Epidemiology of measles
Reading File
Finding Sources
Finding Sources
Searching PubMed
"measles" AND "epidemiology"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Epidemiology of Measles
Agent
Measles (rubeola) is caused by the measles virus, an enveloped, single-stranded RNA virus of the genus Morbillivirus, family Paramyxoviridae. There is only one serotype, and immunity after infection is lifelong. The virus is easily inactivated by dryness and acid. Humans are the only natural host - there is no animal reservoir.
- Medical Microbiology 9e, p. 542
- Red Book 2021, p. 799
Global Burden
-
Before widespread vaccination, an estimated 2.6 million measles deaths occurred annually (1980 figure).
-
In the pre-vaccine era, approximately 90% of Americans were infected before age 15.
-
Vaccination programs reduced measles-related deaths by 73% and cases by 76% from 2000 to 2018.
-
Despite this, measles still caused an estimated 9.7 million cases and >140,000 deaths in 2018 alone.
-
Measles accounts for approximately 2% of all under-five mortality worldwide.
-
By end of 2018, 89% of children globally had received at least one dose of measles vaccine by their second birthday.
-
Park's Textbook of Preventive & Social Medicine, p. 166-167
-
Red Book 2021, p. 800
Transmission
| Feature | Detail |
|---|---|
| Route | Inhalation of respiratory large-droplet aerosols; less commonly, true airborne spread |
| Infectivity | ~90% attack rate among susceptible contacts in close-contact settings |
| Basic reproduction number (R₀) | Estimated 12-18, one of the highest of any infectious disease |
| Infectious period | 4 days before rash onset through 4 days after rash appearance |
| Airborne survival | Infectious droplets can remain airborne for up to 2 hours |
- Red Book 2021, p. 799
- Fitzpatrick's Dermatology, p. 3019
Incubation Period
- 8-12 days from exposure to onset of prodromal symptoms (cough, coryza, conjunctivitis)
