Best indicator for assesment of tissue perfusion in a septic patient is?
lactate tissue perfusion sepsis indicator
Serum Lactate - Best Indicator of Tissue Perfusion in Sepsis
Why Lactate?
- "As the product of anaerobic metabolism, lactate is an indicator of insufficient oxygen delivery to cells." - Barash's Clinical Anesthesia, 9e
- "Though hypoperfusion is the suspected cause of lactic acidosis in sepsis, various degrees of intermediary metabolic alterations may contribute to the increased lactate production." - Barash's Clinical Anesthesia, 9e
- Lactic acidosis in sepsis is classified as Type A (impaired tissue perfusion/hypoxia), per Harper's Illustrated Biochemistry
Clinical Thresholds
| Lactate Level | Interpretation |
|---|---|
| < 2 mmol/L | Normal |
| 2-4 mmol/L | Cryptic shock / occult hypoperfusion - warrants aggressive resuscitation |
| > 4 mmol/L | Overt shock - high mortality, ICU admission mandatory |
Lactate Clearance as a Resuscitation Goal
- >10% reduction in lactate over 2 hours = adequate resuscitation response
- The Surviving Sepsis Campaign guidelines recommend lactate clearance as a marker of improving tissue hypoperfusion
- A lactate that fails to clear despite resuscitation carries a worse prognosis
Important Limitations
- Liver dysfunction - impairs lactate clearance; levels may remain elevated even when production normalizes
- Catecholamines (especially epinephrine) - can increase hepatic lactate production via increased glycolysis, independent of true tissue hypoperfusion
- Sepsis-specific metabolic alterations - lactate can rise due to altered intermediary metabolism even when tissue oxygen tension is normal (mitochondrial dysfunction, Warburg effect)
How Lactate Compares to Other Markers
| Marker | Role | Limitation vs Lactate |
|---|---|---|
| Serum lactate | Best overall tissue perfusion indicator | Affected by clearance issues |
| ScvO2 (central venous O2 sat) | Surrogate for O2 extraction ratio; >70% is a target | Mixed evidence for outcome benefit; newer trials failed to replicate early benefit |
| Blood pressure / MAP | Crude hemodynamic marker | Misses occult/cryptic shock |
| Urine output | Marker of renal perfusion | Lagging indicator |
| Procalcitonin | Infection/inflammation marker | Not a perfusion marker |
| Base deficit | Metabolic acidosis marker | Less specific than lactate |
What about the urine output? More than 0.5ml/kg/hr
Urine Output vs. Lactate in Sepsis
Urine Output >0.5 ml/kg/hr
-
Organ-specific, not global - It only reflects renal perfusion. Other organs (gut, liver, brain) may still be hypoperfused even when urine output is adequate.
-
It can be falsely reassuring (lag effect) - As stated directly in Mulholland's Surgery: "Inappropriate urine output may initially be maintained by peripheral vasoconstriction and maintenance of cardiac output due to tachycardia" - meaning you can be in compensated shock with a normal urine output.
-
Renal perfusion is preferentially maintained - The body preserves blood flow to the brain and heart first, at the expense of skin, muscle, gut, and eventually kidneys. By the time urine output drops, hypoperfusion of other organs is already advanced.
-
Confounders - ADH release, contrast nephropathy, pre-existing renal disease, diuretics, and glycosuria can all distort urine output readings independent of perfusion status.
-
It is a lagging indicator - Urine output reflects what has already happened over the past hour, not real-time cellular metabolism.
The Hierarchy of Perfusion Markers
| Marker | What it reflects | Speed | Specificity for global hypoperfusion |
|---|---|---|---|
| Serum lactate | Whole-body anaerobic metabolism | Fast (blood test) | Best - global |
| ScvO2 | Oxygen extraction across all tissue beds | Continuous (if CVC) | Good - global |
| Urine output >0.5 ml/kg/hr | Renal perfusion only | Hourly | Limited - organ-specific |
| MAP >65 mmHg | Driving pressure - not flow | Continuous | Poor - doesn't detect occult shock |
| Base deficit | Metabolic acidosis burden | Fast | Moderate |
The Key Conceptual Point
Urine output is a resuscitation target (something you aim to achieve), while lactate is a perfusion indicator (something that directly tells you whether cells are getting enough oxygen). These are different roles.
Hematanesis patient resuscitation done with blood and fluids what is next step? Iv terlipression or binding?
variceal bleeding terlipressin band ligation management
esophageal varices acute bleeding treatment guidelines
PMID: 37978969
Hematemesis (Variceal Bleeding) - After Resuscitation: What's Next?
The Correct Sequence
Resuscitation (blood + fluids)
↓
STEP 1: IV Vasoactive Drug IMMEDIATELY
(Start as soon as variceal source suspected - BEFORE endoscopy)
↓
STEP 2: Urgent Endoscopy (within 12 hours)
+ Endoscopic Band Ligation (EBL) ← preferred over sclerotherapy
↓
STEP 3: Continue vasoactive drug for 2-5 days post-endoscopy
(prevents early rebleeding)
↓
STEP 4: Early TIPS if high-risk (Child-Pugh B/C, HVPG >20 mmHg)
↓
STEP 5: Secondary prophylaxis with non-selective beta-blockers + repeat EBL
Why Vasoactive Drug FIRST (Before Endoscopy)?
- Reduces portal pressure via splanchnic vasoconstriction
- Controls active bleeding before the scope is even inserted
- Makes the endoscopic field cleaner and safer
- Buys time if endoscopy is delayed
Which Vasoactive Drug?
| Drug | Preferred in | Mechanism |
|---|---|---|
| Terlipressin | Europe, Asia, most of world | V1 receptor agonist - splanchnic vasoconstriction; also FDA-approved in USA since 2022 |
| Octreotide | USA (drug of choice per AGA 2024) | Somatostatin analog - inhibits splanchnic vasodilation |
| Somatostatin | Europe (where available) | Same as octreotide |
| Vasopressin | Largely abandoned | Too many cardiac side effects |
AGA 2024 Best Practice Advice 3: "Octreotide is the vasoactive drug of choice in the management of variceal hemorrhage based on its safety profile."
Terlipressin is equally effective but has more cardiac side effects (contraindicated in ischemic heart disease). In many exam contexts (Indian/UK boards), terlipressin is listed as the drug of choice.
Why Band Ligation Over Sclerotherapy?
- Equal or better hemostasis rates (85-95%)
- Far fewer complications than sclerotherapy (no esophageal ulcers, strictures, mediastinitis)
- Varices eradicated in fewer sessions
- Sclerotherapy is a backup when EBL is technically not possible (e.g., active spurting blood obscuring view, gastric varices)
Additional Measures (Do Not Miss)
- IV Ceftriaxone 1g/day x 7 days - mandatory antibiotic prophylaxis; reduces infections, early rebleeding, and mortality
- Avoid over-transfusion - transfuse to Hb ~7-8 g/dL only (over-transfusion raises portal pressure and worsens bleeding)
- Avoid beta-blockers acutely - only for secondary prophylaxis after acute episode controlled
- TIPS (Transjugular Intrahepatic Portosystemic Shunt) - if endoscopy fails to control bleeding, or as pre-emptive TIPS within 72h in high-risk patients (Child-Pugh B with active bleeding or Child-Pugh C)
To Directly Answer Your Question
| Your Question | Answer |
|---|---|
| IV Terlipressin or Band Ligation first? | Terlipressin (or octreotide) FIRST, then band ligation at endoscopy |
| Are they alternatives? | No - they are used together |
| Which is "the next step" after resuscitation? | IV vasoactive drug (terlipressin/octreotide) is the immediate next step |
Brain deaths criteria in icu
brain death determination criteria guidelines
PMID: 37821233
Brain Death (Death by Neurological Criteria) - ICU Criteria
Definition: Irreversible cessation of all functions of the entire brain, including the brainstem, in a patient on mechanical ventilation with a known catastrophic brain injury.
STEP 1: Prerequisites (ALL Must Be Satisfied First)
| Prerequisite | Requirement |
|---|---|
| Known cause of coma | Confirmed by history + neuroimaging (CT/MRI) |
| Irreversibility established | Catastrophic structural brain injury; no treatable cause |
| Normothermia | Core temperature ≥36°C (hypothermia mimics brain death) |
| Hemodynamic stability | Systolic BP ≥100 mmHg (needed before apnea test) |
| No sedatives/analgesics | Adequate time for drug clearance; toxicology screen if uncertain |
| No neuromuscular blockers | Use peripheral nerve stimulator to confirm if any doubt |
| No severe metabolic derangement | Exclude severe electrolyte, acid-base, or endocrine abnormality |
| No hypoglycemia | Blood glucose must be normal |
| Neuroimaging explains coma | CT/MRI must show a lesion consistent with brain death |
STEP 2: Clinical Neurological Examination
A. Coma
- No motor response to noxious stimuli (central pain stimulation - supraorbital ridge, nail bed pressure)
- GCS = 3 (E1V1M1)
- Note: Spinal reflexes (triple flexion, deep tendon reflexes) can still be present and do NOT exclude brain death - only brainstem-mediated responses matter
B. Absent Brainstem Reflexes (ALL must be absent)
| Reflex | How Tested | Expected in Brain Death |
|---|---|---|
| Pupillary light reflex | Bright light in each eye | Pupils fixed, mid-dilated (4-6 mm), no constriction |
| Corneal reflex | Cotton wisp on cornea | No blink response bilaterally |
| Oculocephalic reflex (Doll's eyes) | Head rotated rapidly side to side | Eyes remain fixed (no movement) - only test if C-spine cleared |
| Oculovestibular reflex (Caloric testing) | 50 mL ice water in each ear, head at 30°; wait 1 min, 5 min between sides | No eye deviation toward the cold stimulus |
| Gag reflex | Finger or tongue blade to posterior pharynx | Absent |
| Cough reflex | Deep suction catheter to level of carina | No cough response |
| Response to pain | Supraorbital/nail bed pressure | No grimacing, no purposeful movement |
Important: Constricted pupils suggest opioid effect - do NOT proceed until excluded.
