Biochemical tests
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Now I have enough material from the medical library to compile a thorough, well-organized answer. Here is the comprehensive overview:
Biochemical Tests - A Comprehensive Overview
Biochemical tests (also called clinical chemistry or laboratory investigations) measure specific substances in blood, urine, or body fluids to assess organ function, metabolic status, and disease. The major panels are covered below.
1. Liver Function Tests (LFTs)
The liver is conceptualized as three functional systems, each tested differently:
A. Hepatocyte Injury Markers (Chemical-Metabolic System)
| Test | Normal Role | Significance |
|---|---|---|
| AST (Aspartate Aminotransferase) | Hepatocyte enzyme | Rises markedly in acute hepatitis, infarction, trauma |
| ALT (Alanine Aminotransferase) | Hepatocyte enzyme (more liver-specific) | Same as AST; ALT more specific to liver |
| LDH (Lactate Dehydrogenase) | Metabolic enzyme | Elevated in hepatocyte injury and mass lesions |
In hepatitis, AST/ALT rise dramatically but protein synthesis is preserved (less than 80% of liver destroyed).
B. Synthetic Function Markers
| Test | Normal Role | Significance |
|---|---|---|
| Total Protein & Albumin | Liver synthesizes >90% of body proteins | Falls only when >80% of liver is destroyed (cirrhosis, fulminant failure) |
| Ammonia (NH3) | Liver converts NH3 to urea via urea cycle | Rises in severe failure (>80% destruction); causes hepatic encephalopathy |
| Prothrombin Time (PT) | Clotting factors made in liver | Prolonged in liver failure |
C. Biliary/Canalicular Markers
| Test | Normal Role | Significance |
|---|---|---|
| Direct (Conjugated) Bilirubin | Secreted into bile canaliculi | Rises with biliary obstruction or hepatocyte injury |
| Indirect (Unconjugated) Bilirubin | Pre-hepatic product from RBC breakdown | Rises in hemolysis or severe hepatocyte injury |
| ALP (Alkaline Phosphatase) | Canalicular surface enzyme | Elevated in biliary obstruction and space-occupying lesions |
| GGT (Gamma-Glutamyltransferase) | Hepatic surface enzyme | Elevated with biliary obstruction; sensitive to alcohol |
| 5'-Nucleotidase (5'-N) | Biliary enzyme | Confirms hepatic origin of ALP elevation |
Six Classic LFT Patterns
| Condition | AST/ALT | ALP/GGT | Bilirubin | Albumin | Ammonia |
|---|---|---|---|---|---|
| Acute Hepatitis | ↑↑↑ | ↑ | ↑ (both) | Normal | Normal |
| Cirrhosis | Normal/low | ↑ | ↑ (both) | ↓↓ | ↑ |
| Biliary Obstruction | Normal | ↑↑ | ↑ direct | Normal | Normal |
| Space-Occupying Lesions | Normal | ↑↑ (ALP+LDH) | Normal | Normal | Normal |
| Passive Congestion | Mildly ↑ | ↑ | ↑ (severe cases) | Normal | Normal |
| Fulminant Hepatic Failure | ↑↑↑↑ (>10,000) | ↑ | ↑ | ↓↓ | ↑↑ |
- Henry's Clinical Diagnosis and Management by Laboratory Methods, pp. 139-141
- Harper's Illustrated Biochemistry, 32nd Ed
2. Renal Function Tests
The kidney is assessed by measuring filtration (glomerular function) and concentrating ability (tubular function).