- Average interval between rash in index case and secondary cases: 14 days (range 7-21 days)
- For SSPE (late complication), mean incubation is 10.8 years
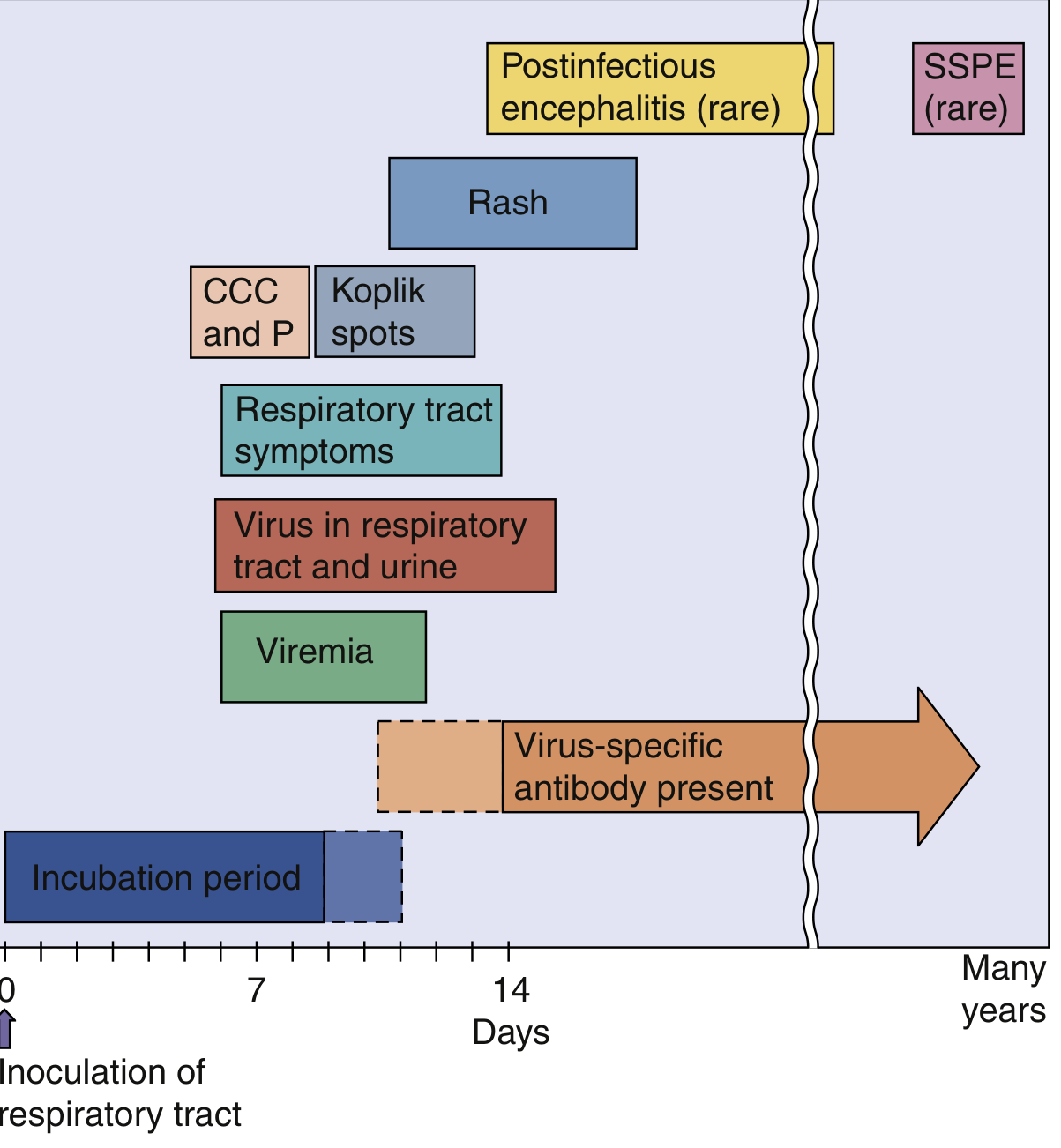
Fig. Time course of measles infection. CCC and P = cough, conjunctivitis, coryza, and photophobia (prodrome). SSPE appears many years later.
Herd Immunity Threshold
-
Population immunity of ≥95% is required to interrupt ongoing transmission - a threshold higher than almost any other vaccine-preventable disease.
-
Epidemics tend to arise when susceptibles reach approximately 40% of the population.
-
When measles is introduced into a previously unexposed ("virgin") population, >90% of that community will be infected.
-
Park's Textbook, p. 166
Seasonality and Geography
- Worldwide distribution: endemic in virtually all parts of the world.
- In temperate climates: peak incidence during late winter and spring, likely related to indoor crowding.
- In tropical/developing countries: year-round transmission with less pronounced seasonality.
- Highest burden remains in sub-Saharan Africa and South/Southeast Asia.
Age Distribution (Shifting Epidemiology)
This is one of the most important epidemiological features:
| Era | Predominant age group affected |
|---|---|
| Pre-vaccine era | Preschool and young school-age children (nearly universal infection by age 20) |
| Post-vaccine era (routine single dose) | Shift to infants <1 year (before maternal antibodies wane) AND older adolescents/adults (primary vaccine failure or unvaccinated) |
| Current outbreaks | Adolescents and adults, particularly in undervaccinated or vaccine-hesitant communities |
- Maternal antibodies protect infants in the first months of life, but once they wane, infants become susceptible before vaccination age.
- The Red Book 2021 notes that primary vaccine failure (inadequate response to a single dose) occurs in up to 7% of recipients - the main reason a two-dose schedule was adopted.