STEP 3: Apnea Test
- Pre-oxygenate with 100% O2 for 10 minutes → target PaO2 ≥200 mmHg
- Confirm normocapnia: baseline PaCO2 35-45 mmHg
- Confirm SBP ≥100 mmHg
- Disconnect ventilator - provide passive O2 via catheter at carina (6 L/min) or T-piece
- Observe for 8-10 minutes for any respiratory effort (chest movement, abdominal excursion, gasping)
- Draw ABG at end
- PaCO2 ≥60 mmHg OR rise of ≥20 mmHg from baseline with no spontaneous breathing effort
STEP 4: Ancillary (Confirmatory) Tests
- Clinical exam cannot be fully completed (e.g., facial trauma, bilateral tympanic membrane rupture preventing caloric testing)
- Apnea test is aborted or inconclusive
- Confounders cannot be fully excluded
| Test | Finding in Brain Death |
|---|---|
| EEG | Electrocerebral silence (flat, <2 mV for 30 min, min. 8 electrodes) |
| CT Angiography (head + neck) | No intracranial blood flow (gold standard for flow) |
| Nuclear CBF scan (Tc-99m) | No cerebral blood flow - "hollow skull sign" |
| Transcranial Doppler | Absent or reverberating flow pattern |
| Auditory/Somatosensory Evoked Potentials | Absent cortical responses |
Who Can Declare Brain Death?
- At least one physician (attending level, trained in neurology/neurosurgery/critical care)
- Many institutions require two independent physicians
- One examination is sufficient in most US states if the clinical exam + apnea test are both complete
- Pediatric patients (<1 year) may require two exams 24 hours apart
Quick Memory Aid
BRAIN DEATH =
Known irreversible cause
+ No confounders (temp, drugs, metabolic)
+ Deep coma (no motor response)
+ All 7 brainstem reflexes absent
+ Positive apnea test (PaCO2 ≥60, no breathing)
Key Distinguishing Points (Exam Favorites)
| Feature | Brain Death | Vegetative State | Locked-in Syndrome |
|---|---|---|---|
| Brainstem reflexes | Absent | Present | Present |
| Apnea test | Positive | Breathes spontaneously | Breathes spontaneously |
| Eye movements | None | Roving | Vertical only |
| Awareness | None | None | Present |
| Legal death | Yes | No | No |
Patella surgery only one nerve block sufficient?
Nerve Block for Patella Surgery - Is One Enough?
Direct Answer from the Textbook
Patellar ORIF or tendon repair → Femoral nerve block (assuming a knee immobilizer will be used)
Why Femoral Nerve Block Alone Works for the Patella
| Structure | Primary Nerve |
|---|---|
| Patella (bone + anterior capsule) | Femoral nerve (dominant) |
| Medial knee skin | Saphenous nerve (terminal branch of femoral) |
| Posterior knee | Sciatic/tibial/common peroneal |
| Medial capsule | Obturator nerve |
Fascia Iliaca Block = Equivalent Alternative
"Level 1 evidence in the setting of surgery for patella fractures suggests that fascia iliaca nerve blockade is equally efficacious while being safer and easier to perform relative to femoral nerve block."
| Block | Advantage |
|---|---|
| Femoral nerve block | Direct, well-established |
| Fascia iliaca block | Level 1 evidence; safer, easier; covers femoral + lateral femoral cutaneous + obturator nerves |
Contrast with Total Knee Arthroplasty
- Adductor canal block (or femoral) + sciatic block for surgical anesthesia
- Lumbar plexus + sciatic for complete coverage
Important Caveat
- Posterior knee (sciatic)
- Tourniquet pain at thigh level (requires additional proximal block or IV analgesia)
Most common nerve danaged in upper limb in type 2 crps
Most Common Nerve Damaged in Upper Limb CRPS Type 2
Direct Answer
"Causalgia is the name that Weir Mitchell applied to peripheral neuralgia consequent on trauma, most often following partial interruption of the median or ulnar nerve and, less often, the sciatic or peroneal nerve."
Why the Median Nerve?
-
Highest density of sympathetic (autonomic) fibers among upper limb nerves - the median nerve carries proportionally more C-fiber afferents and sympathetic efferents, making its partial injury more likely to trigger the pathological sympathetic-sensory cross-excitation that underlies CRPS Type 2
-
Anatomical vulnerability - travels through the forearm and wrist (carpal tunnel), areas frequently injured by penetrating wounds, lacerations, and crush injuries
-
Historical association - Weir Mitchell first described causalgia in Civil War soldiers with gunshot wounds, and the median nerve was the most commonly affected in those high-velocity partial injuries
CRPS Type 2 vs Type 1 - Key Distinction
| Feature | CRPS Type 1 (RSD) | CRPS Type 2 (Causalgia) |
|---|---|---|
| Nerve injury identifiable? | No - no specific nerve injury | Yes - direct, documented nerve injury |
| Former name | Reflex Sympathetic Dystrophy | Causalgia |
| Most common nerve (UL) | N/A | Median > Ulnar |
| Most common nerve (LL) | N/A | Sciatic > Peroneal |
| Mechanism | Unclear, possibly central sensitization | Partial nerve injury → sympathetic-afferent coupling |
Why "Partial" Injury Matters
- Some intact C-fibers remain sensitized
- Abnormal ephaptic transmission occurs between damaged sympathetic efferents and intact pain afferents at the injury site
- Circulating catecholamines activate α-adrenergic receptors on sensitized nociceptors
- This creates a self-sustaining pain loop (sympathetically maintained pain)
Memory Tip
"CRPS 2 = Causalgia = Median nerve most common in upper limb" (Weir Mitchell, Civil War wounds, burning pain in the hand)
Stepwise management plan for crps
complex regional pain syndrome treatment guidelines
PMID: 37185896
Stepwise Management of CRPS
Core principle: Early, aggressive, multidisciplinary treatment gives the best outcomes. The longer CRPS is untreated, the more refractory it becomes. Physical rehabilitation is the backbone - everything else supports it.
