Early and late toxicoses in pregnancy definition, etiology, pathogenesis, clinical factors, treatment and management
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
preeclampsia pathogenesis treatment management
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full response.
Toxicoses of Pregnancy: Early and Late
The term "toxicosis of pregnancy" (also called "toxemia of pregnancy") historically refers to a group of pregnancy-specific disorders characterized by systemic dysfunction. They are divided into early toxicosis (first trimester, primarily nausea/vomiting - hyperemesis gravidarum) and late toxicosis (second/third trimester, primarily hypertensive disorders - gestational hypertension, preeclampsia, eclampsia, and HELLP syndrome).
PART I: EARLY TOXICOSIS - Nausea, Vomiting, and Hyperemesis Gravidarum
Definition
- Nausea and vomiting of pregnancy (NVP): Nausea and/or vomiting occurring in up to 70-90% of pregnancies, typically starting at 4-6 weeks, peaking at 8-12 weeks, and resolving by week 20.
- Hyperemesis gravidarum: The severe end of the spectrum - intractable vomiting with weight loss (>5% of pre-pregnancy weight), volume depletion, ketonuria, and electrolyte disturbances. Occurs in 0.3-3% of all pregnancies.
Etiology
The etiology is multifactorial:
| Factor | Details |
|---|---|
| Hormonal | HCG peaks coincide with worst symptoms; conditions with elevated HCG (multiple gestation, trophoblastic disease, trisomy 21) have higher incidence |
| Estrogen/Progesterone | Alter gastric motility and slow GI transit time |
| Thyroid | HCG has TSH-like activity - transient gestational thyrotoxicosis in 2/3 of hyperemesis cases |
| Gut hormones | Ghrelin and leptin implicated |
| H. pylori infection | Two meta-analyses confirm increased risk; some symptomatic improvement after eradication |
| Psychosocial | Stress, anxiety, psychological factors |
| Genetic | Familial clustering suggests predisposition |
Risk factors include: personal/family history of hyperemesis, female fetus, multiple gestation, gestational trophoblastic disease, fetal trisomy 21, hydrops fetalis.
Pathogenesis
Pregnancy hormones (primarily HCG and estrogen) impair gastric motility, slow GI transit, and alter chemoreceptor trigger zone sensitivity. Vomiting episodes are often triggered by olfactory, auditory, and visual stimuli. The PUQE score (pregnancy-unique quantification of nausea and emesis) can quantify severity.
Clinical Features
- Nausea and vomiting, typically morning-predominant but can occur any time
- Physical exam: usually normal except signs of volume depletion (tachycardia, hypotension, poor skin turgor)
- Hyperemesis: ketonuria, hypokalemia, hyponatremia, elevated aminotransferases (25-40% of cases), hyperamylasemia (from salivary glands, ~25%)
- Abdominal pain is NOT a feature - if present, consider other diagnoses
Differential diagnosis: Cholecystitis/cholelithiasis, gastroenteritis, pancreatitis, appendicitis, hepatitis, peptic ulcer, pyelonephritis, ectopic pregnancy, acute fatty liver of pregnancy, HELLP syndrome.
Severe complications (rare): Mallory-Weiss tears, Boerhaave syndrome, Wernicke encephalopathy/Korsakoff psychosis, central pontine myelinolysis, retinal hemorrhage, spontaneous pneumomediastinum.
Fetal effects: Infants of women with weight gain <7 kg are at increased risk for low birth weight, prematurity, small for gestational age, and low Apgar scores.
