Lupus nephritis ref. Robins harrison davidson
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed. Note: Davidson's Principles and Practice of Medicine is not in this textbook library, but I have comprehensive data from Robbins Basic Pathology, Robbins & Cotran Pathologic Basis of Disease, and Harrison's 22e. Let me compile the full, detailed answer.
Lupus Nephritis
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Harrison's Principles of Internal Medicine 22e (2025)
Note: Davidson's Principles and Practice of Medicine is not in the available textbook library. The coverage below is drawn from Robbins (both editions) and Harrison's 22e, which together provide the pathology, classification, clinical features, and management comprehensively.
Definition and Epidemiology
Lupus nephritis is a common and serious complication of systemic lupus erythematosus (SLE). Clinical manifestations of kidney disease are present in 30% of patients at the time of SLE diagnosis, and the majority will develop kidney abnormalities over the course of their disease. Up to 50% of all SLE patients develop clinically significant renal involvement, mainly in the form of autoimmune-mediated glomerulopathies and tubulointerstitial nephritis.
- Harrison's 22e, p. 2461; Robbins Cotran, p. 854
Pathogenesis
SLE is the prototype of a human systemic immune complex disease (type III hypersensitivity). The mechanism involves:
- Immune complex deposition - Circulating complexes composed primarily of DNA and anti-DNA antibodies deposit in the glomerular mesangium, subendothelial, and subepithelial spaces.
- Complement activation - Immune complex binding activates the complement cascade, causing complement-mediated damage, leukocyte infiltration, activation of procoagulant factors, and release of cytokines.
- In situ complex formation - Also plays a role alongside circulating complex deposition.
- Immunoglobulin profile - Deposits are usually reactive for IgG, often accompanied by IgA, IgM, C3, and C1q. The presence of all three immunoglobulin classes plus both complement components (C3 + C1q) is called the "full house" pattern, highly characteristic of lupus.
Anti-dsDNA antibodies that fix complement correlate best with the presence and activity of kidney disease. Hypocomplementemia is common in acute lupus nephritis (70-90%), and declining complement levels may herald a flare.
- Robbins Basic Pathology, p. 510; Robbins Cotran, p. 854-855; Harrison's 22e, p. 2461
ISN/RPS Classification (2004, revised 2018)
The WHO first outlined patterns of lupus glomerular injury in 1974; the classification was revised in 2004 by the International Society of Nephrology - Renal Pathology Society (ISN/RPS), which recognizes six classes. There is overlap between classes, and lesions may evolve over time. Class I is least common; Class IV is most common.
| Class | Name | Histology | Clinical Features |
|---|---|---|---|
| I | Minimal mesangial | Immune complex deposits in mesangium by IF/EM; normal LM | Asymptomatic; normal urinalysis and creatinine |
| II | Mesangial proliferative | Mesangial cell proliferation + mesangial matrix expansion; granular mesangial Ig/complement deposits; no capillary involvement | Proteinuria or microscopic hematuria; almost never nephrotic syndrome or renal failure |
| III | Focal nephritis | <50% glomeruli affected; segmental or global; endothelial and mesangial cell swelling/proliferation, leukocyte accumulation, capillary necrosis, hyaline thrombi, focal crescent formation | Hematuria + proteinuria; active urinary sediment; some have nephrotic syndrome, hypertension, decreased GFR; <5% progress to renal failure over 5 years with therapy |
| IV | Diffuse nephritis | >50% glomeruli affected; same lesions as III but diffuse; "wire loop" lesions (subendothelial deposits causing circumferential capillary wall thickening); cellular crescents; fibrinoid necrosis | Hematuria, proteinuria, hypertension, renal insufficiency; most symptomatic class; worst prognosis without treatment |
| V | Membranous nephritis | Diffuse thickening of capillary walls due to subepithelial immune deposits; may coexist with Class III or IV ("mixed membranous and proliferative") | Nephrotic syndrome; less hematuria than proliferative classes |
| VI | Sclerotic nephritis | Global sclerosis of nearly all glomerular capillaries; represents end-stage burnt-out lupus nephritis | Chronic renal failure; unresponsive to immunosuppression |
- Harrison's 22e, Table 326-3, p. 2461; Robbins Cotran, p. 855-856; Robbins Basic Pathology, p. 511
Characteristic Morphological Features
"Wire Loop" Lesions (Class IV hallmark)
Subendothelial immune complex deposits cause circumferential thickening of the capillary wall, creating the appearance of rigid "wire loops" on light microscopy (PAS or silver stains). This is pathognomonic of Class IV diffuse lupus nephritis.
Hyaline Thrombi
Intracapillary accumulations of immune complexes forming eosinophilic plugs.