STEP 1: Early Recognition + Diagnosis
- Use the Budapest Criteria (current gold standard for diagnosis):
- Continuing pain disproportionate to the inciting event
- At least 1 symptom in 3 of 4 categories: sensory (allodynia/hyperalgesia), vasomotor (temperature/color asymmetry), sudomotor/edema, motor/trophic
- At least 1 sign in 2 of 4 categories at time of evaluation
- No other diagnosis explains the findings
- Distinguish CRPS 1 (no nerve injury) from CRPS 2 (documented nerve injury = causalgia)
- Start treatment immediately - do not wait for spontaneous resolution
STEP 2: Physical & Occupational Therapy (FIRST LINE - Foundation)
| Modality | Details |
|---|---|
| Graded motor imagery (GMI) | Mirror therapy, mental imagery, left/right discrimination - targets cortical reorganization |
| Mirror therapy | Especially effective in early CRPS of upper limb |
| Desensitization | Progressive tactile stimulation to reduce allodynia |
| Active range of motion | Gentle, pain-guided mobilization; avoid forced movement |
| Edema management | Compression, elevation, contrast baths |
| Occupational therapy | Functional task retraining, splinting, adaptive equipment |
"A certain degree of improvement can be expected if treatment is started early and the limb is mobilized." - Adams & Victor's Neurology, 12e
STEP 3: Pharmacotherapy (Concurrent with Step 2)
A. Neuropathic Pain Agents (First Line)
| Drug | Dose | Notes |
|---|---|---|
| Gabapentin | 300-3600 mg/day | First-line neuropathic agent |
| Pregabalin | 150-600 mg/day | Alternative to gabapentin |
| TCAs (amitriptyline, nortriptyline) | 10-75 mg at night | Also treats depression/sleep |
| SNRIs (duloxetine) | 30-120 mg/day | Good for sympathetically maintained pain |
B. Anti-inflammatory / Bone Remodeling
| Drug | Evidence |
|---|---|
| Bisphosphonates (IV pamidronate, alendronate) | Strong evidence - reduces pain and bone resorption in CRPS |
| Calcitonin (intranasal) | Reduces bone pain; less used now |
| Corticosteroids (prednisolone 30-80 mg/day, short course) | Useful in early, hot/inflammatory CRPS |
| NSAIDs | Mild benefit only |
C. Topical Agents
- Topical lidocaine (5% patch) - strong evidence for localized allodynia
- Topical DMSO (dimethyl sulfoxide) 50% cream - evidence in early CRPS; free radical scavenger
- Capsaicin cream - desensitization of C-fibers
D. Other Systemic Agents
| Drug | Mechanism | Evidence |
|---|---|---|
| IV Ketamine (low-dose infusion) | NMDA antagonist - resets central sensitization | Strong evidence; used in refractory cases |
| IV Lidocaine | Membrane stabilization | Good evidence per 2023 systematic review [PMID: 37185896] |
| Opioids | Last resort; limited evidence; risk of dependence | Use cautiously |
| Clonidine (oral/patch/epidural) | α2-agonist - reduces sympathetic outflow | Useful adjunct |
E. Psychological Support (Throughout All Steps)
- CBT (cognitive behavioral therapy) - mandatory for chronic CRPS
- Address catastrophizing, fear-avoidance, depression
- Pain psychology referral early
STEP 4: Interventional Procedures
A. Sympathetic Nerve Blocks
| Block | Upper Limb | Lower Limb |
|---|---|---|
| Stellate ganglion block | Yes - T1 sympathetics | No |
| Lumbar sympathetic block | No | Yes |
| Mechanism: Local anesthetic (procaine/bupivacaine) → interrupts sympathetic-afferent loop |
"It can respond favorably, if only temporarily, to procaine block of the appropriate sympathetic ganglia." - Adams & Victor's Neurology, 12e
B. Intravenous Regional Sympatholysis (Bier Block Variant)
- IV guanethidine into isolated limb (tourniquet applied) - depletes norepinephrine from sympathetic terminals
- "May alleviate pain for days or longer" - Adams & Victor's
C. Brachial Plexus Block (Upper Limb)
- Strong evidence per 2023 systematic review
- Continuous catheter infusion provides prolonged relief
- Facilitates physiotherapy (pain-free window)
D. Epidural Infusion
- Epidural analgesics (opioids) or ketamine
- Continuous epidural useful for lower limb CRPS
STEP 5: Neuromodulation (Refractory Cases)
A. Spinal Cord Stimulation (SCS)
- Best evidence for refractory CRPS - considered the gold standard interventional treatment for chronic CRPS
- Dorsal column stimulation at C4-T1 (upper limb) or T8-L1 (lower limb)
- Produces paresthesia covering painful area
- "Spinal cord stimulators" listed as treatment in Adams & Victor's
B. Dorsal Root Ganglion (DRG) Stimulation
- Newer; more targeted than SCS; particularly effective for focal CRPS
C. Motor Cortex / Deep Brain Stimulation
- Reserved for extreme refractory cases; limited centers
STEP 6: Surgical Sympathectomy (Last Resort)
- Chemical or surgical sympathectomy - regional or thoracoscopic
- "For a longer time, to regional sympathectomy" - Adams & Victor's
- Used when repeated sympathetic blocks provide temporary but consistent relief
- Risk: post-sympathectomy neuralgia; not curative
Summary Algorithm
DIAGNOSIS (Budapest Criteria)
↓
STEP 1: Physiotherapy + Graded Motor Imagery (START EARLY)
↓
STEP 2: Pharmacotherapy
- Gabapentin/TCAs/SNRIs
- Bisphosphonates
- Topical lidocaine/DMSO
- Steroids (if early/hot phase)
+ Psychological support (CBT)
↓
STEP 3: Sympathetic nerve blocks
(Stellate - upper limb | Lumbar - lower limb)
+ Brachial plexus block / IV guanethidine
+ IV Ketamine / IV Lidocaine infusion
↓
STEP 4: Spinal Cord Stimulation (SCS)
↓
STEP 5: Surgical sympathectomy (last resort)
Key Points for Exams
| Fact | Answer |
|---|---|
| Foundation of CRPS treatment | Physiotherapy (especially graded motor imagery) |
| Strongest evidence drug class | Bisphosphonates + IV Ketamine + IV Lidocaine |
| Sympathetic block for upper limb | Stellate ganglion block |
| Best long-term interventional option | Spinal cord stimulation |
| Vitamin C for prevention? | No - 2023 systematic review shows no significant benefit [PMID: 37185896] |
| Key principle | Multidisciplinary + Early |
Question 41 Answer: B - Visceral Neuropathic Pain
- Right hypochondrium location (visceral = liver/biliary territory)
- Poorly localized (hallmark of visceral pain - viscera have sparse sensory innervation)
- Cramping quality (typical visceral descriptor: deep, cramping, aching, colicky)
- Opioid resistant (key feature of neuropathic component - when cancer infiltrates the celiac plexus, normal visceral pain becomes neuropathic and loses opioid responsiveness)
- Somatic neuropathic pain would be well-localized with dermatomal distribution
- CRPS requires autonomic/trophic features
- Psychogenic pain is a diagnosis of exclusion
- Nociceptive somatic pain responds to opioids and is well-localized
Question 42 Answer: E - Limbic System (Amygdala/Hippocampus)
The Two-Pathway Model of Pain Processing
| Pathway | Structure | Function |
|---|---|---|
| Spinothalamic tract (neospinothalamic) | Spinal cord → VPL thalamus → Somatosensory cortex (S1/S2) | Sensory-discriminative aspect: WHERE does it hurt? HOW intense? |
| Spinoparabrachial tract (paleospinothalamic) | Spinal cord → Parabrachial nucleus → Limbic system (amygdala, anterior cingulate, insular cortex) | Affective-motivational aspect: HOW unpleasant? Emotional suffering, memory of pain |
"Sensory discriminative features of the pain experience are transmitted from the spinal cord to the ventroposterolateral thalamus via the spinothalamic tract. A second pathway (the spinoparabrachial tract) carries information from the spinal cord to the parabrachial nucleus of the dorsolateral pons. These neurons in turn target limbic forebrain regions, including the insular and anterior cingulate cortex, which process emotional features of the pain experience." - Kandel's Principles of Neural Science, 6e
Why Each Option is Wrong
| Option | Role in Pain | Why NOT the answer |
|---|---|---|
| A. Medial Thalamus | Arousal, attention, affective tone of pain | Relay station only - not the primary memory/emotion processor |
| B. Lateral Thalamus (VPL) | Sensory-discriminative - location, intensity, quality | Processes "where/how much," NOT emotion or memory |
| C. Reticular Formation | Arousal, modulation of pain via descending pathways | Does not process memory or emotional response |
| D. VPL Nucleus | Same as lateral thalamus - somatosensory relay | Precision of pain location, not emotional memory |
| E. Limbic System (Amygdala/Hippocampus) ✓ | Emotional response (amygdala = fear/aversion) + Memory (hippocampus = contextual memory of painful events) | Correct answer |
The Amygdala's Specific Role
- Fear and aversion responses to pain
- Emotional learning from painful experiences
- Why chronic pain causes anxiety and psychological distress
- The "suffering" component of pain (distinct from the sensation itself)
- Contextual memory encoding of painful events
- Why people recall past painful experiences with distress
- Central sensitization through memory-based anticipatory pain
Medial thalmus?
Medial Thalamus vs. Limbic System - Why Limbic System Wins
What the Medial Thalamus DOES do in pain:
"Many neurons in the medial thalamus respond optimally to noxious stimuli and project to many regions of the limbic system, including the anterior cingulate cortex."