Treatment and Management
Step 1 - Dietary modification:
- Small, frequent meals; avoid empty stomach
- Separate solid and liquid intake
- High-carbohydrate diet
- Avoid offensive odors
Step 2 - Pharmacotherapy (outpatients):
- Ginger - helpful, safe
- Pyridoxine (Vitamin B6) - first-line
- Doxylamine + pyridoxine (Diclegis/Diclectin) - re-introduced after initial teratogenicity concerns were refuted; no increased fetal risk
- Phenothiazines (promethazine, prochlorperazine, chlorpromazine) - effective; side effects: drowsiness, dystonic reactions
- Metoclopramide - dopamine antagonist; beneficial
- Ondansetron (Zofran) - 5-HT3 antagonist; 8 mg IV or 4 mg PO TID; no dystonia; good safety profile
Step 3 - Hospital admission indications:
- Persistent vomiting after outpatient therapy
- Weight loss >10% of pre-pregnancy weight
- Persistent ketonuria/electrolyte abnormalities after IV rehydration
- Uncertain diagnosis
- Severe dehydration, hypotension, tachycardia
Inpatient management:
- IV fluids: 5% dextrose in lactated Ringer's or normal saline
- Nothing by mouth initially; advance to oral fluids once controlled
- IV antiemetics
- Electrolyte replacement
- Thiamine (to prevent Wernicke encephalopathy)
- Nutritional support (enteral/parenteral in refractory cases) - note: ~50% catheter complication rate due to hypercoagulability of pregnancy
Discharge criteria: Resolution of ketonuria, correction of electrolyte imbalance, tolerating oral fluids.
PART II: LATE TOXICOSIS - Hypertensive Disorders of Pregnancy
Definition and Classification
Late toxicosis encompasses a spectrum:
- Gestational hypertension: New-onset BP ≥140/90 mmHg after 20 weeks without proteinuria or systemic features
- Preeclampsia: New-onset hypertension + proteinuria and/or systemic organ dysfunction, after 20 weeks
- Preeclampsia with severe features: BP ≥160/110 mmHg, or severe organ involvement
- Eclampsia: Preeclampsia + new-onset seizures (tonic-clonic convulsions) not explained by another cause
- HELLP syndrome: Hemolysis + Elevated Liver enzymes + Low Platelets - a severe variant of preeclampsia
Incidence: ~8.5% of all deliveries in the US. Preeclampsia affects 3-5% of pregnant women and is more common in nulliparas.
Etiology and Risk Factors
| Risk Category | Specific Factors |
|---|---|