A. Blood Urea Nitrogen (BUN)
- BUN is inversely proportional to GFR: BUN ∝ 1/GFR
- Reference range: 10-20 mg/dL
- Limitation: affected by hydration status, catabolic state, and diet
B. Serum Creatinine
- Reference range: ~0.5-1.0 mg/dL
- Filtered and excreted; serum creatinine rises as GFR falls
- Important: a 75% reduction in GFR may cause only a modest rise in creatinine (non-linear relationship - see figure below)
C. BUN/Creatinine Ratio (key diagnostic tool)
| Pattern | BUN/Cr Ratio | Interpretation |
|---|---|---|
| Normal | 10:1 to 20:1 | Normal |
| Disproportionate BUN rise | >20:1 | Prerenal - reduced renal perfusion (renal artery stenosis, dehydration, heart failure) |
| Both rise proportionately | 10:1 to 20:1 | Renal or Postrenal - true parenchymal disease or obstruction |
D. GFR & Creatinine Clearance
GFR = CrCl = (Urine Creatinine × Urine Volume) / Plasma Creatinine
Estimated GFR (eGFR) is now calculated using CKD-EPI or MDRD equations, which account for age, sex, and race.
E. Urine Tests for Renal Function
| Test | Significance |
|---|---|
| Urine specific gravity (1.001-1.035) | Assesses concentrating ability |
| Urine osmolality | Normal: 50-1,000 mOsm/kg |
| Uosm/Posm ratio | >1.2 = normal concentrating ability; <1.2 = tubular defect |
| Urine sodium | <20 mEq/L = prerenal; >40 mEq/L = AKI/tubular damage |
| FENa (fractional excretion of Na) | <1% = prerenal; >2% = intrinsic renal failure |
| Proteinuria | Glomerular vs tubular vs overflow proteinuria |
- Henry's Clinical Diagnosis and Management by Laboratory Methods, pp. 137-138
- Barash's Clinical Anesthesia, 9e
3. Thyroid Function Tests (TFTs)
| Test | What It Measures | Interpretation |
|---|---|---|
| TSH (Thyroid Stimulating Hormone) | Pituitary drive | Best initial screening test; ↑ in hypothyroidism, ↓ in hyperthyroidism |
