Can Cautery be used for gingivectomy and crown lengthening procedures
electrosurgery gingivectomy crown lengthening
electrocautery electrosurgery gingivectomy crown lengthening indications contraindications
https://www.gijhsr.com/GIJHSR_Vol.8_Issue.2_April2023/GIJHSR…
Can Cautery (Electrosurgery) Be Used for Gingivectomy and Crown Lengthening?
- Gingivectomy
- Gingivoplasty
- Crown lengthening
- Frenectomy
- Operculectomy
- Depigmentation
- Gingival curettage
- Periodontal flap procedures
- Mucogingival surgeries
- Implantology procedures
Use in Gingivectomy
- Patients with a bleeding tendency or on anticoagulants (immediate hemostasis is the key advantage)
- Fibrous/hyperplastic tissue - electrosurgery handles firm/fibrotic tissue well
- When suture-free healing is desired (wounds heal by secondary intention)
- Areas with limited access where a scalpel is awkward
Use in Crown Lengthening
- When osseous recontouring is needed (bone needs reshaping), a flap procedure with a scalpel is required - electrosurgery cannot be used near bone
- Crown lengthening that requires bone removal must use a flap + rotary instruments/chisels; electrosurgery only addresses soft tissue
Advantages of Electrosurgery in These Procedures
| Advantage | Notes |
|---|---|
| Minimal intraoperative bleeding | Clear surgical field, improved visibility |
| Precise, pressureless incisions | Less tissue trauma vs. scalpel pressure |
| No sutures needed | Healing occurs by secondary intention |
| Shorter chair time | Less operator fatigue |
| Access to difficult areas | Needle electrode fits tight embrasures |
| Soft tissue contouring (gingivoplasty) | Smooth gingival margins possible |
Disadvantages and Risks
| Disadvantage | Notes |
|---|---|
| Bone necrosis if electrode contacts bone | Must maintain safe distance from alveolar bone |
| Delayed healing vs. scalpel | Lateral thermal damage slows regeneration |
| Unpleasant burning odor | High-volume suction required |
| High equipment cost | Initial investment |
| Restricted use near restorations | Can damage crowns, metal margins |
| Post-op discomfort | More than scalpel in some studies |
Contraindications (Absolute / Relative)
- Patients with cardiac pacemakers - electromagnetic interference risk (absolute contraindication)
- Near inflammable anesthetic gases
- When the electrode tip could contact bone - risk of necrosis
- When osseous recontouring is simultaneously required - a flap approach is mandatory
- Inadequate keratinized tissue - if gingivectomy would eliminate the attached gingiva (Maynard and Wilson recommend maintaining at least 3 mm of attached gingiva)
Key Clinical Rule
Electrosurgery for gingivectomy/crown lengthening is appropriate only when the procedure is confined to soft tissue, there is no need for osseous recontouring, and adequate bone distance (≥3 mm) exists. When bone recontouring is required, a full-thickness flap with conventional instruments remains the standard of care.
Create a clinical decision tree: when to use scalpel vs electrosurgery vs laser for gingivectomy
scalpel vs electrosurgery vs laser gingivectomy clinical selection criteria comparison
A detailed clinical decision tree flowchart titled "Gingivectomy: Scalpel vs Electrosurgery vs Laser — Clinical Decision Guide". Clean white background, professional medical style with clear boxes and arrows. START at the top: "Patient Requires Gingivectomy" (dark teal header box) First branch question box: "Does the patient have a cardiac pacemaker or implanted electrical device?" - YES arrow → "LASER or SCALPEL only — Electrosurgery contraindicated" (red warning box) - NO arrow → continue down Second branch: "Is osseous recontouring (bone reshaping) required?" - YES arrow → "SCALPEL + Flap procedure — Neither laser nor electrosurgery near bone" (blue box) - NO arrow → continue Third branch: "Is bone crest less than 3mm from planned gingival margin?" - YES arrow → "SCALPEL preferred — Risk of thermal bone damage with laser/electrosurgery" (blue box) - NO (≥3mm clearance) arrow → continue Fourth branch: "Does patient have significant bleeding tendency / on anticoagulants?" - YES arrow → "ELECTROSURGERY or LASER — Superior hemostasis" (green box) - NO arrow → continue Fifth branch: "Is tissue fibrotic or hyperplastic (drug-induced, orthodontic)?" - YES arrow → three sub-boxes side by side: "LASER — Best outcomes, less post-op discomfort" (green) | "ELECTROSURGERY — Good for fibrotic tissue" (amber) | "SCALPEL — Standard option"(blue) - NO (normal/thin gingiva) arrow → continue Sixth branch: "Is aesthetic precision the priority (anterior teeth, smile line)?" - YES arrow → "LASER — Most precise, minimal thermal spread, best aesthetics" (green preferred box) - NO arrow → continue Final box at bottom: "Routine gingivectomy, no special constraints" → three equal outcome boxes: "SCALPEL — Gold standard, predictable healing, histology available" (blue) | "ELECTROSURGERY — Good hemostasis, suture-free, cost moderate" (amber) | "LASER — Least discomfort, bactericidal, higher equipment cost" (green) Bottom summary bar with three color-coded columns: SCALPEL (blue) — best when: osseous work needed, bone proximity, histologic specimen required, standard cases. ELECTROSURGERY (amber) — best when: bleeding tendency, fibrotic tissue, suture-free desired, no pacemaker. LASER (green) — best when: aesthetics priority, anxious patient, anticoagulated, bactericidal effect needed, pacemaker present. Professional clinical diagram style, readable fonts, color-coded arrows (blue=scalpel, amber=electrosurgery, green=laser), clean layout.