| Obstetric | Nulliparity (32.3% population-attributable fraction), prior preeclampsia, multiple gestation, molar pregnancy, IVF conception |
| Medical | Chronic hypertension (25% develop superimposed preeclampsia), chronic renal disease, pregestational diabetes (20% risk overall; up to 70% in classes F/R), systemic lupus erythematosus, antiphospholipid syndrome |
| Demographic | Extremes of maternal age, non-White race (associated with severity more than incidence), family history |
| Other | Obesity, chronic kidney disease, connective tissue disorders |
Pathogenesis
The central mechanism is failed trophoblast invasion and inadequate spiral artery remodeling:
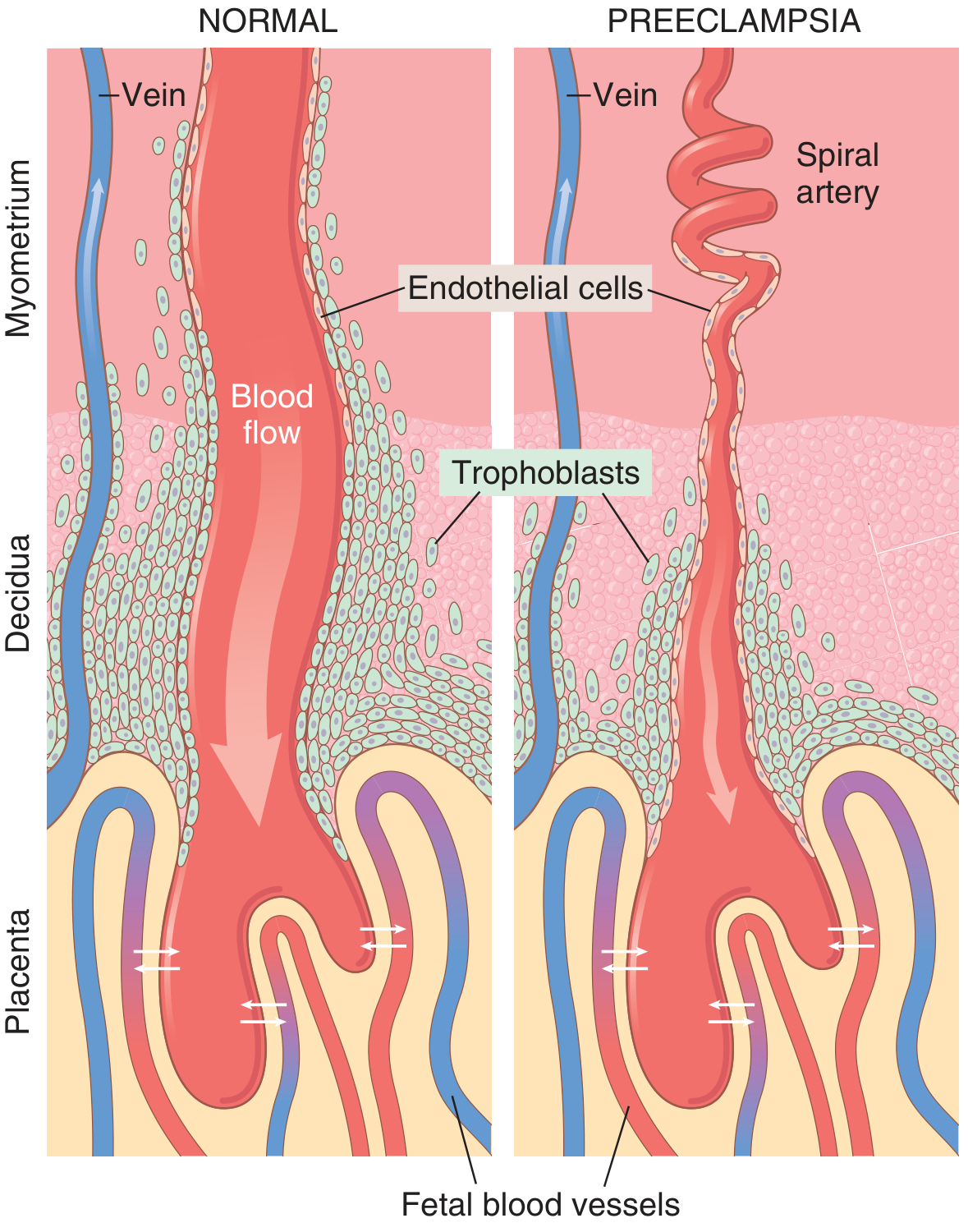
Normal vs. preeclampsia: In normal pregnancy, trophoblasts invade and remodel spiral arteries into wide, low-resistance sinusoids. In preeclampsia, this remodeling fails - the spiral arteries remain narrow and high-resistance, causing placental ischemia.
Step-by-step cascade:
- Failed trophoblast invasion - Spiral arteries retain their musculoelastic walls and remain narrow instead of being remodeled into wide sinusoids
- Placental ischemia/hypoxia - Reduced uteroplacental blood flow results in placental hypoxia and dysfunction
- Release of anti-angiogenic factors - The ischemic placenta releases:
- Soluble fms-like tyrosine kinase-1 (sFlt-1) - antagonizes VEGF
- Soluble endoglin - antagonizes TGF-β
- Inflammatory cytokines (TNF-α, IL-6)
- Maternal endothelial dysfunction - These circulating factors impair vascular endothelium throughout the body, leading to:
- Reduced production of vasodilators (prostacyclin/PGE2) → Hypertension
- Increased thromboxane A2 → vasoconstriction
- Endothelial hyperpermeability → Edema, proteinuria
- Activation of coagulation → Hypercoagulability, thrombocytopenia
- Reduced GFR with glomerular endotheliosis → Renal dysfunction
Morphological changes include:
- Placental infarcts, retroplacental hemorrhage
- Increased syncytial knots (ischemic change)
- Acute atherosis: fibrinoid necrosis + lipid-laden macrophages in decidual vessels
- Glomerular endotheliosis: swollen endothelial cells obliterating capillary lumen
- Brain: PRES (posterior reversible encephalopathy syndrome) on MRI - bilateral signal abnormality in occipital white matter
Clinical Features
Onset: Usually after 34 weeks; earlier with hydatidiform mole, preexisting kidney disease, hypertension, or coagulopathy.