| Free T4 (fT4) | Active thyroxine, unbound | Low in hypothyroidism; elevated in hyperthyroidism |
| Free T3 (fT3) | Active triiodothyronine | More potent than T4; low in hypothyroidism |
| Total T4 | Less useful | Affected by thyroid-binding globulin changes; seldom used now |
-
TSH is the most sensitive and first-line test
-
Free T4 and free T3 are preferred over total levels because they are unaffected by changes in binding proteins
-
Harper's Illustrated Biochemistry, 32nd Ed
4. Adrenal Function Tests
| Test | What It Measures | Significance |
|---|---|---|
| Serum Cortisol (8 AM and midnight) | Diurnal variation | Loss of diurnal variation = early sign of Cushing syndrome |
| Dexamethasone Suppression Test (DST) | HPA axis suppression | 1 mg dexamethasone at midnight; failure to suppress 8 AM cortisol confirms Cushing syndrome |
| ACTH stimulation test | Adrenal reserve | Used to diagnose Addison disease (primary adrenal insufficiency) |
| 24-hr urine cortisol | Total cortisol output | Elevated in Cushing syndrome |
5. Cardiac Biomarkers
| Test | Significance | Time Course |
|---|---|---|
| Troponin I / Troponin T | Gold standard for myocardial infarction; highly cardiac-specific | Rises 3-6 hrs after MI; stays elevated for 10-14 days |
| CK-MB (Creatine Kinase-MB isoenzyme) | Confirms MI when ECG non-diagnostic | Rises 4-8 hrs; returns to baseline in 48-72 hrs (faster than troponin) |
| LDL/HDL Cholesterol Ratio | Cardiovascular risk | High LDL:HDL ratio = increased atherosclerosis risk |
| BNP / NT-proBNP | Heart failure marker | Elevated with ventricular wall stress; guides heart failure diagnosis |
- Harper's Illustrated Biochemistry, 32nd Ed; Tintinalli's Emergency Medicine