Hematoxylin Bodies
Nuclear material extruded from damaged cells, forming hematoxylin-stained inclusions - the tissue equivalent of LE cells.
Crescents
Extracapillary proliferation of parietal epithelial cells + macrophages filling Bowman's space; seen especially in Classes III and IV when active.
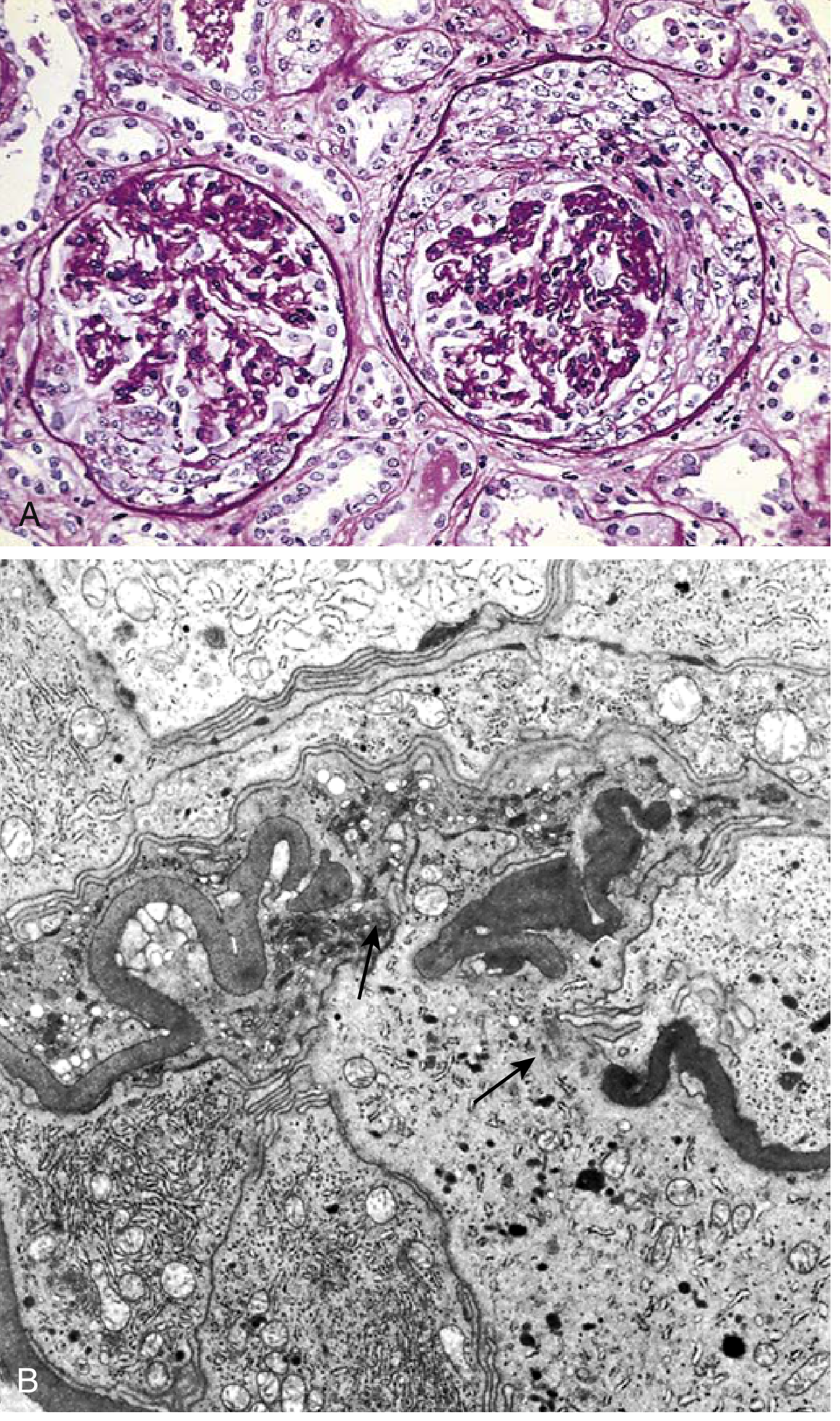
Crescentic GN - as may be seen in severe lupus nephritis (Class III/IV with active lesions). PAS (A) and electron microscopy (B). - Robbins Basic Pathology, Fig. 12.10
Tubulointerstitial Nephritis
Can accompany any class; mediated by immune complex deposits in tubular basement membranes.