Classic triad: Hypertension + Edema + Proteinuria (though proteinuria is no longer mandatory for diagnosis)
Symptoms and signs:
- Hypertension (BP ≥140/90 mmHg on two occasions ≥4 hours apart)
- Edema (particularly non-dependent - face, hands)
- Headache, visual disturbances (blurred vision, scotomata)
- Epigastric/right upper quadrant pain (hepatic capsule distension)
- Nausea and vomiting
- Oliguria
- Pulmonary edema (in severe cases)
- Petechiae/bruising (with DIC)
Severe features (any of the following):
- Systolic BP ≥160 mmHg or diastolic BP ≥110 mmHg (persistent ≥15 min)
- Thrombocytopenia (<100,000/μL)
- Renal insufficiency (creatinine >1.1 mg/dL)
- Impaired liver function (AST/ALT ≥2x upper limit of normal)
- Pulmonary edema
- New-onset headache unresponsive to medication
- Visual disturbances
HELLP Syndrome:
- Microangiopathic hemolytic anemia (schistocytes on peripheral smear)
- AST/ALT elevated (but typically <500 U/L, unlike viral hepatitis)
- Platelets <100,000/μL (or <150,000 suspicious)
- LDH >600 U/L
- Total bilirubin >1.2 mg/dL
- More common in multigravid women; hypertension may be absent initially
- Presents with epigastric/RUQ pain - easily confused with cholecystitis, hepatitis, pancreatitis
Eclampsia: Tonic-clonic seizures, coma; vascular spasm throughout body; may occur antepartum, intrapartum, or postpartum
Laboratory Evaluation
| Test | Finding |
|---|---|
| Urinalysis | Proteinuria (≥300 mg/24h or protein:creatinine ≥0.3) |
| CBC | Thrombocytopenia, schistocytes (in HELLP/DIC) |
| Serum uric acid | Elevated early (sensitive marker of preeclampsia) |
| Serum creatinine | Elevated in severe disease |
| AST/ALT | Elevated with hepatic involvement |
| Coagulation profile | May show DIC |
| LDH | Elevated in hemolysis |
Treatment and Management
Definitive treatment: Delivery - The only cure for preeclampsia. All other therapy is temporizing.
Antihypertensive Therapy
Acute severe hypertension (BP >160/110 mmHg confirmed over 15 minutes) requires treatment within 1 hour to prevent intracranial hemorrhage.
| Drug | Mechanism | Onset | Dose | Notes |
|---|---|---|---|---|
| Labetalol | α + nonselective β antagonist | 5 min | 20 mg IV, then 40-80 mg q10 min; max 300 mg | Less hypotension/reflex tachycardia than hydralazine |
| Hydralazine | Arterial vasodilator | 10-20 min | 5-10 mg IV q20 min | Risk of maternal hypotension |
| Nifedipine | Calcium channel blocker | 10-20 min | 10-20 mg PO; repeat q30 min | Oral route; avoid sublingual |
NOT recommended: Sodium nitroprusside (fetal cyanide toxicity), diazoxide (metabolic effects), ACE inhibitors (contraindicated in pregnancy).
NOT beneficial: Strict sodium restriction, routine diuretics (worsen volume depletion - use only for pulmonary edema).
Seizure Prophylaxis - Magnesium Sulfate
Standard of care for prevention and treatment of eclamptic seizures.