6. Ascitic Fluid Biochemistry (Body Fluid Tests)
| Test | Significance |
|---|---|
| SAAG (Serum-Ascites Albumin Gradient) | Preferred over exudate/transudate: ≥11 g/L = portal hypertension (cirrhosis, heart failure); <11 g/L = non-portal cause (malignancy, TB) |
| Total Protein | Historical cutoff 25-30 g/L; less reliable than SAAG |
| LDH in ascites | High LDH associated with malignant effusions |
| Glucose | Decreased in infection/malignancy |
| Amylase | Elevated in pancreatic ascites |
| ADA (Adenosine Deaminase) | Elevated in TB peritonitis |
- Tietz Textbook of Laboratory Medicine, 7th Ed
7. Quick Reference: Common Reference Ranges
| Test | Reference Range |
|---|---|
| ALT | 7-56 U/L |
| AST | 10-40 U/L |
| ALP | 44-147 U/L |
| GGT | 8-61 U/L |
| Total Bilirubin | 0.2-1.2 mg/dL |
| Albumin | 3.5-5.0 g/dL |
| BUN | 10-20 mg/dL |
| Serum Creatinine | 0.5-1.0 mg/dL (varies by sex) |
| TSH | 0.4-4.0 mIU/L |
| Troponin I | <0.04 ng/mL (high-sensitivity assays lower) |
Key Concept - Pattern Recognition: The real clinical value of biochemical tests lies in interpreting the pattern of abnormalities together, not any single value in isolation. For example, isolated ALP + LDH elevation points to a space-occupying liver lesion, while AST/ALT elevation with normal albumin and ammonia points to acute hepatitis rather than cirrhosis.
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods; Harper's Illustrated Biochemistry 32nd Ed; Tietz Textbook of Laboratory Medicine 7th Ed; Barash's Clinical Anesthesia 9e
Biochemical test for microorganisms
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Excellent content gathered. Here is the comprehensive answer:
Biochemical Tests for Microorganisms