- Receives input via the paleospinothalamic tract (the "old" pain pathway)
- Responds to noxious stimuli
- Has large, diffuse receptive fields (poor localization)
- Projects TO the limbic system - it is an upstream relay, not the final processor
The Critical Distinction - Relay vs. Processor
Spinal cord
↓
Paleospinothalamic tract
↓
MEDIAL THALAMUS ──────────────→ LIMBIC SYSTEM
(relay/transmitter) (Amygdala + Hippocampus)
↑ THIS is where emotional
processing and MEMORY
of pain actually happen
| Structure | Role | Analogy |
|---|---|---|
| Medial Thalamus | Relay station - passes pain signals toward limbic regions; contributes to affective tone and arousal | A postal sorting office |
| Limbic System (Amygdala/Hippocampus) | Final processor of emotional response + memory encoding of pain | The person who reads and reacts to the letter |
Why the Question Specifically Asks "Memory AND Emotional Response"
- Memory of pain → Hippocampus (contextual memory encoding - why you remember the last time you burned yourself and dread it happening again)
- Emotional response to pain → Amygdala (fear, aversion, anxiety associated with pain)
Summary Table
| Structure | Sensory Location | Intensity | Affective Tone | Emotional Response | Memory of Pain |
|---|---|---|---|---|---|
| VPL (Lateral Thalamus) | ✓✓ | ✓✓ | ✗ | ✗ | ✗ |
| Medial Thalamus | ✗ | ✗ | ✓ (relay) | ✗ (projects to limbic) | ✗ |
| Limbic System (Amygdala/Hippocampus) | ✗ | ✗ | ✓✓ | ✓✓ | ✓✓ |
| Anterior Cingulate Cortex | ✗ | ✗ | ✓✓ | ✓✓ | ✗ |
Please explain hand nerve supply with images nerves involved snd clinical scebarios
Hand Nerve Supply - Complete Guide with Images
Overview: Three Nerves Supply the Hand
Sensory Map of the Hand
Dorsum (Back) of Hand
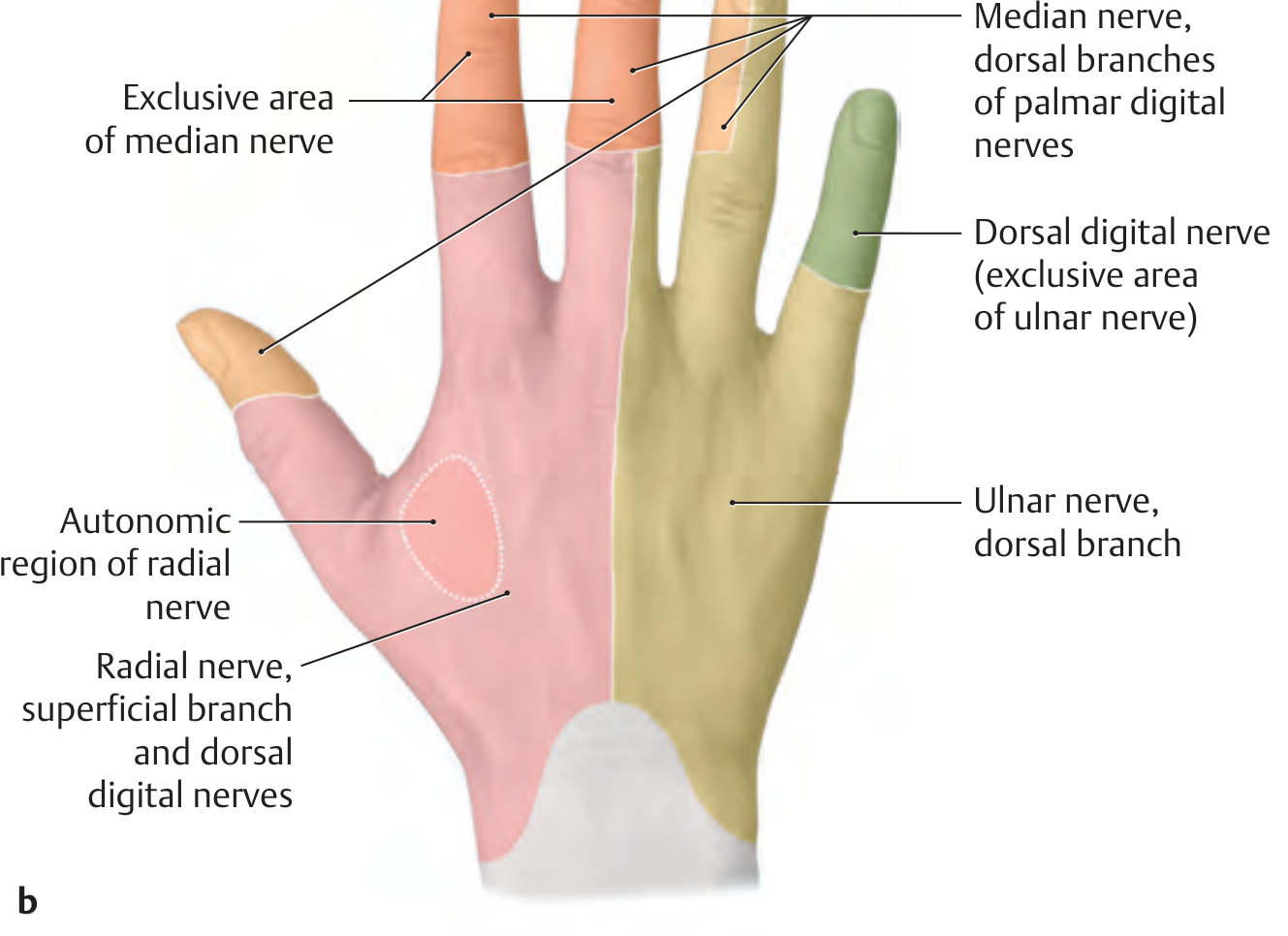
Key Sensory Rules (Palm/Dorsum)
| Nerve | Palm | Dorsum |
|---|---|---|
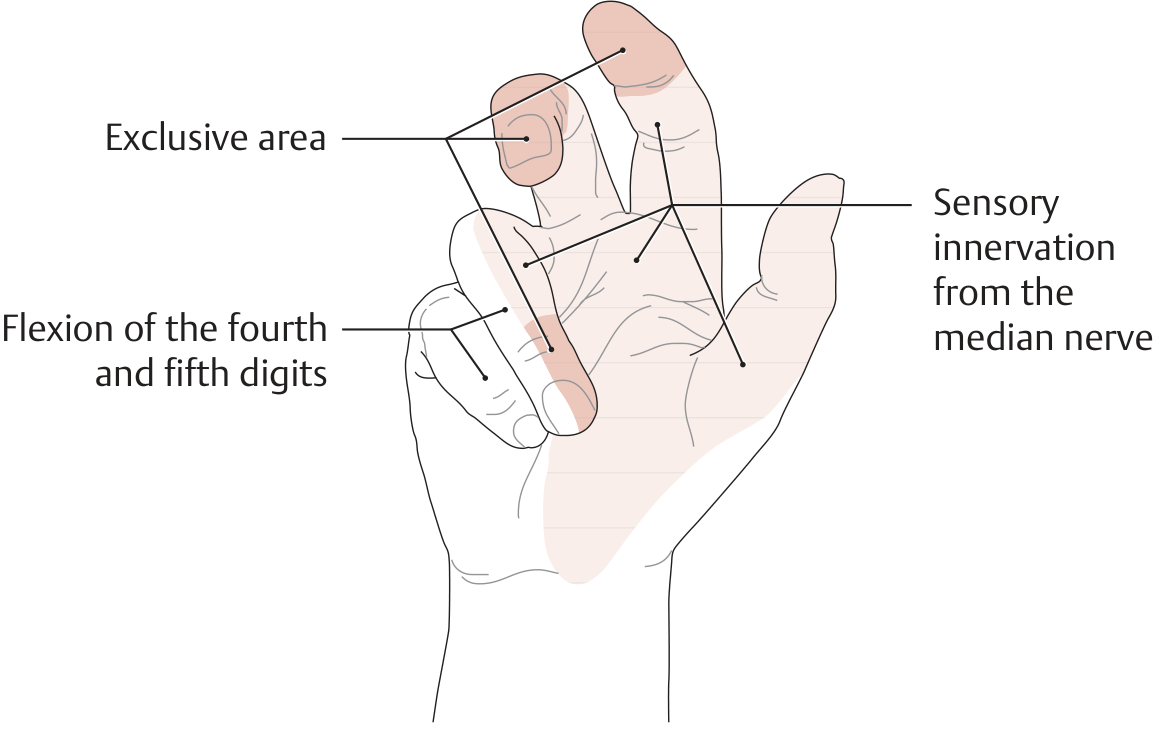
| Median | Lateral 3½ fingers (thumb, index, middle, radial half of ring) + thenar skin | Distal dorsum of index, middle, radial ring finger (fingertip skin) |
| Ulnar | Medial 1½ fingers (ulnar half of ring + little finger) | Medial dorsum of hand + little finger (exclusive territory) |
| Radial | Virtually NONE (small thenar skin strip) | Dorsum of hand, thumb, index, middle finger (proximal - to PIP level) |
Important: The dorsal fingertips of index, middle, and ring fingers are supplied by the median nerve via dorsal branches of palmar digital nerves - NOT by the radial nerve. This is a classic exam trap.
NERVE 1: MEDIAN NERVE (C6-T1)
Motor Supply in the Hand
| Muscle | Function |
|---|---|
| Lumbricals 1 & 2 (radial two) | Flex MCP, extend IP joints of index & middle finger |
| Opponens pollicis | Opposition of thumb (most important!) |
| Abductor pollicis brevis | Abducts thumb |
| Flexor pollicis brevis (superficial head) | Flexes thumb MCP |
Sensory Supply
- Palmar surface: Lateral 3½ fingers
- Palmar cutaneous branch (given off BEFORE carpal tunnel) → thenar skin
- Dorsal fingertips of index, middle, radial ring finger
CLINICAL SCENARIO 1: Carpal Tunnel Syndrome (CTS)
- Sensory loss: Lateral 3½ fingers (palmar surface)
- Thenar wasting - visible hollowing at base of thumb
- Weakness of opposition - cannot touch thumb to little finger
- Tinel's sign: Tapping over carpal tunnel → tingling in median nerve distribution
- Phalen's test: Sustained wrist flexion → symptoms in <60 sec
- Palmar skin SPARED (palmar cutaneous branch exits proximal to carpal tunnel)
CLINICAL SCENARIO 2: High Median Nerve Injury (Elbow/Forearm)
- "Hand of benediction" / "Papal hand" - when asked to make a fist:
- Index and middle fingers cannot flex (FDP to index/middle + FDS affected)
- Ring and little fingers flex normally (FDP ulnar half = ulnar nerve)
- Loss of pronation (pronator teres, pronator quadratus)
- Loss of wrist flexion (partially - FCU ulnar nerve spared)
- Sensory loss: Lateral 3½ fingers
Note: "Hand of benediction" = injury ABOVE wrist. "Ape hand" (thenar wasting only) = injury AT wrist (CTS chronic).