- Loading dose: 4-6 g IV over 15-20 minutes
- Maintenance: 1-2 g/hour IV continuous infusion
- For eclampsia: Same loading dose; MgSO4 is superior to phenytoin and diazepam
- Recommended for all women with preeclampsia with severe features (intrapartum and 24-48 hours postpartum)
- Monitor for toxicity: loss of deep tendon reflexes, respiratory depression, cardiac arrest (antidote: calcium gluconate 1g IV)
Delivery Decisions
| Gestational Age | Clinical Situation | Recommendation |
|---|---|---|
| ≥37 weeks (any) | Preeclampsia (with or without severe features) | Prompt delivery |
| 34-37 weeks | Severe features | Delivery after stabilization with steroids |
| <37 weeks | Without severe features, reassuring fetal testing | Expectant management with close monitoring |
| Any | HELLP, eclampsia, non-reassuring fetal status | Prompt delivery |
Expectant management (for preterm without severe features): Weekly BP monitoring, CBC, liver enzymes, creatinine; weekly fetal NST/BPP; fetal growth every 3 weeks; admit vs. outpatient depending on reliability and severity. Antenatal corticosteroids if <34 weeks.
Postpartum: Continue magnesium sulfate 24-48 hours postpartum. BP may remain elevated for 7-10 days. Proteinuria and hypertension usually resolve within 1-2 weeks after delivery.
Prevention
- Low-dose aspirin (81 mg/day) starting at 12-16 weeks for women with ≥1 high-risk factor - reduces incidence and complications
- Calcium supplementation in calcium-deficient populations
- No benefit from: vitamins C and E, strict bed rest, sodium restriction
Prognosis
- Hypertension and proteinuria typically resolve within 1-2 weeks postpartum
- Perinatal mortality is 1.4-2.7x higher in preeclamptic pregnancies
- Maternal mortality from: intracranial hemorrhage (undertreated severe hypertension), hepatic rupture (HELLP), eclampsia complications
- Long-term: Women who had preeclampsia have significantly increased lifetime risk of hypertension, stroke, ischemic heart disease, and renal disease
- Women with HELLP and superimposed preeclampsia on chronic hypertension have the highest risk for severe complications
Summary Comparison
| Feature | Early Toxicosis (Hyperemesis) | Late Toxicosis (Preeclampsia/Eclampsia) |
|---|---|---|
| Timing | Weeks 4-20 (first trimester) | After 20 weeks (usually >34 weeks) |
| Core mechanism | HCG/estrogen-driven dysmotility | Failed trophoblast invasion → endothelial dysfunction |
| Main symptoms | Nausea, vomiting, dehydration | Hypertension, proteinuria, edema, seizures |
| Diagnostic hallmark | Ketonuria, weight loss >5% | BP ≥140/90 + proteinuria/organ dysfunction |
| Definitive treatment | Supportive (IV fluids, antiemetics) | Delivery |
| Key drug | Ondansetron/pyridoxine-doxylamine | Magnesium sulfate + antihypertensives |
| Recurrence | Frequently recurs in subsequent pregnancies | Increases risk in future pregnancies |
Sources: Creasy & Resnik's Maternal-Fetal Medicine 8e; Robbins & Kumar Basic Pathology; Guyton & Hall Medical Physiology 14e; Tintinalli's Emergency Medicine; Sleisenger & Fordtran's Gastrointestinal and Liver Disease
What is Bishop score and how is it useful in monitoring pregnancy?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Searching PubMed
"Bishop score" cervical assessment labor induction
I now have all the information needed for a thorough answer.
The Bishop Score
Background and Origin
The Bishop Pelvic Scoring System was developed by Dr. Edward Bishop in 1964 (Obstet Gynecol. 1964;24:266) as an objective, standardized tool to assess cervical readiness for labor induction. Before this, the decision to induce labor was largely subjective. Bishop's scoring system quantified the likelihood of successful vaginal delivery and has since become one of the most widely used tools in obstetrics.
The Score: Five Parameters
The Bishop score assesses five components of the cervix and fetal station on digital vaginal examination. Points are assigned as follows:
| Parameter | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| Cervical dilation (cm) | Closed (0) | 1-2 | 3-4 | 5-6 |
| Cervical effacement (%) | 0-30 | 40-50 | 60-70 | 80+ |
| Fetal station | -3 | -2 | -1 or 0 | +1 or +2 |
| Cervical consistency | Firm | Medium | Soft | - |
| Cervical position | Posterior | Middle | Anterior | - |
Maximum total score: 13
Dilation and effacement each score 0-3; station 0-3; consistency 0-2; position 0-2.