Biochemical tests exploit differences in enzyme activity, metabolic pathways, and substrate utilization to identify and differentiate microorganisms. They form the backbone of classical bacteriology and are still widely used alongside newer molecular and mass spectrometry methods.
The Core Principle
Each microorganism has a unique enzymatic and metabolic fingerprint. By exposing an organism to specific substrates and detecting the products (color changes, gas production, pH shifts), it is possible to assign genus and species identity.
Gram-Positive Cocci - The Key Algorithm
The catalase and coagulase tests are the two most used rapid tests for Gram-positive cocci identification:
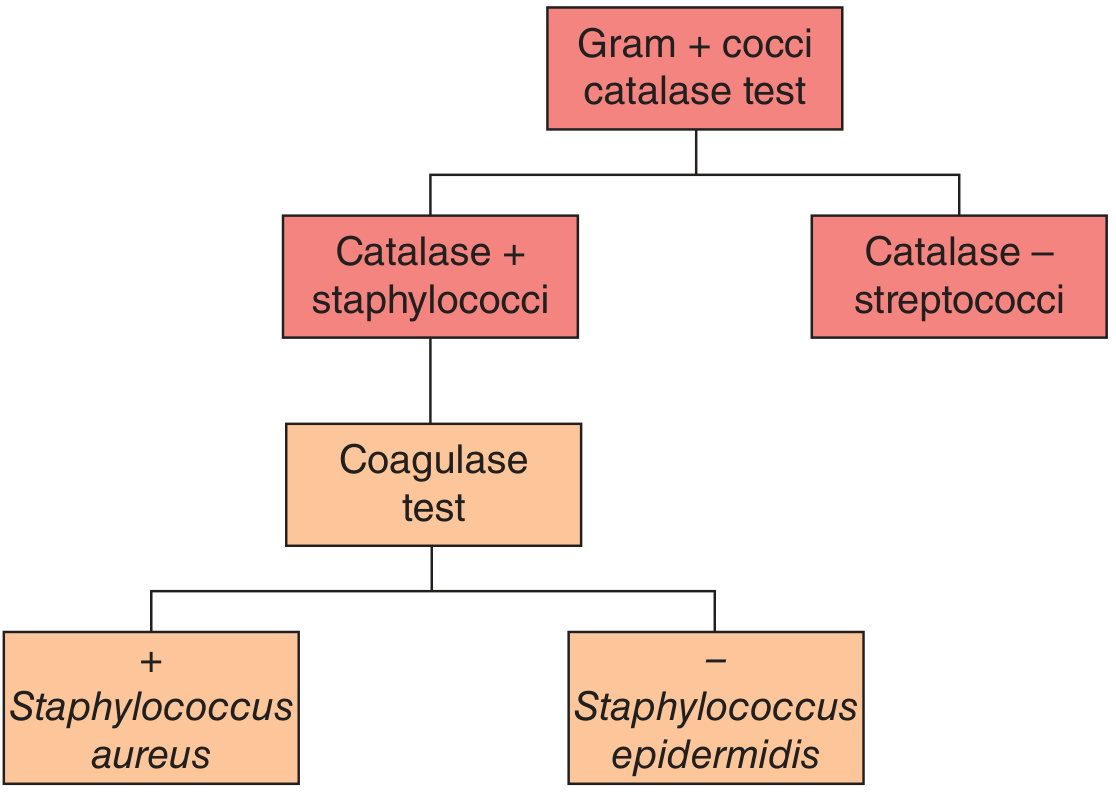
Algorithm for differentiating Gram-positive cocci - Jawetz, Melnick & Adelberg's Medical Microbiology 28e
The 14 Standard Biochemical Tests
1. Catalase Test
- Principle: Catalase enzyme converts H₂O₂ → H₂O + O₂ (visible bubbles)
- Method: Add a drop of 3% hydrogen peroxide to a colony on a glass slide
- Positive result: Rapid bubbling/effervescence
- Key use:
- Differentiates Staphylococcus (catalase +) from Streptococcus (catalase -)
- Also positive: Micrococcus, Campylobacter, Listeria, Bacillus
- Note: Do NOT use blood agar - blood can cause false positives
2. Coagulase Test
- Principle: Coagulase enzyme + plasma factor → converts fibrinogen to fibrin clot
- Two methods:
| Method | Detects | Reading time | Notes |
|---|---|---|---|
| Slide coagulase | Bound coagulase (clumping factor) | Seconds/minutes | Faster, but needs confirmation |
| Tube coagulase | Free coagulase (clot in tube) | 4 hrs (check again at 24 hrs) | Definitive; gold standard |
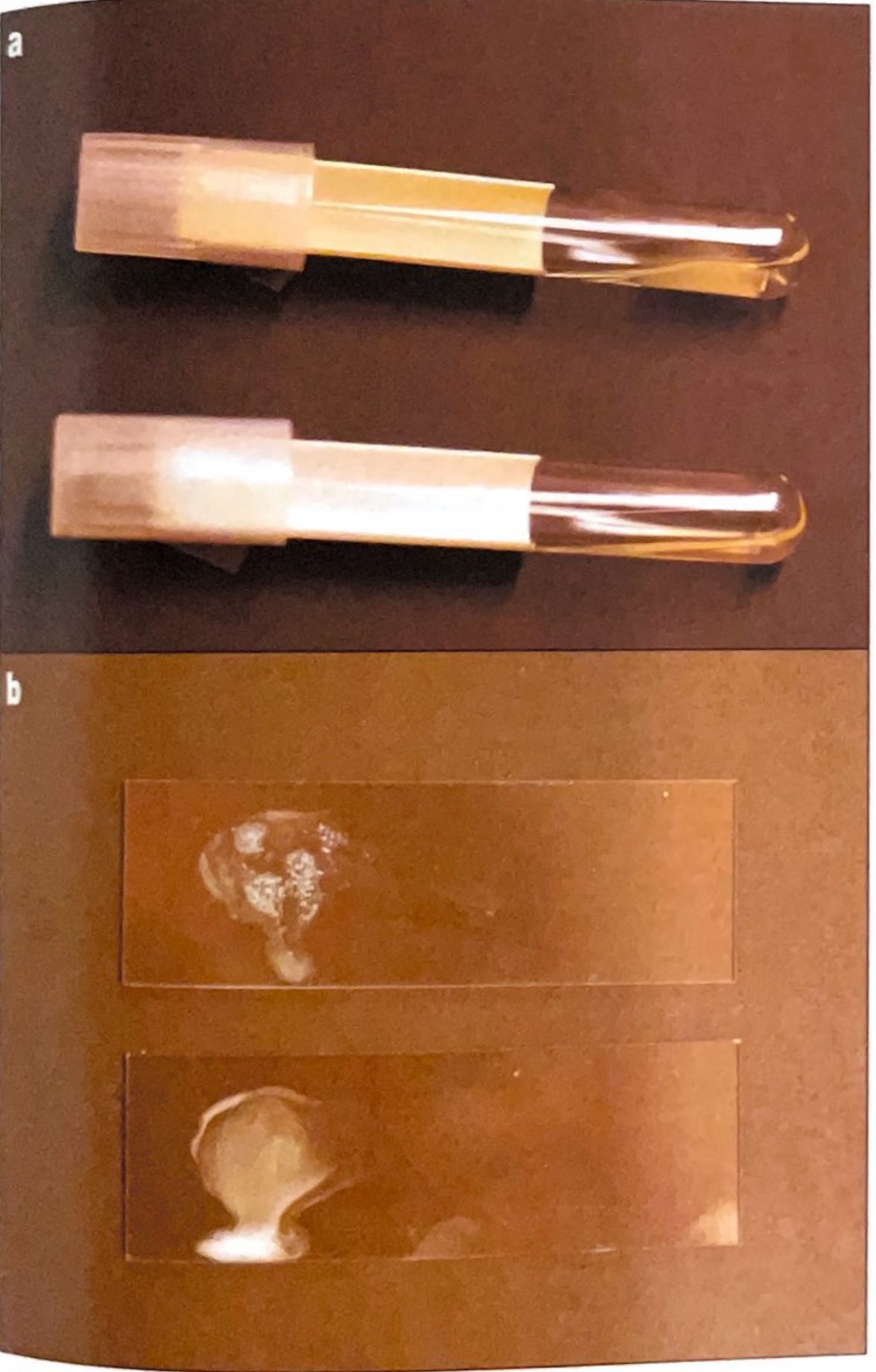
Coagulase test: tube coagulase (a) and slide coagulase (b). Top = positive, bottom = negative.
