zygomaticotemporal, auriculotemporal, greater occipital, lesser occipital, and great auricular nerves - Miller's Anesthesia 10e
3. Techniques of Scalp Block
Option A: Individual Nerve Block Technique (Selective/Classic)
Each of the 6-7 nerves is blocked at a specific anatomical landmark. More precise but time-consuming.
1. Supratrochlear Nerve:
- Landmark: superomedial aspect of orbit, medial to supraorbital notch, near trochlea
- Technique: 2-3 mL LA injected subcutaneously at medial end of eyebrow / superomedial orbital rim
2. Supraorbital Nerve:
- Landmark: supraorbital notch/foramen (palpable on superior orbital rim, approximately in line with the pupil)
- Technique: 3-5 mL LA injected at notch/foramen; needle directed superiorly
3. Zygomaticotemporal Nerve:
- Landmark: lateral orbital rim / temporal fossa, just lateral to zygomaticofrontal suture line
- Technique: 2 mL LA injected subcutaneously in temporal fossa above the zygomatic arch
4. Auriculotemporal Nerve:
- Landmark: pre-auricular region, 1.5 cm anterior to the tragus, at the level of the zygomatic arch
- Technique: 3 mL LA injected subcutaneously anterior to the tragus (caution: superficial temporal artery nearby)
5. Greater Occipital Nerve:
- Landmark: nuchal line; palpate the occipital artery at the superior nuchal line - the greater occipital nerve lies medial to the occipital artery, approximately one-third of the way from the external occipital protuberance to the mastoid process
- Technique: 3-5 mL LA injected medial to the pulsating occipital artery, aspirate first (close to artery)
6. Lesser Occipital Nerve:
- Landmark: 2.5-3.5 cm lateral and 1-2 cm caudal to the greater occipital nerve at the nuchal line
- Technique: 2-3 mL LA injected subcutaneously at this point
7. Great Auricular Nerve:
- Landmark: posterior to the ear, at the mastoid process
- Technique: 2-3 mL LA injected subcutaneously posterior to the auricle/mastoid region
Option B: Circumferential Ring Block Technique (Field Block)
- A practical alternative requiring less anatomical precision
- A ring of local anaesthetic is infiltrated circumferentially above an imaginary line drawn from the external occipital protuberance to the eyebrows, passing along the upper border of the ear
- This line encircles all nerve entry points into the scalp
- All scalp nerves become superficial and accessible above this line
- Volume required: approximately 30 mL of LA solution (with epinephrine 1:200,000)
- Injections made subcutaneously using a long 22-gauge needle advanced along the scalp
4. Local Anaesthetic Choice and Dosing
| Agent | Concentration | Onset | Duration |
|---|---|---|---|
| Bupivacaine 0.25-0.5% | With adrenaline 1:200,000 | Moderate (10-15 min) | 4-8 hours (preferred for long craniotomies) |
| Ropivacaine 0.375-0.5% | With or without adrenaline | Moderate | 4-6 hours (less cardiotoxic) |
| Lidocaine 1-2% | With adrenaline 1:200,000 | Fast (5 min) | 2-3 hours |
| Levobupivacaine 0.25-0.5% | With adrenaline | Moderate | 4-6 hours |
Mixture strategy: Lidocaine (fast onset) + Bupivacaine (long duration) mixture often used
Adrenaline (epinephrine) 1:200,000:
- Mandatory addition (unless contraindicated)
- Vasoconstriction reduces bleeding, decreases systemic absorption, prolongs block duration
- Alerts to inadvertent intravascular injection (tachycardia)
Total Volume: 20-40 mL for a complete scalp block
5. Local Anaesthetic Toxicity - Critical Concern
This is the major risk because multiple LA injections are cumulative:
- Scalp block by anaesthesiologist
- Pin site infiltration (4-6 pin sites) by anaesthesiologist/surgeon
- Dural infiltration by surgeon (dura is pain-sensitive)
- Incision field block by surgeon
Anesthesiologist must:
- Track cumulative LA dose throughout the procedure
- Communicate with surgeon regarding remaining safe dose
- Use maximum doses: Bupivacaine with adrenaline = 3 mg/kg (max ~225 mg in 70 kg adult)
- Ropivacaine with adrenaline = 3.5-4 mg/kg
- Lidocaine with adrenaline = 7 mg/kg
LAST management: Lipid emulsion 20% (Intralipid) must be immediately available
6. Additional Pin Site and Dural Analgesia
- Pin sites (Mayfield clamp): 5-10 mL of 1% lidocaine or 0.25% bupivacaine infiltrated at each pin site before application - this is the most acutely painful moment