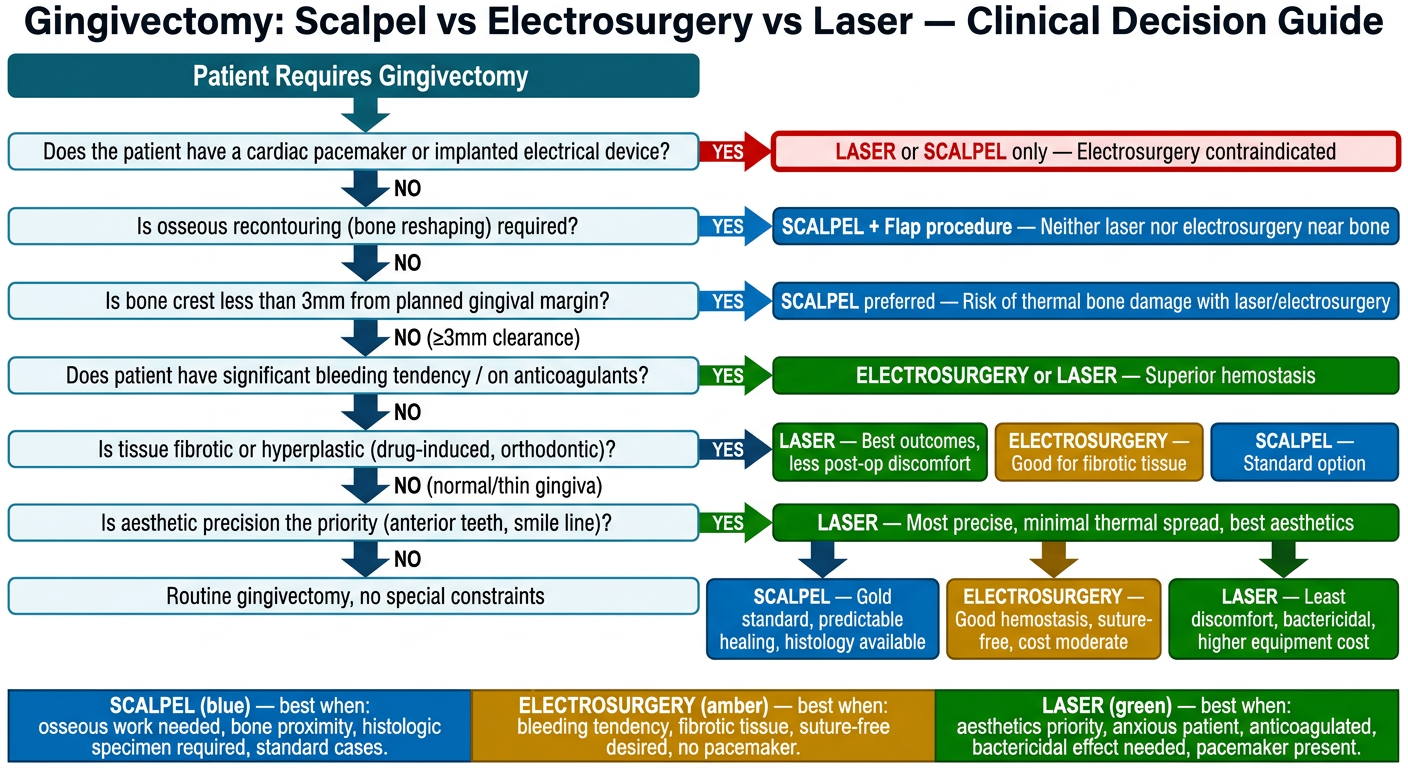
Step-by-Step Decision Logic
| Clinical Question | Answer | Instrument Choice |
|---|---|---|
| Cardiac pacemaker present? | YES | Laser or Scalpel only - no electrosurgery |
| Osseous recontouring needed? | YES | Scalpel + flap - no thermal devices near bone |
| Bone crest < 3mm from planned margin? | YES | Scalpel preferred - thermal injury risk too high |
| Significant bleeding / anticoagulated? | YES | Electrosurgery or Laser - superior hemostasis |
| Fibrotic / hyperplastic tissue? | YES | Laser (first choice) > Electrosurgery > Scalpel |
| Anterior aesthetics / precision priority? | YES | Laser - tightest thermal control, best contour |
| Routine case, no special constraints? | - | Any of the three (scalpel = gold standard default) |
Quick Summary: When Each Tool Wins
- Osseous recontouring required (flap surgery)
- Bone proximity < 3mm
- Histologic specimen needed (biopsy)
- Standard, uncomplicated cases
- Best predictable long-term healing data
- Active bleeding / anticoagulated patient
- Fibrotic or drug-induced gingival enlargement
- Suture-free closure desired
- Short chair time priority
- NOT if: pacemaker, bone proximity, flap needed
- Aesthetic zone - anterior smile line
- Anxious or needle-phobic patients (less post-op pain)
- Anticoagulated patients (comparable hemostasis to electrosurgery)
- Pacemaker present (safe - no electromagnetic interference)
- Bactericidal effect desired (infected/inflamed tissue)
- Pediatric patients