- Coagulase +: Staphylococcus aureus
- Coagulase -: S. epidermidis, other CoNS
- Note: S. lugdunensis is slide coagulase positive but tube coagulase negative
3. Oxidase Test
- Principle: Detects the cytochrome c oxidase enzyme component (part of electron transport chain)
- Method: Reagent changes from colorless → blue/purple when oxidized
- Positive result: Blue/purple pigment within seconds
- Key use: Initial classification of Gram-negative rods
- All Enterobacterales (e.g., E. coli, Klebsiella, Salmonella, Shigella) are oxidase NEGATIVE
- Oxidase POSITIVE organisms: Pseudomonas aeruginosa, Neisseria, Campylobacter, Vibrio
- This single test separates the entire family Enterobacterales from other Gram-negative rods
4. Urease Test
- Principle: Urease hydrolyzes urea → 2 NH₃ + CO₂; ammonia raises medium pH
- Result: Pink/red color change (alkaline shift)
- Organisms:
- Rapid (within 4 hrs) urease positive: Proteus spp., H. pylori
- Positive: Klebsiella, Helicobacter, Ureaplasma
- Negative: E. coli, Salmonella
- Clinical use: CLO test (Campylobacter-Like Organism test) is the bedside rapid urease test for H. pylori on gastric biopsy
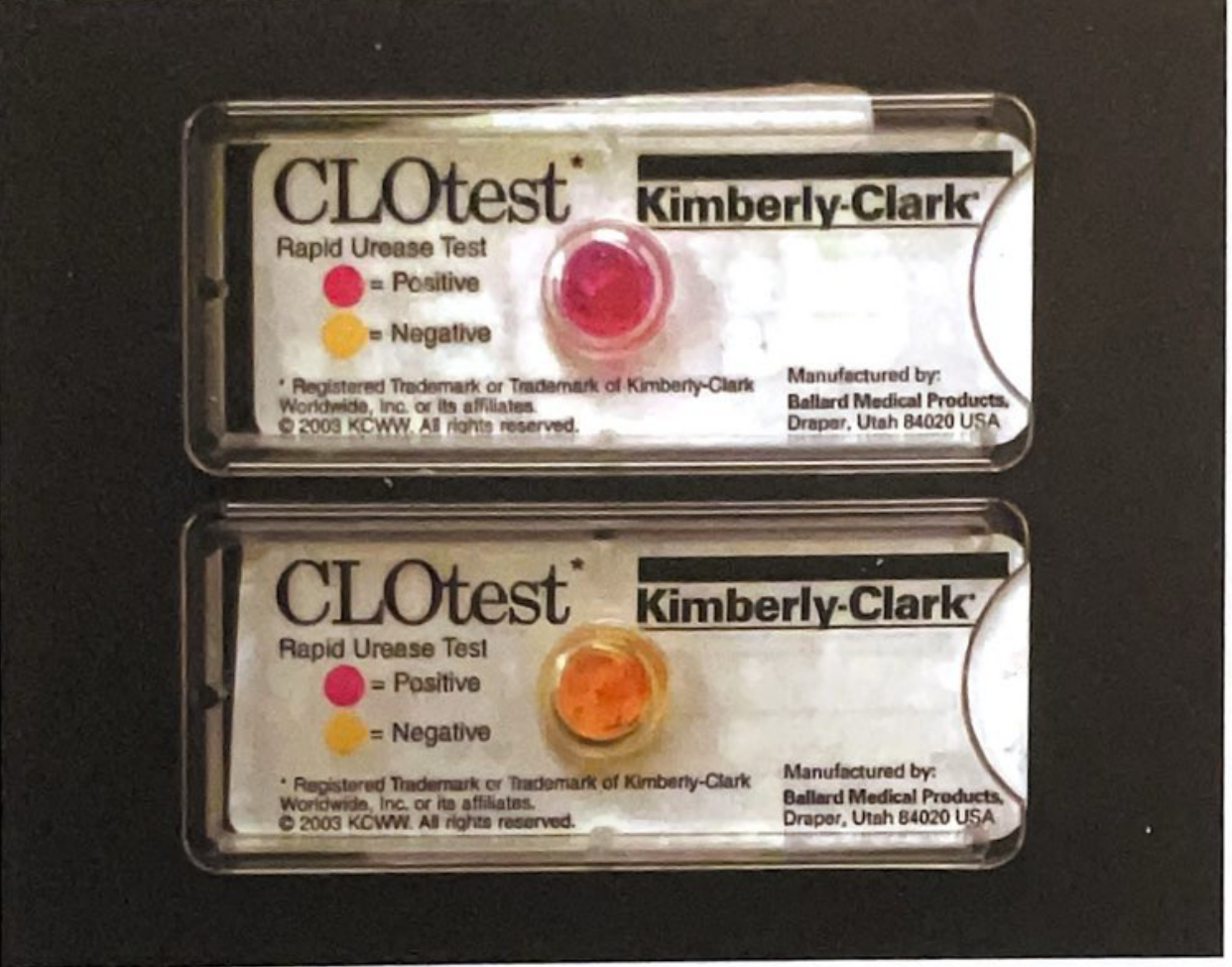
CLOtest Rapid Urease Test: positive = pink/red (top), negative = yellow/orange (bottom)
5. Indole Test
- Principle: Tests ability to split indole (a benzopyrrole) from tryptophan
- Detection: Addition of Kovacs' reagent (p-dimethylaminobenzaldehyde) → red ring at surface
- Positive organisms: E. coli, Proteus vulgaris
- Negative organisms: Klebsiella, Proteus mirabilis, Salmonella
- Can be done as a rapid spot test from isolated colonies in seconds
6. Methyl Red (MR) Test
- Principle: Detects stable acid end products from glucose fermentation via mixed acid pathway
- Method: Add methyl red indicator after glucose fermentation
- Positive result (red): Strong acid production - E. coli, Shigella
- Negative result (yellow): Little acid - Klebsiella, Enterobacter
7. Voges-Proskauer (VP) Test
- Principle: Detects acetoin (acetylmethylcarbinol), an intermediate in the butylene glycol fermentation pathway
- Method: Add alpha-naphthol + KOH → red color if acetoin present
- Positive organisms: Klebsiella, Enterobacter (VP+, MR-)
- Negative: E. coli, Shigella (VP-, MR+)
- The MR and VP tests are typically opposite for the same organism
Together with Indole and Citrate, MR and VP form the classic IMViC battery used to differentiate members of the Enterobacteriaceae family.
8. Citrate Utilization Test
- Principle: Tests ability to use citrate as the sole carbon source
- Medium: Simmons Citrate Agar (with bromothymol blue pH indicator)
- Positive result: Growth + blue color change (alkaline)
- Positive organisms: Klebsiella pneumoniae, Salmonella, Enterobacter, Citrobacter