- Robbins Cotran, p. 855-856; Robbins Basic Pathology, p. 511-512
Clinical Features
| Feature | Details |
|---|---|
| Proteinuria | Most common sign; ranges from mild to nephrotic-range (>3.5 g/day) |
| Haematuria | Microscopic or gross; red cell casts indicate active glomerulitis |
| Active urine sediment | RBC casts, granular casts - correlate with nephritic pattern |
| Hypertension | Common in proliferative classes (III, IV) |
| Nephrotic syndrome | Primarily Class V; can occur in severe Class IV |
| Nephritic syndrome | Classes III and IV |
| RPGN | Severe Class IV or III with extensive crescents |
| Acute/chronic renal failure | Class IV and Class VI |
| Anti-dsDNA | Titres correlate with disease activity |
| Hypocomplementemia | C3/C4 low in 70-90% of active lupus nephritis; falling levels herald flare |
- Harrison's 22e, p. 2461; Robbins Cotran, p. 854
Diagnosis
- Kidney biopsy is required in most patients with kidney involvement to establish histologic subtype, which directly guides therapy.
- Anti-dsDNA antibodies (especially complement-fixing) and low C3/C4 support the diagnosis and correlate with activity.
- Urinalysis with microscopy: active sediment (RBC casts) suggests proliferative disease.
- 24-hour urine protein or urine protein:creatinine ratio quantifies proteinuria.
Treatment (Harrison's 22e)
Treatment is closely tied to histologic class:
Classes I and II
- Minimal kidney manifestations, normal or near-normal kidney function.
- Excellent prognosis - little or no specific therapy for nephritis needed.
- Treat underlying SLE with hydroxychloroquine; ACE inhibitors/ARBs for proteinuria if present.
Class III (Focal) and Class IV (Diffuse) - Proliferative Lupus Nephritis
These are the most aggressive forms requiring active immunosuppression:
Induction therapy (to achieve remission):
- High-dose corticosteroids (IV methylprednisolone pulses followed by oral prednisolone)
- Combined with mycophenolate mofetil (MMF) OR cyclophosphamide (CYC)
- MMF (2-3 g/day) is preferred in most centres (equivalent efficacy to CYC with better tolerability)
- IV cyclophosphamide (NIH protocol or low-dose Euro-Lupus protocol) remains standard in severe disease
- Voclosporin or belimumab (anti-BLyS) can be added to MMF as triple therapy (newer approach)
Maintenance therapy (to prevent relapse):
- MMF (1-2 g/day) or azathioprine (AZA) - MMF is generally preferred
- Low-dose corticosteroids
- Hydroxychloroquine - all SLE patients without contraindication
Class V (Membranous)
- If nephrotic syndrome: steroids + MMF or CYC
- Pure Class V without proliferative component has a better prognosis
- ACE inhibitors/ARBs for antiproteinuric effect
Class VI (Sclerotic)
- Immunosuppression is not beneficial (burnt-out disease)
- Supportive care; preparation for renal replacement therapy
All Classes
-
Hydroxychloroquine - recommended for all SLE patients; renoprotective effect
-
ACE inhibitors/ARBs - reduce proteinuria and slow progression
-
Blood pressure control (<130/80 mmHg target)
-
Monitor for treatment toxicity (bone marrow suppression with CYC, infections, osteoporosis with steroids)
-
Harrison's 22e, p. 2461-2462
Prognosis
- Classes I and II: excellent; rarely progress to renal failure.
- Class III: <5% progress to kidney failure at 5 years with treatment; patients with heavy proliferation involving a large percentage of glomeruli have worse outcomes.
- Class IV: most severe; untreated, most patients progress to ESKD. With modern immunosuppression, 5-year kidney survival is ~80-90%.
- Class V: generally good, though nephrotic syndrome may persist; small risk of progression.
- Class VI: end-stage; dialysis/transplantation.
Key Points Summary (Robbins Perspective)
"Much of the pathology is caused by immune complexes composed of nuclear antigens and specific antibodies; in fact, SLE is the prototype of a human systemic immune complex disease (type III hypersensitivity). Glomeruli are the major site of deposition of immune complexes and bear the brunt of the lesions."
- Robbins Basic Pathology, p. 510
"Class I is the least common and class IV is the most common pattern."
Wire loops, hyaline thrombi, hematoxylin bodies, and the "full house" immunofluorescence pattern (IgG + IgA + IgM + C3 + C1q) are histological hallmarks distinguishing lupus nephritis from other glomerulopathies.
Note on Davidson's: Davidson's Principles and Practice of Medicine is not available in this textbook library. The above covers the topic as presented in Robbins (both Basic Pathology and Cotran editions) and Harrison's 22e (2025), which are the authoritative references for pathology and clinical medicine respectively.
This is a shared conversation. Sign in to Orris to start your own chat.