High-Risk Groups
- Unvaccinated individuals, especially infants <1 year
- Malnourished children, particularly those with vitamin A deficiency (worse outcomes, higher case-fatality)
- Immunocompromised patients (HIV, leukemia, severe malnutrition) - may lack the characteristic rash; can have prolonged viral shedding
- Pregnant women - increased case-fatality
- Children infected before age 2 - highest rates of SSPE
Case-Fatality Rate (CFR)
- In the US post-elimination era: 1-3 deaths per 1,000 cases
- In developing countries: CFR is substantially higher, particularly in malnourished populations
- Main causes of death: respiratory complications (pneumonia, croup) and neurological complications (encephalitis)
Complications Affecting Epidemiology
| Complication | Frequency |
|---|---|
| Otitis media, bronchopneumonia | Common, especially in young children |
| Acute encephalitis | ~1 per 1,000 cases (often causes permanent brain damage) |
| SSPE (subacute sclerosing panencephalitis) | 4-11 per 100,000 measles cases overall; up to ~1 per 1,000 in some recent studies; risk highest if infected <2 years of age |
| Measles inclusion body encephalitis (MIBE) | Rare; in immunocompromised, within 1 year of infection |
- Red Book 2021, p. 799
An underappreciated epidemiological consequence: measles causes long-term immune amnesia, blunting immune responses to other pathogens for months to years after recovery and increasing all-cause childhood mortality even without direct measles-related death.
Challenges to Elimination
The WHO Global Measles and Rubella Strategic Plan identified these as major barriers:
- Weak immunization systems
- High infectivity of measles virus (R₀ 12-18)
- Populations inaccessible due to conflict or geography
- Growing vaccine hesitancy and refusal
- Shifting epidemiology - increasing transmission among adolescents and adults
- Gaps in financial and human resources at country and global levels
Measles in India
-
Prior to the Universal Immunization Programme (UIP), cyclical outbreaks occurred every 3 years.
-
Vaccination coverage has extended inter-epidemic intervals and reduced peak intensity.
-
In 1987, approximately 2.47 lakh (247,000) cases were reported; by 2018 this fell to 20,895 cases with 34 deaths.
-
Persistent hotspots remain in tribal, remote, and conflict-affected areas.
-
States most affected in 2018: West Bengal, Assam, Jammu & Kashmir, Maharashtra.
-
Park's Textbook, p. 167
WHO Targets for Elimination
The 2010 World Health Assembly set these milestones:
- MCV1 (first dose) routine coverage of ≥90% nationally and ≥80% in every district
- Annual measles incidence of <5 cases per million
- ≥95% reduction in measles mortality compared to year 2000 levels
Vaccination and Control
| Vaccine | Detail |
|---|---|
| Type | Live attenuated (Schwartz or Moraten variants of Edmonston B strain) |
| Schedule | Two doses: first at 9-15 months, second dose at 15-24 months or school entry (country-specific) |
| Efficacy | Single dose: ~93%; Two doses: ~97% |
| Post-exposure prophylaxis | Immune serum globulin within 6 days of exposure for high-risk contacts; MMR vaccine within 72 hours |
- Medical Microbiology 9e, p. 542
Recent Evidence (2023-2026)
A 2024 systematic review and meta-analysis (PMID 39227789) examining measles outbreaks in Ethiopia from 2000-2023 confirmed that under-five children, unvaccinated status, and low vaccination coverage remain the dominant epidemiological risk factors in sub-Saharan Africa. A companion 2024 meta-analysis on vaccine effectiveness in African children (PMID 39574018) confirmed high but sub-optimal vaccine effectiveness in some African settings, reinforcing the need for two-dose schedules.
Summary: Measles is one of the most contagious human pathogens (R₀ 12-18, 90% attack rate), requiring >95% population immunity for herd protection. Vaccination has reduced global deaths by over 70%, but pockets of vaccine hesitancy, conflict zones, and immunization infrastructure gaps continue to sustain outbreaks. The epidemiology has shifted from a universal childhood disease to one disproportionately affecting unvaccinated infants, adolescents, adults, and immunocompromised individuals.
This is a shared conversation. Sign in to Orris to start your own chat.