Score Modifiers
Add 1 point for:
- Preeclampsia
- Each prior vaginal delivery
Subtract 1 point for:
- Post-dates pregnancy
- Nulliparity
- Premature or prolonged rupture of membranes
How to Interpret the Score
| Bishop Score | Clinical Interpretation |
|---|---|
| ≥9 | Favorable cervix - induction success approaches that of spontaneous labor; average labor ~4 hours in multiparas; essentially no failed inductions in Bishop's original series |
| 6-8 | Moderately favorable; induction likely to succeed |
| <6 | Unfavorable cervix - correlates with prolonged labor or failed induction; cervical ripening recommended before induction |
| ≤5 (nullipara) | ~50% risk of failed induction |
Clinical Usefulness in Pregnancy Monitoring
1. Decision to Induce Labor
The primary use of the Bishop score is to determine whether the cervix is ready for labor induction and whether cervical ripening agents are needed first. Before initiating any induction, a cervical assessment with Bishop scoring should be performed, along with a non-stress test (NST) to confirm fetal well-being.
2. Selecting the Method of Induction
- Favorable cervix (Bishop ≥6-8): Proceed directly with oxytocin IV infusion or amniotomy (artificial rupture of membranes). Amniotomy is highly effective when the vertex is engaged and the cervix is ≥2 cm dilated - only 3.4% of such patients require additional oxytocin.
- Unfavorable cervix (Bishop <6): Cervical ripening is needed first.
3. Guiding Cervical Ripening
When the score is low, ripening can be achieved by:
Pharmacological methods (preferred):
- Dinoprostone (PGE2, Prepidil/Cervidil) - FDA approved; 0.5 mg intracervical gel q6-12h, or 10 mg vaginal slow-release insert
- Misoprostol (PGE1, Cytotec) - off-label; more potent; more effective than PGE2 per meta-analysis; contraindicated with prior uterine scar/cesarean section due to uterine rupture risk
Mechanical methods:
- Foley catheter balloon (30-50 mL in lower uterine segment, exerts pressure on internal os)
- Laminaria (osmotic dilators from seaweed; draw water from cervix)
- Membrane sweeping (if cervix admits a finger)
4. Predicting Preterm Birth Risk
Beyond induction planning, Bishop score assessed by digital examination has also been studied as a predictor of preterm birth - alongside cervical ultrasound measurement. Iams and colleagues found that digital cervical examination (expressed as Bishop score) and transvaginal ultrasound of the cervix were both useful in predicting preterm birth in high-risk women.
5. Monitoring Progress Over Time
Repeated scoring at clinical visits during the last weeks of pregnancy can track cervical change (ripening), helping identify women approaching readiness for labor or those who may require induction.
Simplified Bishop Score
A simplified 3-parameter version using only dilation, effacement, and station (max score: 9) was validated in a large study of 5,610 nulliparous women undergoing induction (Laughton et al., Obstet Gynecol 2011). It demonstrated better positive and negative predictive values than the traditional 5-parameter score and is easier to calculate at the bedside.