NERVE 2: ULNAR NERVE (C8-T1)
Motor Supply in the Hand
| Group | Muscles |
|---|---|
| Hypothenar muscles | Abductor digiti minimi, flexor digiti minimi, opponens digiti minimi |
| Lumbricals 3 & 4 (ulnar two) | Ring and little finger MCP flexion, IP extension |
| All interossei (7 total) | PAD = Palmar Adduct, DAB = Dorsal ABduct |
| Adductor pollicis | Adducts thumb (key for grip) |
| Flexor pollicis brevis (deep head) | Flexes thumb |
| Palmaris brevis | Wrinkles hypothenar skin |
Sensory Supply
- Palmar surface: Medial 1½ fingers (little finger + ulnar half of ring)
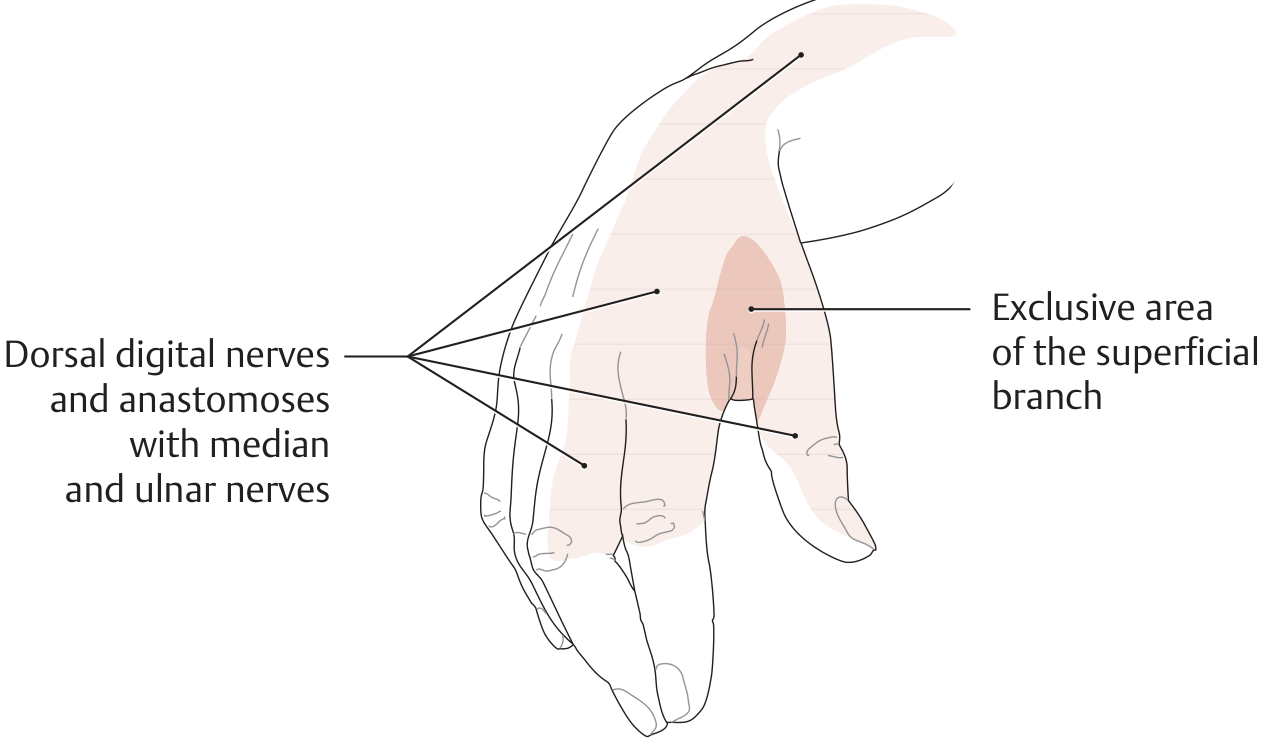
- Dorsal branch: Medial dorsum of hand, little finger (exclusive territory - green in image above)
CLINICAL SCENARIO 3: Ulnar Nerve Injury at Elbow (Cubital Tunnel)
"Ulnar nerve palsy is the most common peripheral nerve paralysis. The characteristic feature is a 'claw hand' deformity, in which loss of the interosseous muscles causes the fingers to be hyperextended at the MCPs and slightly flexed at the PIPs/DIPs."
- Ring and little fingers claw (ulnar 2 lumbricals lost) - MCP hyperextension + IP flexion
- Index and middle less clawed (median nerve lumbricals 1&2 partially compensate)
- Guttering - visible hollowing between metacarpals (interossei atrophy, especially 1st web space)
- Hypothenar wasting
- Weak pinch grip (adductor pollicis lost)
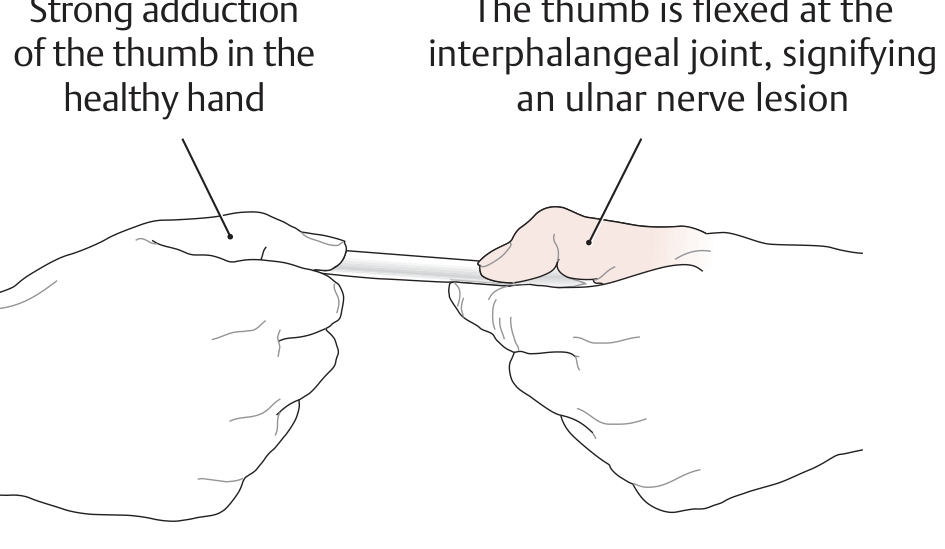
- Positive Froment sign (shown below):
Paradox of clawing: High ulnar nerve lesion (at elbow) = LESS clawing than low lesion (at wrist). Because at elbow, FDP to ring and little finger is also lost - so fingers can't flex into a claw. At wrist, FDP is intact, making the claw more pronounced. This is Ulnar Paradox.
CLINICAL SCENARIO 4: Ulnar Nerve at Wrist (Guyon's Canal)
| Feature | At Elbow | At Wrist (Guyon's Canal) |
|---|---|---|
| Claw hand | Less pronounced | More pronounced (Ulnar paradox) |
| Hypothenar sensation | Lost | Spared (palmar cutaneous branch exits proximal to canal) |
| FCU weakness | Yes | No |
| FDP ring/little weakness | Yes | No |
NERVE 3: RADIAL NERVE (C5-C8)
At the Hand Level - Sensory ONLY
Motor at Forearm Level (affecting hand function):
- All wrist extensors (ECRL, ECRB, ECU)
- Finger extensors (EDC, EIP, EDM)
- Thumb extensors and abductor (EPL, EPB, APL)
CLINICAL SCENARIO 5: Radial Nerve Injury - "Saturday Night Palsy"
"When the radial nerve is damaged, the patient can no longer actively extend the hand at the wrist - wrist drop (drop hand) is present. Sensory loss on the radial surface of the dorsum and on the extensor surface of the thumb, index finger, and the radial half of the middle finger extending to the PIP joint."
- Cannot extend wrist (wrist drop)
- Cannot extend MCP joints of fingers
- Cannot extend/abduct thumb
- Triceps usually spared (branches to triceps leave radial nerve before spiral groove)
- Minimal sensory loss - only 1st dorsal web space (easily compensated by overlap)
| Site | Cause | Features |
|---|---|---|
| Axilla | Crutch palsy, axillary fracture | Triceps + wrist drop |
| Spiral groove | Midshaft humerus fracture, Saturday night palsy | Wrist drop, triceps SPARED |
| Lateral epicondyle (PIN) | Posterior interosseous nerve entrapment | Finger drop, wrist extensors SPARED |
| Wrist (superficial radial) | Handcuff neuropathy, de Quervain surgery | Sensory only - 1st web space |
Quick Comparison Table
| Feature | Median | Ulnar | Radial |
|---|---|---|---|
| Root values | C6-T1 | C8-T1 | C5-C8 |
| Thenar muscles | Yes (LOAF) | Only FPB deep head | No |
| Hypothenar muscles | No | Yes | No |
| Interossei | No | Yes (all 7) | No |
| Intrinsic hand motor | Partial | Most | None |
| Thumb opposition | Median | - | - |
| Thumb adduction | - | Ulnar | - |
| Wrist extension | No | No | Radial |
| Sensory (palm) | Lateral 3½ fingers | Medial 1½ fingers | Minimal |
| Sensory (dorsum) | Fingertips of 3½ | Medial dorsum | Radial dorsum (proximal) |
| Classic deformity | Ape hand / Benediction | Claw hand | Wrist drop |
| Common entrapment | Carpal tunnel | Cubital tunnel | Spiral groove |
| Special test | Tinel's, Phalen's | Froment's sign | - |
Important Anastomoses (Exam Favorites)
- Martin-Gruber anastomosis: Median → Ulnar nerve in forearm (prevalence 1-17%). Can cause atypical CTS presentations.
- Riche-Cannieu anastomosis: Ulnar → Median deep motor branch in palm. Can allow ulnar nerve to supply thenar muscles.