- Negative organisms: E. coli, Shigella
9. Hydrogen Sulfide (H₂S) Production
- Principle: Some bacteria produce H₂S from sulfur-containing amino acids
- Detection: H₂S reacts with iron salts → black precipitate (ferrous sulfide)
- Positive organisms: Salmonella, Proteus, Citrobacter
- Negative: E. coli, Klebsiella
- Used in TSI (Triple Sugar Iron) agar along with fermentation reactions
10. Carbohydrate Fermentation Tests
- Principle: Acidic metabolic products from carbohydrate breakdown change pH indicators
- Sugars tested: glucose, lactose, sucrose, mannitol, maltose
- Key clinical example: Lactose fermentation differentiates coliforms from non-coliforms
- Lactose fermenters (pink colonies on MacConkey): E. coli, Klebsiella
- Non-fermenters (colorless on MacConkey): Salmonella, Shigella, Pseudomonas
- Gas chromatographic detection of short-chain fatty acids from glucose fermentation is useful for anaerobic bacteria classification
11. Nitrate Reduction Test
- Principle: Detects bacterial reduction of nitrate → nitrite (or N₂ gas)
- Positive organisms: Most Enterobacteriaceae, Pseudomonas
- Clinical use: Nitrite dipstick in urinalysis detects Gram-negative UTI pathogens
12. ONPG Test (O-Nitrophenyl-β-D-Galactoside)
- Principle: Tests for presence of β-galactosidase enzyme
- Identifies organisms that have β-galactosidase but lack lactose permease - so they appear lactose-negative on standard media but are ONPG positive
- Example: Late lactose fermenters like Shigella sonnei
13. Decarboxylase / Deaminase Tests (Lysine, Ornithine, Arginine)
- Principle: Amino acid decarboxylation produces amines → alkaline shift detected by pH indicator
- Key example: Lysine decarboxylase positive = Klebsiella, E. coli
- Used primarily with Gram-negative rods
14. PYR Test (Pyrrolidonyl Arylamidase)
- Principle: Rapid colorimetric test; positive = pink to red color change
- Key organisms: Identifies Group A Streptococci (S. pyogenes), Enterococci, and S. lugdunensis
- Fast, can give presumptive ID from colonies within minutes
IMViC Summary Table (Enterobacteriaceae Differentiation)
| Organism | Indole (I) | Methyl Red (M) | Voges-Proskauer (V) | Citrate (C) |
|---|---|---|---|---|
| E. coli | + | + | - | - |
| Klebsiella pneumoniae | - | - | + | + |
| Enterobacter | - | - | + | + |
| Proteus vulgaris | + | + | - | - |
| Salmonella | - | + | - | + |
| Shigella | - | + | - | - |
Oxidase-Based Gram-Negative Classification
| Oxidase Result | Organisms |
|---|---|
| Oxidase Negative | All Enterobacterales: E. coli, Klebsiella, Salmonella, Shigella, Proteus, Enterobacter |
| Oxidase Positive | Pseudomonas, Neisseria, Campylobacter, Vibrio, Moraxella, Brucella |
Modern Automated Methods
Classical biochemical tests are now often bundled into:
| System | Type | How it works |
|---|---|---|