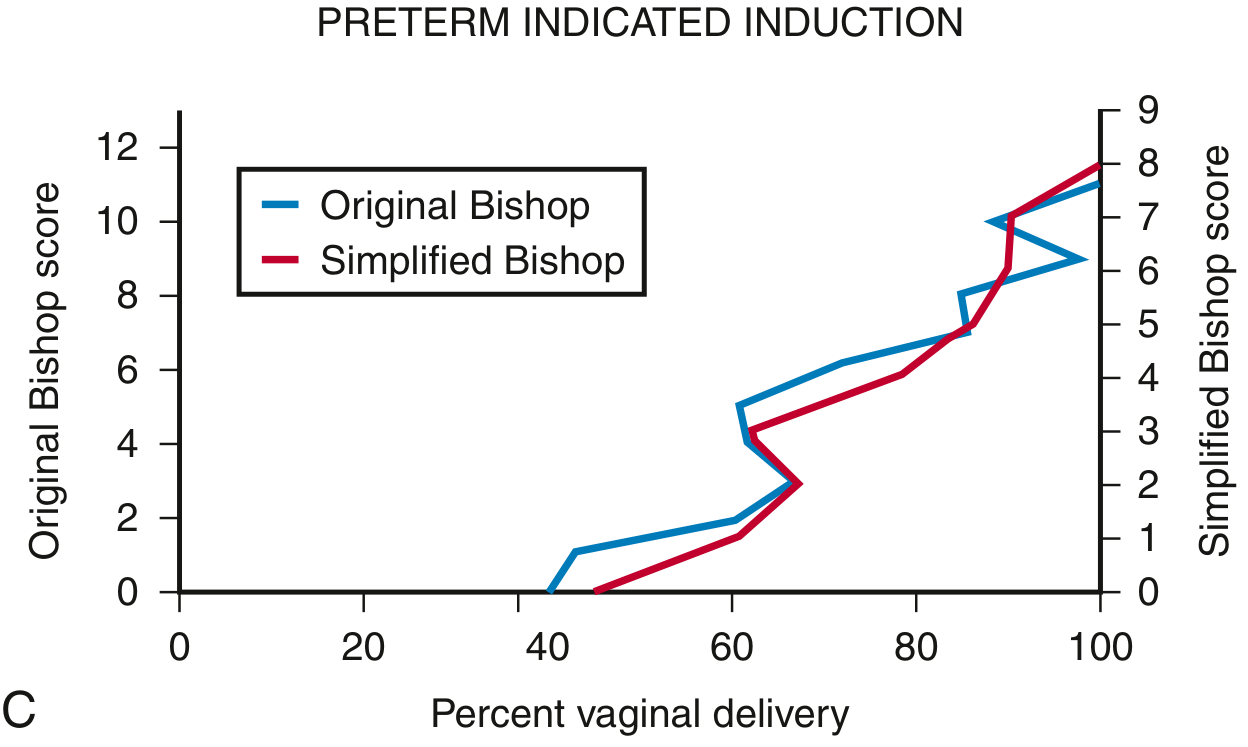
As shown above, both the original and simplified Bishop scoring systems show a strong positive correlation with the rate of vaginal delivery across all populations (term induction, preterm induction, spontaneous labor).
Limitations
- Subjectivity: Some parameters (consistency, position) are semi-subjective and vary between examiners
- Cervical dilation is the most important predictor - Lange et al. (808-patient study) found dilation was the single most important component, suggesting it should be weighted double
- Transvaginal ultrasound of cervical length does not improve on the Bishop score for predicting induction success
- Fetal fibronectin (fFN) in cervical/vaginal secretions is an additional predictor of successful induction, though its precise role in elective induction selection is still being defined
- The original Bishop criteria technically applied only to multiparous women, though subsequent studies confirmed its usefulness in nulliparas as well
Indications for Labor Induction (context for Bishop scoring)
The Bishop score is calculated whenever induction is being considered for any of these indications:
- Preeclampsia/eclampsia/pregnancy-induced hypertension
- Prolonged/post-term pregnancy (>42 weeks)
- Premature rupture of membranes
- Fetal growth restriction or non-reassuring fetal testing
- Maternal diabetes, renal disease, chronic hypertension
- Abruptio placentae
- Chorioamnionitis
- Fetal demise
- Logistic/social indications (distance from hospital, history of rapid labor) - elective induction only at ≥39 weeks with confirmed gestational age
Summary
The Bishop score remains the standard bedside tool to evaluate cervical "ripeness" before labor induction. A score ≥9 means go ahead with oxytocin or amniotomy; a score <6 means ripen the cervix first. Its key contribution to pregnancy monitoring is translating the subjective clinical impression of the cervix into an objective number that predicts outcomes, guides clinical decisions, and reduces the risk of failed induction and unnecessary cesarean section.
Sources: Creasy & Resnik's Maternal-Fetal Medicine 8e; Textbook of Family Medicine 9e; Pfenninger & Fowler's Procedures for Primary Care 3e; Bishop EH, Obstet Gynecol 1964
This is a shared conversation. Sign in to Orris to start your own chat.