Neve suppy of hand with images illustrations clinical pearls of nerve damge entrapment
Hand Nerve Supply - Illustrated Guide with Clinical Pearls
1. MEDIAN NERVE (C6-T1)
Origin & Course
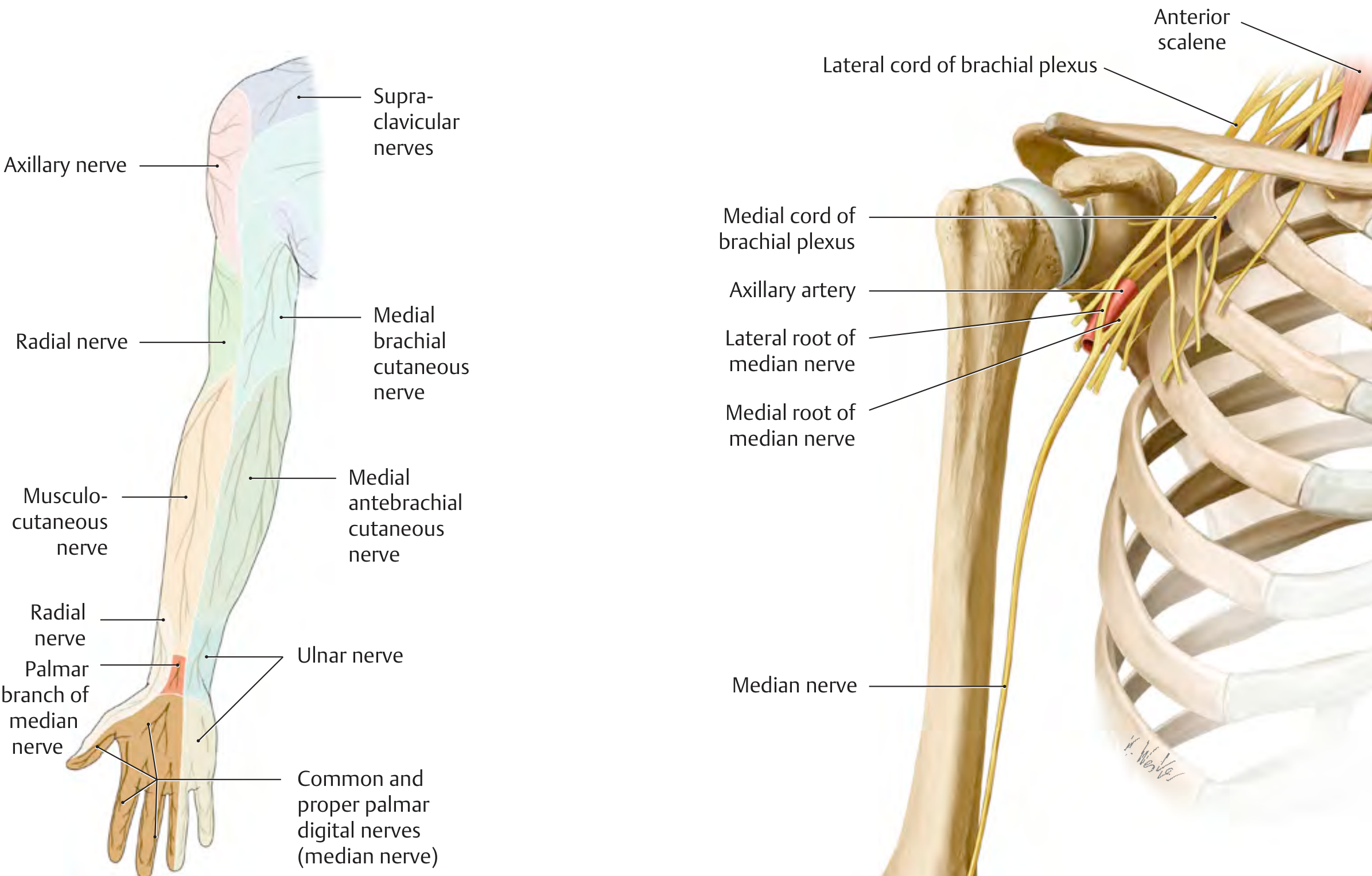
Complete Motor & Sensory Course
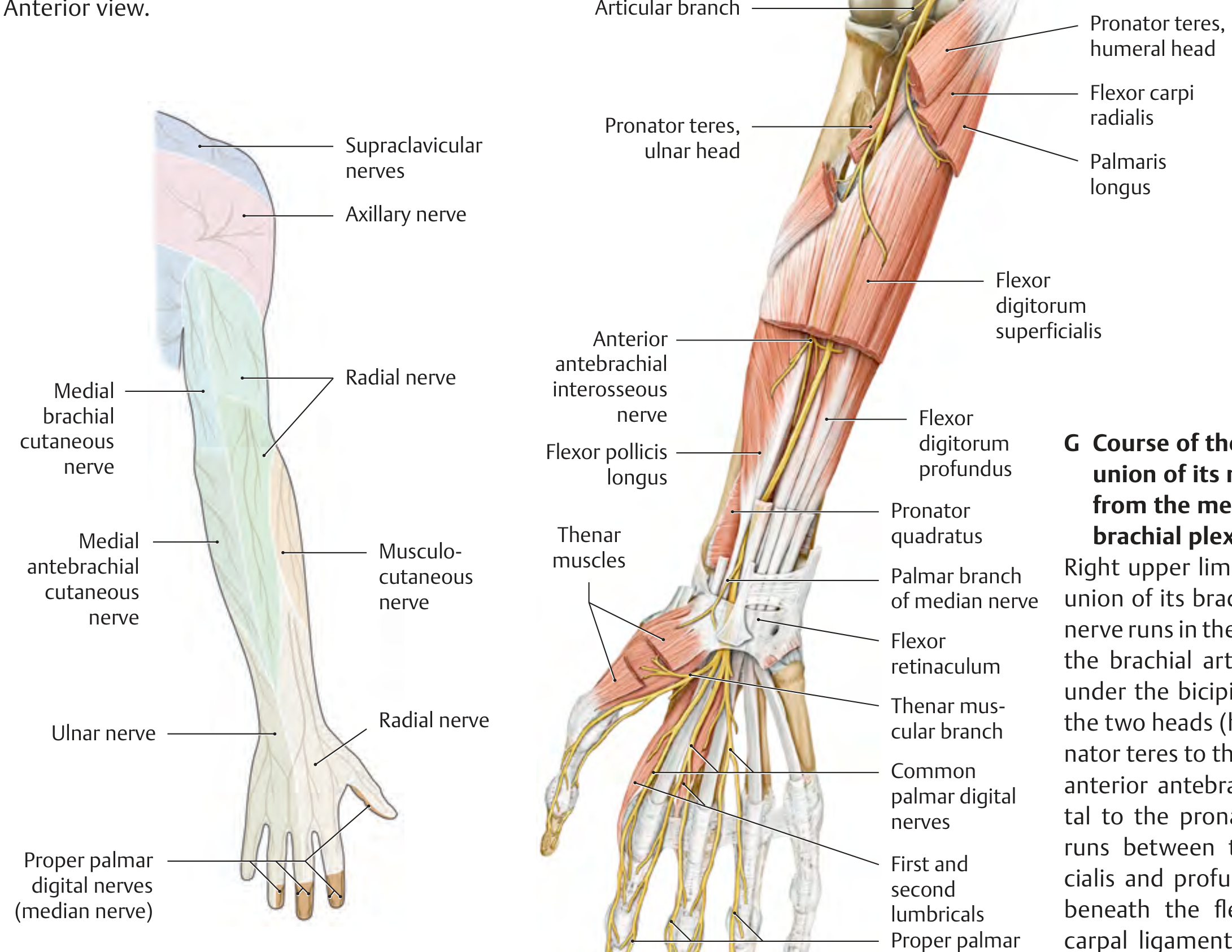
- Lumbricals 1 & 2 (radial two)
- Opponens pollicis
- Abductor pollicis brevis
- Flexor pollicis brevis (superficial head)
🔴 Clinical Pearl 1: Carpal Tunnel Syndrome (CTS)
- Thenar wasting (APB atrophy visible as flat thumb base)
- Tinel's sign: Tapping wrist → tingling in median territory
- Phalen's test: Wrist flexion 60 sec → symptoms reproduced
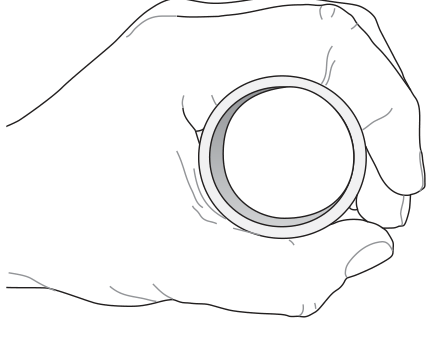
- Bottle sign (positive): Cannot fully encircle a cylindrical object
🔴 Clinical Pearl 2: Hand of Benediction (Proximal Median Nerve Injury)
🔴 Clinical Pearl 3: Anterior Interosseous Nerve (AIN) Syndrome
- Branch of median nerve in proximal forearm
- No sensory loss (pure motor nerve)
- Loss of: FPL (can't flex thumb IP), FDP to index/middle (can't flex DIP of index)
- Classic test: "OK sign" - patient makes pinch between thumb and index fingertip; in AIN palsy, they form a triangle instead of a circle because FPL + FDP index both fail
- Cause: Forearm trauma, Parsonage-Turner syndrome
2. ULNAR NERVE (C8-T1)
Origin & Course
Sensory Distribution - Dorsum
- All interossei (4 palmar, 3 dorsal) - PAD (Palmar = Adduct), DAB (Dorsal = ABduct)
- Lumbricals 3 & 4 (ulnar two)
- All hypothenar muscles (AbDM, FDM, OpDM)
- Adductor pollicis - key for grip
- FPB deep head, Palmaris brevis
🔴 Clinical Pearl 4: Claw Hand (Ulnar Nerve Palsy)
🔴 Clinical Pearl 5: The Ulnar Paradox
| Level of Injury | Clawing Severity | Why |
|---|---|---|
| High (elbow) | Less clawing | FDP to ring/little also paralyzed - no flexor to pull IPs into flexion |
| Low (wrist) | More clawing | FDP intact, acts unopposed on now-unbalanced fingers |
"The higher the ulnar nerve lesion, the less the claw" - this is paradoxical because you'd expect more damage = worse deformity.