| API panels (e.g., API 20E) | Manual | Multiple mini-wells with different substrates; incubate then enter results into database |
| Vitek 2 | Automated | Instrument inoculates panel, reads fluorescent reactions, gives ID + susceptibility |
| MicroScan WalkAway | Automated | Similar to Vitek; walkaway automation |
| MALDI-TOF MS | Mass spectrometry | Protein fingerprint of organism matched to database; rapid, highly accurate - may replace conventional biochemical testing |
MALDI-TOF limitations: Works best on cultured organisms (not direct specimens); poor discrimination between closely related species (e.g., E. coli vs Shigella); relies on database representation.
Quick Organism-Test Summary
| Test | Organism Identified | Result |
|---|---|---|
| Catalase | Staph vs Strep (Gram+ cocci) | Staph = + |
| Coagulase | S. aureus vs CoNS | Aureus = + |
| Oxidase | Enterobacterales vs non-Enterobacterales | Enterobacterales = - |
| Urease (rapid) | H. pylori, Proteus | Positive = pink/red |
| Indole | E. coli vs Klebsiella | E. coli = + |
| Citrate | Klebsiella vs E. coli | Klebsiella = + |
| H₂S | Salmonella vs E. coli | Salmonella = + |
| PYR | Group A Strep, Enterococci | Positive = pink-red |
Sources: Sherris & Ryan's Medical Microbiology, 8th Ed; Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed; Quick Compendium of Clinical Pathology, 5th Ed
Can you give book pdf of cruckshank book micro
I'm not able to provide a PDF of Cruickshank's Medical Microbiology (or any copyrighted textbook). Sharing or distributing copyrighted book PDFs would be a copyright infringement, regardless of the source.
Here are legitimate ways to access it:
How to Get Cruickshank's Medical Microbiology Legally
1. Library Access
- Check your university or medical college library - most institutions hold physical or digital copies
- Ask your librarian for interlibrary loan if not available locally
2. Purchase
- Search on Amazon, AbeBooks, or local medical bookstores
- Second-hand copies are often available at low cost on AbeBooks
3. Online Legal Platforms
- Google Books - often has partial previews
- Open Library (Internet Archive) - older editions may be available for free borrowing
- WorldCat - find the nearest library holding a copy
4. Institutional Access
- If you are a student, check if your institution subscribes to ClinicalKey, AccessMedicine, or Elsevier platforms
Note: The full title is "Medical Microbiology" by Cruickshank, Duguid, Marmion & Swain. Older editions (e.g., 12th) may be available through Internet Archive for free borrowing as they are out of print.
Is there a specific topic from Cruickshank you need help with? I can answer questions directly from the medical library I have access to.
This is a shared conversation. Sign in to Orris to start your own chat.