- Dural infiltration: surgeon infiltrates dura directly, especially the middle meningeal artery region and along subtemporal dura (most pain-sensitive portion)
- Periosteal infiltration: along incision line before skin incision
7. Timing of Scalp Block
- Performed before skin preparation and head pinning
- Allow adequate onset time before pin placement (10-15 minutes for bupivacaine)
- Can be performed bilaterally (unilateral block for unilateral craniotomy; bilateral if required)
- Often performed while patient is lightly sedated to improve comfort during injection
8. Advantages of Scalp Block in Awake Craniotomy
- Reduces intraoperative pain and sedation requirements
- Attenuates haemodynamic responses to painful stimuli (pin insertion, skin incision)
- Reduces propofol and opioid consumption - better neurological testing conditions
- Reduces brain swelling (less coughing, less sympathetic stimulation → less ICP elevation)
- Reduces postoperative pain - scalp block with LA significantly reduces post-craniotomy pain scores (Miller's Anesthesia)
- Reduces PONV (reduced opioid use)
- Facilitates earlier recovery and mobilisation
9. Complications of Scalp Block
| Complication | Prevention/Management |
|---|---|
| Intravascular injection (most important) | Aspirate before each injection; use adrenaline as marker; use incremental injection |
| Local anaesthetic systemic toxicity (LAST) | Dose tracking, lipid emulsion available |
| Haematoma at injection site | Careful technique; aspiration; avoid superficial temporal artery |
| Inadequate block | Ensure correct landmarks; adequate volume; correct planes (subcutaneous) |
| Adrenaline adverse effects | Caution in ischaemic heart disease, severe HTN |
| Infection | Aseptic technique |
PART III: INTEGRATED ANAESTHETIC PLAN FOR AWAKE CRANIOTOMY
Step-by-Step Protocol
Preoperative:
- Thorough counselling and consent
- NPO as standard
- Establish IV access (large bore), arterial line
- Antiemetic prophylaxis: dexamethasone 8 mg + ondansetron 4 mg
- Urinary catheter
Induction/Sedation Phase (Asleep):
- Propofol TCI or infusion (± dexmedetomidine loading 0.5-1 mcg/kg over 10 min)
- Insert LMA (AAA technique)
- Patient positioned with adequate padding, face visible
- Scalp block performed: all 6-7 nerves blocked; pin site infiltration
- Allow 15 min onset time
- Head pinned (Mayfield), head positioned
Awake/Mapping Phase:
- Propofol discontinued (at least 15 min before EEG)
- LMA removed (AAA) or sedation lightened (MAC)
- Dexmedetomidine at 0.1-0.2 mcg/kg/h if continued
- Neuropsychological testing + cortical mapping by surgeon
- Cold saline available at field for seizure management
- Propofol bolus 20 mg at hand for seizure management
Re-Sleep Phase (Closure):
- Propofol/remifentanil infusion restarted
- LMA re-inserted (AAA)
- Surgical closure
- Emergence, PACU/ICU as per standard craniotomy protocol
Summary Table: Key Points for Exam
| Topic | Key Point |
|---|---|
| Indication | Eloquent cortex tumour, epilepsy surgery |
| Essential element | Scalp block - sedation cannot substitute |
| Best sedation agent | Dexmedetomidine (minimal respiratory depression) |
| Scalp nerves blocked | Supratrochlear, Supraorbital, Zygomaticotemporal, Auriculotemporal, Greater/Lesser occipital, Great auricular (6-7) |
| Circumferential block volume | ~30 mL with epinephrine 1:200,000 |
| Intraoperative seizure Rx | Cold saline → Propofol 20 mg IV bolus |
| Propofol stop before EEG | At least 15 minutes |
| Major LA toxicity concern | Cumulative doses: scalp block + pins + dura |
| Brain parenchyma pain | Painless - only scalp, periosteum, dura are painful |
| Key monitoring | Arterial line + capnography mandatory |
References:
- Miller's Anesthesia, 10th Ed. (Elsevier) - Awake Craniotomy and Seizure Surgery, Ch. 53; Scalp Blocks, Ch. 74
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th Ed. - Awake Craniotomy
- Roberts & Hedges' Clinical Procedures in Emergency Medicine - Scalp Block Technique
- [PMID 39079421] Akavipat et al. Dexmedetomidine for awake craniotomy: Systematic Review & Meta-Analysis. J Clin Neurosci. 2024
- [PMID 41398134] Sadhasivam et al. Awake mapping and outcomes in low-grade gliomas: Systematic Review. Neurosurg Rev. 2025
This is a shared conversation. Sign in to Orris to start your own chat.