🔴 Clinical Pearl 6: Froment's Sign
- Normal: Adductor pollicis (ulnar nerve) holds it - thumb IP joint stays straight
- Ulnar palsy: Adductor pollicis fails → FPL (median nerve) compensates → thumb IP flexes = positive Froment sign
🔴 Clinical Pearl 7: Cubital Tunnel vs. Guyon's Canal
| Feature | Cubital Tunnel (Elbow) | Guyon's Canal (Wrist) |
|---|---|---|
| FCU weakness | Yes | No |
| FDP (ring/little) | Weak | Normal |
| Hypothenar sensation | Lost | Spared (palmar branch exits before canal) |
| Dorsal ulnar sensation | Lost | Spared (dorsal branch exits before wrist) |
| Clawing | Less (Ulnar paradox) | More |
| Causes | Leaning on elbow, cubitus valgus, fracture | Hook of hamate fracture, cyclist's palsy, ganglion |
3. RADIAL NERVE (C5-C8)
Origin & Course
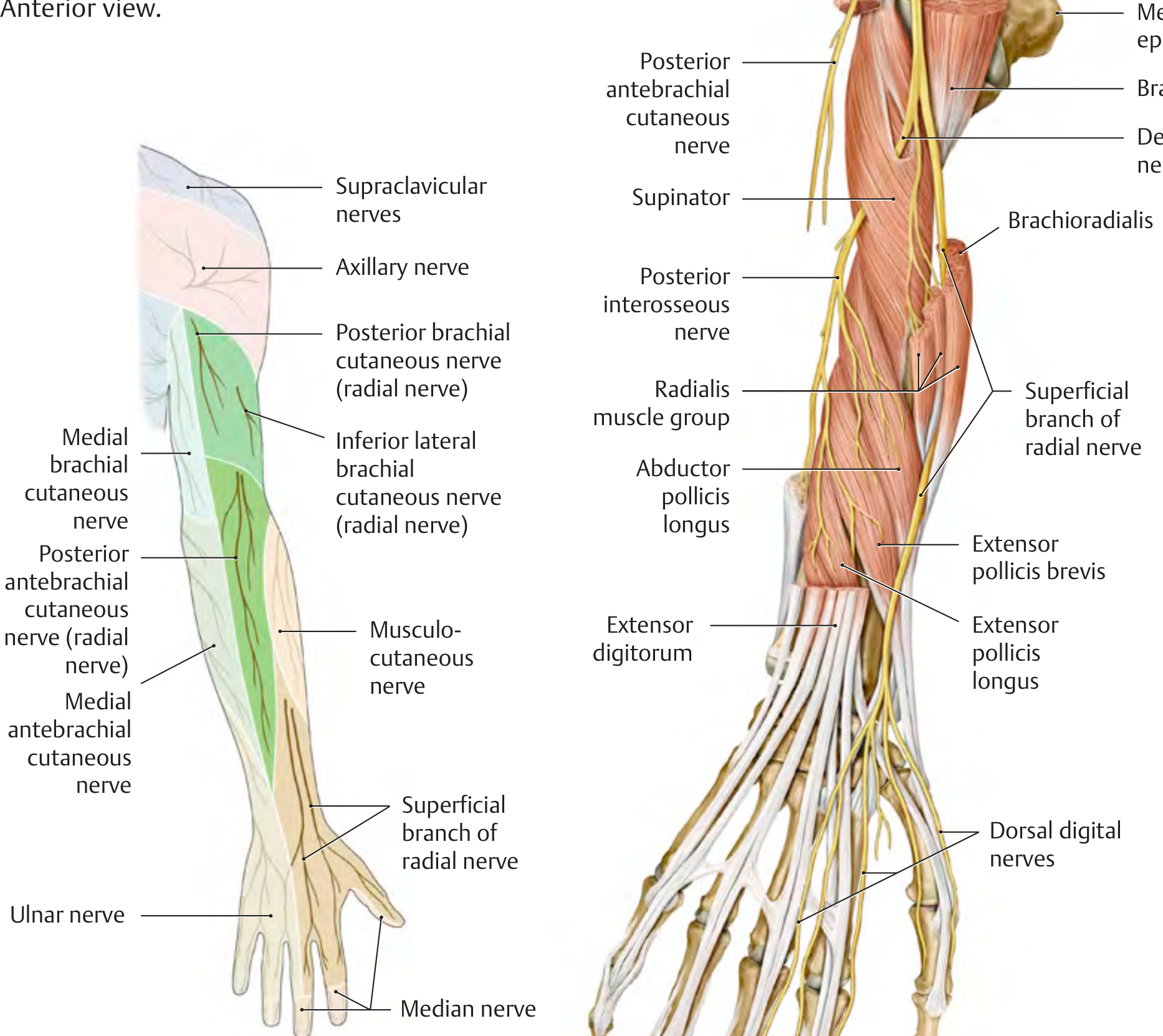
- Deep branch (PIN) → through supinator canal → all finger/thumb extensors
- Superficial branch → purely sensory → dorsum of hand
Sensory Exclusive Zone
🔴 Clinical Pearl 8: Wrist Drop by Level
| Level of Injury | Cause | Triceps | Wrist Extension | Finger Extension | Sensory Loss |
|---|---|---|---|---|---|
| Axilla | Crutch palsy, axillary fracture | Paralysed | Lost | Lost | Posterior arm + dorsum |
| Spiral groove (mid-humerus) | Saturday night palsy, midshaft # humerus | Spared | Lost | Lost | Dorsum of hand |
| Lateral epicondyle (PIN) | Radial tunnel, head of radius fracture | Spared | Spared (ECRL) | Lost (finger drop) | None or minimal |
| Wrist (superficial branch) | Handcuffs, tight watch, de Quervain surgery | Spared | Spared | Spared | 1st web space only |
Combined Sensory Map Summary
Dorsum of Hand
🎯 Master Clinical Pearls Summary
| Nerve | Injury | Deformity | Sensory Loss | Key Test |
|---|---|---|---|---|
| Median - high | Elbow/supracondylar # | Hand of benediction | Lateral 3½ palm | Bottle sign |
| Median - low | Carpal tunnel | Ape hand (thenar wasting) | Lateral 3½ fingers (thenar skin SPARED) | Tinel's, Phalen's |
| Median - AIN | Forearm | No deformity at rest | None | Failed OK sign |
| Ulnar - high | Cubital tunnel (elbow) | Mild claw (ring+little) | Medial 1½ + dorsal medial | Froment's |
| Ulnar - low | Guyon's canal (wrist) | Severe claw (ulnar paradox) | Medial 1½ fingers only (dorsal SPARED) | Froment's |
| Radial - axilla | Crutch palsy | Wrist drop + triceps weak | Posterior arm + dorsum | - |
| Radial - spiral groove | Saturday night palsy | Wrist drop, triceps OK | Dorsum of hand | - |
| Radial - PIN | Radial tunnel | Finger drop, NO wrist drop | None | - |
| Radial - wrist | Handcuff neuropathy | None | 1st dorsal web space only | - |

What is costochondritis vs tietze syndrome
Question 49 Answer: A - Tietze Syndrome ✓
Costochondritis vs. Tietze Syndrome - Complete Comparison
"Tietze syndrome is manifested by painful swelling of one or more costochondral articulations... The term costochondritis is often used interchangeably with Tietze syndrome, but some authors restrict the latter term to pain of the costochondral articulations with swelling."
| Feature | Tietze Syndrome | Costochondritis |
|---|---|---|
| Key distinguishing feature | Swelling at costochondral junction ✓ | No swelling |
| Age of onset | <40 years | >40 years |
| Sex | Equal (M = F) | More common in women |
| Joints affected | Usually 1 joint (2nd or 3rd CJ most common) | Multiple joints - 3rd, 4th, 5th most common |
| Tenderness | Present | Present |
| Radiation | To arm/shoulder | To arm/shoulder |
| Aggravating factors | Coughing, sneezing, deep breath, twisting | Same |
| Nature | Benign, self-limiting | Benign, self-limiting |
| Treatment | NSAIDs, local steroid injection | NSAIDs, local steroid injection |
Why the Question Answer is Tietze (not Costochondritis)
- The post-infectious/post-respiratory context (coughing from pneumonia) is a classic precipitant of Tietze
- The word "tenderness" + specific localization = clinical Tietze presentation
- The question book's explanation states Tietze is "characterized by..." (shown cut off at bottom of image)
The ONE-LINE distinction for exams:
- Tietze = Tenderness + SWELLING (the "TE" in TiETze = Think Edema/swelling)
- Costochondritis = Tenderness ONLY, no swelling
Additional Differentials to Exclude (from Harrison's)
| Condition | How to distinguish |
|---|---|
| MI | ECG changes, troponin rise, radiation to jaw/left arm, diaphoresis |
| Pleurisy | Pleural rub on auscultation, worsened by breathing, not by palpation |
| Intercostal muscle spasm | Pain along rib, not specifically at costochondral junction |
| Herpes zoster | Dermatomal rash, burning pain before vesicles |
| Xiphoidalgia | Pain at xiphoid process only |
| Slipping rib syndrome | Ribs 9-10, pain reproduced by hooking fingers under rib and pulling caudally |
| Malignancy | Weight loss, persistent, worsening, no response to NSAIDs |
Treatment (Both Conditions)
- Analgesics/NSAIDs (ibuprofen, naproxen) - first line
- Local corticosteroid injection into tender joint - for refractory cases
- Rest from aggravating activities
- Reassurance - both are benign self-limiting conditions; very important as they can mimic cardiac pain and cause significant anxiety
Costochindritis vs tietz sy dromw
Costochondritis vs Tietze Syndrome - Quick Revision Card
The ONE Key Difference
TIETZE = Pain + SWELLING at costochondral junction
COSTO = Pain ONLY, NO swelling
| Feature | Tietze Syndrome | Costochondritis |
|---|---|---|
| Swelling | YES (defining feature) | NO |
| Age | < 40 years | > 40 years |
| Sex | M = F (equal) | More in women |
| Joints | Usually 1 joint (2nd/3rd) | Multiple (3rd, 4th, 5th) |
| Tenderness | Yes | Yes |
| Radiation | Arm/shoulder | Arm/shoulder |
| Precipitants | Coughing, trauma, post-infection | Repetitive movements |
| Treatment | NSAIDs + local steroid injection | NSAIDs + local steroid injection |
Memory Tricks
🔑 "TiETzE" = Think Edema (swELLing)
🔑 "CoSTo" = Cost-no-swelling (no extra feature)
🔑 Tietze is YOUNGER, FEWER joints, HAS swelling
🔑 Costochondritis is OLDER, MORE joints, NO swelling
Exam Trap Points
- Both mimic cardiac/pulmonary pain - must always rule out MI, pleurisy first
- Tietze - pain reproduced by palpation of the costochondral junction (this distinguishes it from cardiac pain)
- Costochondritis - thenar skin over costochondral junctions is NORMAL in color (no redness)
- Both are benign and self-limiting - reassurance is part of treatment
- If a question says "swelling at 2nd costal cartilage" → Tietze
- If a question says "multiple tender costochondral junctions, no swelling" → Costochondritis
Why Tietze Happens After Pneumonia/Coughing
- Respiratory infections (pneumonia, URTI, bronchitis)
- Post-cardiac surgery (sternotomy)
- Trauma to chest wall
Question 60 Answer: B - 0.1 mL/kg of 1:10,000 (10 mcg/kg)
Full Explanation: Adrenaline (Epinephrine) in Pediatric Cardiac Arrest
The Dose
Understanding the Concentrations
| Concentration | Meaning | mg per mL | Use |
|---|---|---|---|
| 1:1,000 | 1 g in 1,000 mL | 1 mg/mL | IM for anaphylaxis |
| 1:10,000 | 1 g in 10,000 mL | 0.1 mg/mL | IV cardiac arrest |
| 1:100,000 | 1 g in 100,000 mL | 0.01 mg/mL | Local anesthesia additive |
Calculating the Volume for IV Cardiac Arrest
- Required dose = 0.01 mg/kg
- Using 1:10,000 concentration = 0.1 mg/mL
- Volume = dose ÷ concentration = 0.01 mg/kg ÷ 0.1 mg/mL = 0.1 mL/kg ✓
Why the Other Options Are Wrong
| Option | Problem |
|---|---|
| A: 0.01 mL/kg of 1:1000 | = 0.01 mcg/kg - 100x underdose |
| B: 0.1 mL/kg of 1:10,000 ✓ | = 10 mcg/kg = correct PALS dose |
| C: 0.1 mL/kg of 1:100,000 | = 1 mcg/kg - 10x underdose |
| D: 0.01 mL/kg of 1:10,000 | = 1 mcg/kg - 10x underdose |
| E: 1 mL/kg of 1:1000 | = 1 mg/kg - 100x overdose - DANGEROUS |
Clinical Pearls - Epinephrine in Codes
PALS vs ACLS Dose
| Scenario | Dose | Concentration | Volume |
|---|---|---|---|
| Pediatric cardiac arrest (PALS) | 0.01 mg/kg (10 mcg/kg) IV | 1:10,000 | 0.1 mL/kg |
| Adult cardiac arrest (ACLS) | 1 mg flat dose IV | 1:10,000 | 10 mL |
| Pediatric ET tube (if no IV) | 0.1 mg/kg | 1:1,000 | 0.1 mL/kg |
| Anaphylaxis (IM) | 0.01 mg/kg (max 0.5 mg) | 1:1,000 | 0.01 mL/kg |
Repeat Dosing
- Repeat every 3-5 minutes during CPR
- No maximum number of doses in arrest
- Give AFTER defibrillation in shockable rhythms (VF/pVT)
- Give immediately in non-shockable rhythms (asystole/PEA)
Important Memory Trick
"For IV cardiac arrest in children: 0.1 mL/kg of 1:10,000"Both numbers start with 0.1 - easy to remember together
The 1:10,000 vs 1:1,000 Safety Rule
- 1:1,000 (1 mg/mL) is NEVER given IV directly in cardiac arrest dosing - it would be a 10x overdose
- Always dilute to 1:10,000 for IV use, OR use the pre-drawn 1:10,000 cardiac syringes
- 1:1,000 IM is correct for anaphylaxis only
No its 1 mcg/kg
PALS epinephrine dose pediatric cardiac arrest IV mcg/kg 2024 guidelines
The PALS Epinephrine Dose is 10 mcg/kg - Confirmed
"Epinephrine IV/IO dose: 0.01 mg/kg (0.1 mL/kg of the 0.1 mg/mL concentration). Max dose 1 mg. Repeat every 3-5 minutes."
Unit Conversion - Why This Matters
| Value | Unit | Same dose? |
|---|---|---|
| 0.01 mg/kg | mg | ✓ |
| 10 mcg/kg | mcg | ✓ Same thing |
| 1 mcg/kg | mcg | ✗ This is 10x less - underdose |
- 1 mg = 1000 mcg
- So 0.01 mg = 10 mcg
- Therefore 0.01 mg/kg = 10 mcg/kg
Where 1 mcg/kg IS Used (Different Clinical Context)
| Use | Dose | Route |
|---|---|---|
| Epinephrine infusion (vasopressor/inotrope in shock) | 0.1-1 mcg/kg/min (infusion) | IV drip |
| Bradycardia with pulse (not arrest) | 0.01 mg/kg (same as arrest) | IV |
| Anaphylaxis (IM) | 0.01 mg/kg = 10 mcg/kg | IM |
Summary
| Scenario | Correct Dose |
|---|---|
| Pediatric cardiac ARREST (IV/IO) | 0.01 mg/kg = 10 mcg/kg |
| Pediatric cardiac arrest (via ET tube) | 0.1 mg/kg = 100 mcg/kg |
| Epinephrine infusion for shock | 0.1-1 mcg/kg/min (continuous) |
| Adult cardiac arrest | 1 mg flat dose |
Sorry my bad i read anaphylaxis
Epinephrine Dosing: Cardiac Arrest vs Anaphylaxis
| Scenario | Dose | Route | Concentration |
|---|---|---|---|
| Cardiac Arrest (PALS) | 0.01 mg/kg = 10 mcg/kg | IV/IO | 1:10,000 (0.1 mg/mL) → 0.1 mL/kg |
| Anaphylaxis (pediatric) | 0.01 mg/kg = 10 mcg/kg (max 0.5 mg) | IM (thigh) | 1:1,000 (1 mg/mL) → 0.01 mL/kg |
| Anaphylaxis infusion (refractory) | 0.1-1 mcg/kg/min | IV infusion | Diluted |
| ET tube (no IV access) | 0.1 mg/kg = 100 mcg/kg | Endotracheal | 1:1,000 |
Key Pearls
The DOSE is the same for arrest and anaphylaxis (0.01 mg/kg) - but the ROUTE and CONCENTRATION differ:
- Arrest → IV, using 1:10,000
- Anaphylaxis → IM, using 1:1,000
Anaphylaxis-Specific Notes
- IM into the outer mid-thigh (vastus lateralis) - NOT deltoid, NOT SC
- Repeat every 5-15 minutes if no response
- 1 mcg/kg you mentioned is the IV infusion starting rate used when IM epinephrine fails and the patient needs ICU-level vasopressor support
- Auto-injectors (EpiPen): 0.15 mg for <25 kg; 0.3 mg for >25 kg